Article Text

Statistics from Altmetric.com
Key messages
During the SARS-CoV-2 pandemic, conventional cervical cytology (Pap smear) screening flexible-timing invitations were changed to fixed-timing invitations to ensure social distancing.
Due to the scheduling change, the number of tests conducted per hour decreased from 4.1 (July–December 2019) to 3.6 (July–December 2020).
Nevertheless, the lockdown backlog was successfully addressed through a substantial, but sustainable, reorganisation of obstetrician activities, obtaining performances comparable to 2019.
Why was change needed?
By the end of January 2021, almost 100 million people were infected with SARS-CoV-2 and over two million had died.1 Disruptions in healthcare delivery occurred in most countries as a direct consequence of the pressures posed by overwhelming numbers of COVID-19 cases, and as an indirect effect of strict infection containment measures such as social distancing and lockdowns.2
Italian regions halted cervical screening programmes in March 2020, for about 4 months, when only follow-up colposcopies were guaranteed.3 In the province of Ancona, primary conventional cervical cytology (Pap smear) screening was suspended from 9 March to 30 June 2020 as its organisation did not guarantee social distancing.4 Indeed, the programme was based on flexible-timing invitations: assuming an average 50% participation, more women than the available time slots were invited, without strict timings or having to confirm their appointment.5 This implied the possibility of overcrowding in waiting rooms.
The pandemic posed a double challenge: while flexible-timing was eliminated to ensure social distancing, a greater number of tests was needed to clear the 16-week backlog. The adopted strategies differed greatly across Italian regions: several already used fixed appointments (with a precise date and time in the invitation letter, in accordance with national recommendations)6 and only had to allocate more time for each test in order to avoid overcrowding. Most of the other regions, which used flexible-timing, moved to fixed appointments, and some programmes required the women to book their Pap smear to avoid last-minute rescheduling and missed tests.3
How was change implemented?
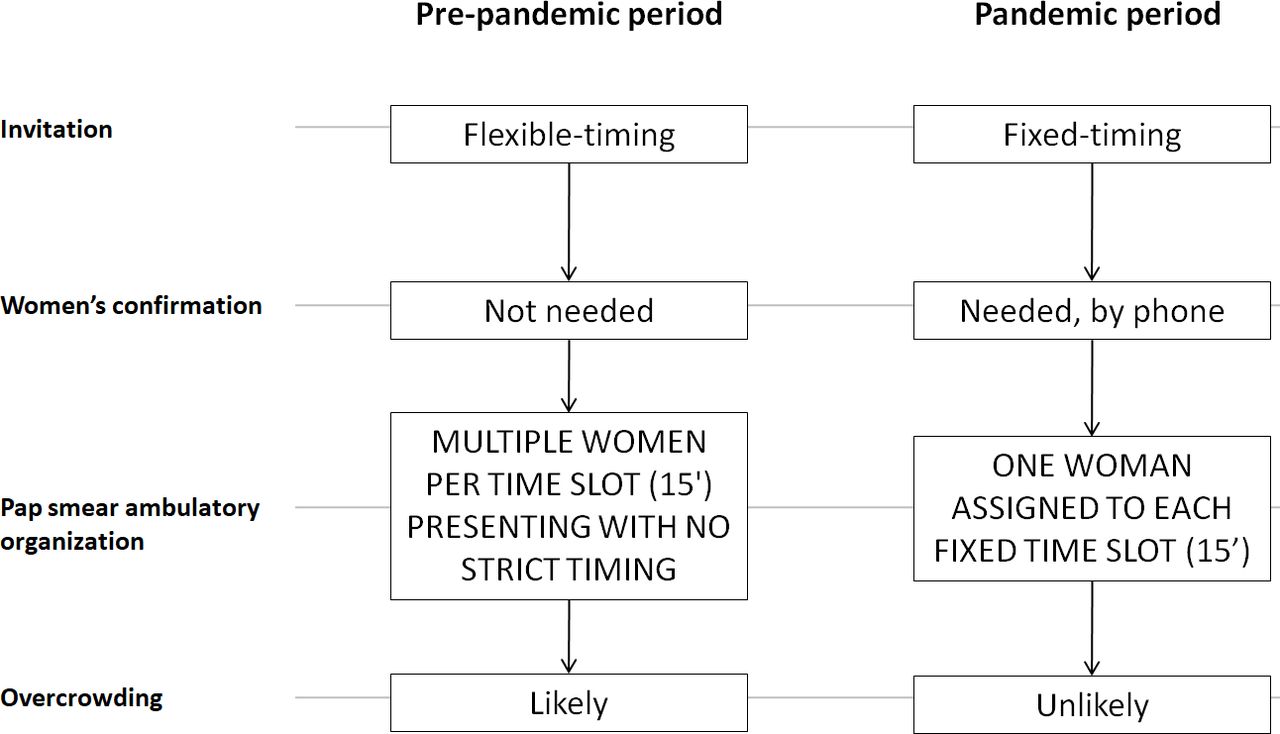
The regional Healthcare Directorate commissioned a survey of provincial screening programmes to determine the number of tests needed in the remaining 6 months of 2020, with the resumption of screening in July 2020. Multidisciplinary group meetings were held to verify the availability of obstetricians and gynaecologists to provide additional clinic hours. After careful evaluation of the various timing strategies for screening tests, the Healthcare Directorate, in agreement with multidisciplinary groups and labour unions, decided to adopt fixed-timing invitations, allocating 15 min per Pap smear and 20 min per colposcopy (figure 1). The requirement to book a fixed appointment by telephone or email was included in invitation letters, and the software was revised in order to confirm only one woman per time slot. The additional obstetricians’ work hours were obtained through the shift of most of their tasks to Pap smear execution, reducing comprehensive maternal health interventions (eg, home visits for breastfeeding education) or (re)scheduling activities (entirely assigned to the call centre staff). Gynaecologists’ supplementary activity was instead ensured through the increase in total work hours (80 vs 65 hours per month in 2020 vs 2019).
{kind=link}
Flow charts outlining the organisation of the Pap smear screening activity in the pre-pandemic and pandemic periods.
How did we assess possible variations in cervical screening activity?
We collected the number of work hours and Pap smears performed during 2019 and 2020, overall and by semester, and computed the hourly rate of tests and the percentage changes from 2019 to 2020. An additional stratification was made for the period 1 January–8 March 2020 to explore differences from the pre-lockdown period. With regard to the expected workload, given a stable 43 100 total invitations per year (≈414 Pap smears per week with a 50% uptake), the 16-week lockdown was expected to result in 6631 missed tests, to be performed during the 26 weeks from July to December 2020, in addition to the 10 775 planned tests (+61.6%; 669 vs 414 tests per week).
There was no direct participation of patients in the study. The analyses were performed using STATA 15.1 (2017; Stata Corp., College Station, TX, USA).
What outcomes resulted from the change in practice?
The effect of the suspension of cervical screening is apparent: from 1 January to 8 March 2020, 4411 Pap smears were performed throughout the province (vs 4883 in 2019), and none during the rest of the first semester (vs 7532 in 2019).
As a consequence, work hours almost doubled in the period July–December 2020 compared with July–December 2019 (93.1% increase; 3445 vs 1784 hours), while the number of Pap smears increased by 70.3% (12 349 vs 7252; table 1), exceeding the 61.6% threshold required to address the backlog.
Hours of obstetrician activity for primary Pap smears, Pap smears performed, and rate of Pap smears per hour for 2019 and 2020, overall, by semester, and for the periods 1 January–8 March and 9 March–30 June 2020, with percentage changes
Notably, however, the comparison between the second semesters (2019 and 2020) is unbalanced: in 2019, the tests that remained to be performed in the second semester were many fewer than those performed in the first semester (7252 vs 12 415, respectively; table 1). Also, overall 2020 screening participation was 14.8% lower than in 2019, which helped with the backlog resolution.
Given this, it is still remarkable that in the second semester of 2020, despite the flexible- to fixed-timing switch, which inevitably increased the mean test duration from 12.0 to 16.7 min (maximum four tests per hour; table 1), almost the same number of Pap smears were performed as in the first semester of 2019 (12 349 vs 12 415, respectively). To achieve this, the work hours devoted to the screening increased sharply, from a total of 2498 in the first semester of 2019 to 3445 in the second semester of 2020 (+37.9%).
In 2020, with fixed-timing scheduling, fewer than four Pap smears were performed per hour. Therefore, despite the full booking of all time slots, almost 10% of the appointments were missed. Nonetheless, 10% missed Pap smears is a positive performance, considering that some women are forced to reschedule because of irregular menstruation.
Finally, higher satisfaction was reported by the obstetricians, whose planning became easier, and by the users, whose role in the process became more active. The Ancona province is thus considering maintaining the current organisation of the Pap smear programme in the long term.
What advice could be given to others who might be considering a similar course of action?
First, clinicians devoting additional hours to screening was key to minimising SARS-CoV-2 infection risk, as fixed-timing tests are necessarily slower paced. Second, call centre staff promptly managed a sudden surge of calls and emails, while management monitored the volumes of invitations, preventing programme overload. Importantly, owing to its awareness of the preventive impact of screening programmes, the Healthcare Directorate coordinated this multidisciplinary effort at the regional level.
Also, while the fixed-timing modality obtained optimal performances, possible explanations for the apparent reduction in uptake could be the lockdown (and the women’s possible residual fear of infection even afterwards)4 or the modality update itself. Indeed, earlier studies found that fixed-timing invitations are likely to reduce uptake compared with flexible-timing ones.6
Furthermore, local characteristics should be borne in mind: for example, larger waiting rooms might accommodate multiple women, allowing the performance of more hourly tests. Naturally, all other precautions, such as using personal protective equipment, will need to be observed at all times.
What additional improvements could be made?
With the fixed-timing invitation modality, if a woman misses her 15-min time slot, no one else can use it. Therefore, efforts should be directed at optimising Pap smear use, for example, through automatic SMS reminders, which are currently under consideration in the province.7 Also, to further reduce the risk of SARS-CoV-2 infection, viable options could include human papillomavirus (HPV) test self-sampling and telecolposcopy.4
Self-sampling, proposed initially as a strategy to increase participation of underscreened populations, was recently found to be a cost-effective alternative to clinician-collected samples.8 Indeed, the reduced test sensitivity is counterbalanced by a greater screening uptake. During the COVID-19 emergency, many countries are considering the use of HPV self-sampling to decrease users of outpatient clinics and increase screening participation.4 9 Examples have been described in Australia, where some programmes mailed kits to women at the request of their provider following a telehealth consultation.10
The Ancona province is projected to transition to HPV testing in 2022, and thereafter from 3-year to 5-year screening intervals, eventually reducing contacts between clinicians and users. In this context, the use of remote technology coupled with self-sampling (probably mailed at the women’s request for those who prefer this method to clinician-collected sampling) could increase uptake, while optimising resource allocation.
What additional research is needed?
The COVID-19 emergency has compelled providers of sexual and reproductive healthcare worldwide to adapt services in order to minimise infection risk.11 In our case, close monitoring of the updated invitation modality is required to confirm the changes in staff and user satisfaction, and to verify the apparent decrease in screening uptake and its possible causes. Moreover, in order to further mitigate the infection risk, the feasibility of widespread HPV self-sampling for routine screening will have to be evaluated.
Ethics statements
Patient consent for publication
Ethics approval
Due to the exclusively aggregated nature of the collected data, ethical clearance was not needed.
Acknowledgments
The authors thank Mrs Ioanna Tzafaridou and Mr Michele Pettinari for their assistance with data collection.
Footnotes
CAM and MM are joint first authors.
Contributors CAM and MM collected and analysed data, and drafted the manuscript. MEF, MP and GG assisted with the literature review and the critical appraisal of the manuscript. LM and FP assisted in drafting and critically appraising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.