Article Text

Statistics from Altmetric.com
Background
The National Health Service (NHS) has become unaffordable through no fault of its own. Advances in medical technology, increased availability of better treatments, and disease epidemiology have all contributed to this challenging situation. People are living longer and putting a strain upon the NHS with an increasing burden of chronic illness. Will the new White Paper, Equity and Excellence: Liberating the NHS,1 prove to be the salvation of the NHS?
Where have we come from?
We have grown accustomed to NHS restructuring every 3 years or so, but the current proposals suggest the biggest change in strategic direction since the inception of the NHS. Many of us have lived through general practitioner (GP) fundholding, followed by primary care groups (PCGs), only for these to be scrapped and replaced with primary care trusts (PCTs).
Historically, the provision of reproductive and sexual health has been poorly funded, and viewed as a ‘Cinderella service’. Despite this we understand only too well that the relatively small amounts of money spent in primary care to provide contraception and genitourinary medicine services have a significant impact upon the sexual health of those who receive the service and that this is regarded as an efficient use of scarce NHS resources.
How are we performing?
Community contraceptive services play a pivotal role in preventing unwanted pregnancies, the need for terminations or antenatal care and, in many instances, significant social support. Chlamydia screening and treatment reduces the number of women developing complications such as pelvic infection and ectopic pregnancy. The cervical screening programme with its army of primary care nurses has contributed to a significant reduction from 1433 to 960 cervical cancer deaths annually over the last 30 years.2 We have, however, struggled with equity of access to NHS-funded assisted reproductive technologies (ART), with PCTs using clinical and/or social criteria (e.g. child in a previous relationship) variably across the UK to restrict access.3
The primary care focus to move patient care ‘closer to home’4 has resulted in more services being offered in the community. Increasingly, patients may seek help from a number of health care providers or general practices with overlapping practice boundaries. We have seen the development of specialist outreach services and partnership working between different organisations, all of which have contributed to improved patient access to care.
Many long-acting reversible contraceptives (LARCs) are now provided under ‘Local Enhanced Service’ arrangements for GP practices, thus recognising the need to invest in effective services locally. General practice has well-established structures and procedures in place to deliver sexual health services for patients within their community, including detailed and fully computerised patient records, robust monitoring systems, clinical audit, a well-developed mandatory system of appraisal (soon to be linked to GP revalidation), and quality assurance in terms of staff training and qualifications. The Faculty of Sexual and Reproductive Healthcare (FSRH) contributes significantly to the success of general practices’ ability to deliver these services through the training programmes linked to its Diploma (DFRSH) and Letters of Competence for Intrauterine Techniques (LoC IUT) and Subdermal Implants (LoC SDI).
The cited examples of successful sexual health services delivered in primary care have a cost implication in that setting but deliver a reduced cost burden in the secondary care setting, through a reduction in associated morbidity.
Where are we going now?
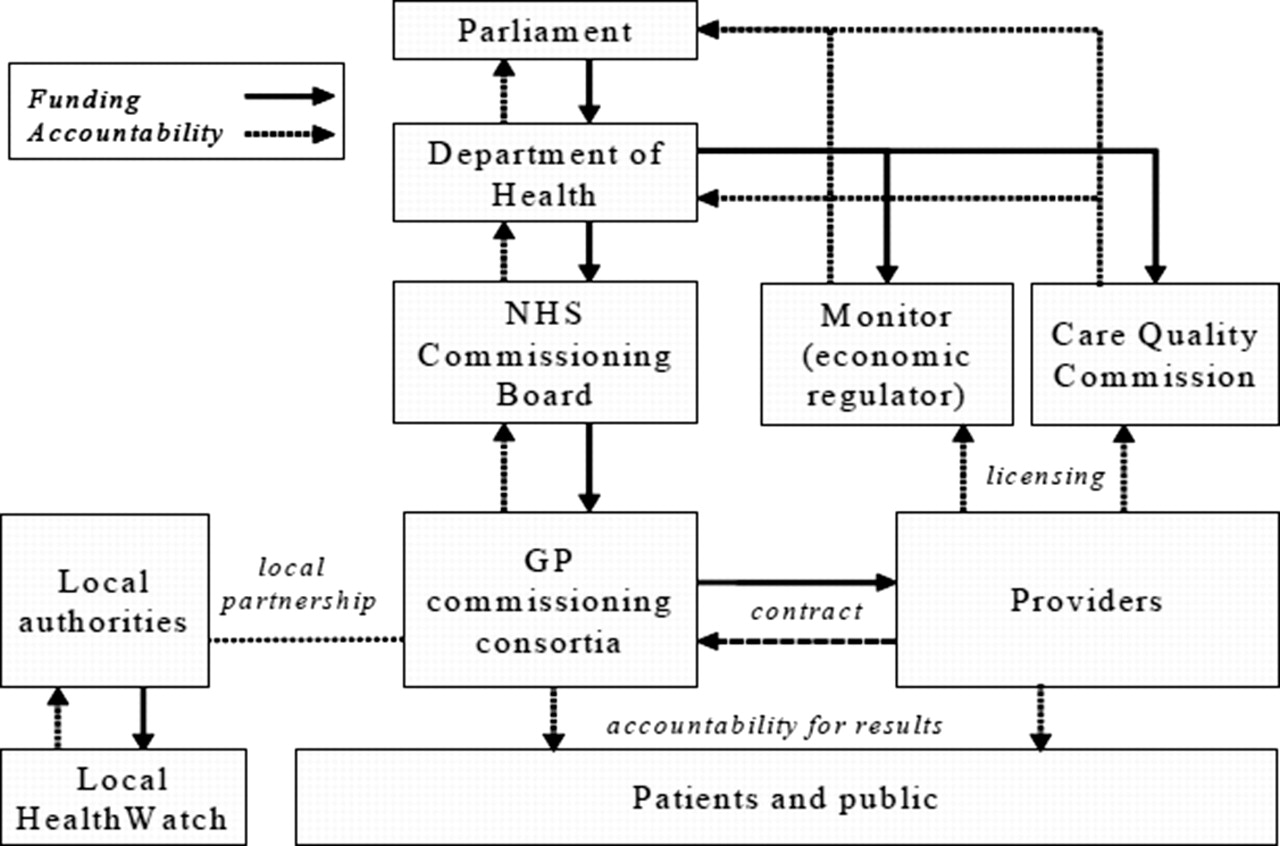
Andrew Lansley, Secretary of State for Health, is scrapping Strategic Health Authorities (SHAs), PCTs, and half of the quangos including the Health Protection Agency (HPA) and Human Fertilisation and Embryology Authority (HFEA). The PCTs are being replaced with approximately 500 GP commissioning consortia, which represents a three-fold increase in commissioning bodies, each of which will be cherry-picking the best managers from within PCTs or obtaining the skills from the private sector to help lead their organisations. Sitting above the GP commissioning consortia will be one NHS Commissioning Board, the function of which has yet to be clarified (Figure 1).
{kind=link}
New National Health Service (NHS) structure. Reproduced from Equity and Excellence: Liberating the NHS. © Crown Copyright
What is clear is that the function of commissioning is a distinctly separate process to the primary care services provided by our GP colleagues. GP providers will be competing against other health care providers, pitching their business case to the commissioning organisation in order to win contracts. The commissioning organisations are to be run by GPs from practices within their consortia. Strategic decisions will be made by those GPs, resulting in a potential conflict of interest as GP practices will be expected to offer their services within an agreed price framework to prevent excessive profit. This presents a dilemma and a new challenge for our GP leaders. Although clinical leadership does exist within the GP community to deliver this change, there is limited enthusiasm and a lot of scepticism among GPs.5 It is, however, the responsibility of each practice to influence the process within their consortia. What is paramount is that patient outcomes, patients’ needs and the quality of patient care are central to the commissioning function.
What are the risks?
The changes proposed in the White Paper are not without risk. There will be a significant cost in delivering this change, which will include the redundancy of PCT staff and re-employment of commissioners from within the current pool to deliver the commissioning function on behalf of their consortia. There will be significantly more GP commissioning consortia than there are currently PCTs. Local structures, relationships and some organisational memory may be lost. If GP commissioning is not successful then it will be open to private health care commissioning. It is likely that we will also see an increasing role for commercial organisations providing health care in all sectors of the NHS (Figure 1).
Reproductive services are currently commissioned supra-regionally and appear to have no home in the new structure. If it is organised at the micro-management level of GP consortia, this risks destabilising small local budgets leading to erratic delivery of services with resultant inequity across the UK. The current ‘postcode lottery’ that we experience may become worse.
We are led to believe that failing commissioning consortia will not be ‘bailed out’ and will not be able to apply to a central subvention fund to mitigate against unusual but financially crippling events. This is clearly not practical and this level of commissioning detail is not apparent yet. We do know that the Government will not underwrite any PCT debts accumulated during the transition phase up to 2013, so it is imperative that the GP consortia become operational as soon as practicable.
The future: opportunity or poisoned chalice?
Commonly a change in strategic direction in an organisation requires financial investment. In the White Paper, GP commissioning consortia are expected to commission health services and deliver the new structure on a budget reduced by approximately £20 billion through efficiency savings by 2014. GP commissioners need to be cautious for three reasons: first, we are on shifting sands as this is unlikely to be the last change we see; second, we are expected to deliver the changes on a significantly reduced budget; and third, it is likely that we will inherit the PCT debts on the lead up to their complete dissolution in 2013. It would have been nice to have taken up the reins before the horse had bolted! Despite this, GPs may prove to be the salvation of NHS commissioning with their culture of seeing themselves as the gatekeepers of the NHS and managing as much as possible in the primary care setting, resorting to specialist services only for those who really need them.
The White Paper provides a great opportunity for the development and commissioning of services that reduce the disease burden on secondary care services through effective primary prevention programmes and services.
Given the above, it would be good to think that the commissioning opportunities presented by the White Paper will allow the GP commissioners of the future to build upon and consolidate existing sexual health services, building these services around patient need and ‘care closer to home’. The shift of some services from secondary to primary care should continue, whilst ensuring that the services are of the highest quality and delivered by appropriately trained staff.
Of course, ensuring first–class sexual and reproductive health services in the future will require understanding and wisdom from those commissioning the services. This is a great opportunity as the commissioners are those professionals closest to the patient. Given the long-term public health arguments presented above, this can only be money well spent. There will, inevitably, be a responsibility placed upon the champions already working in these services to make sure they are given the priority they deserve.
In an ideal world there would never be an unwanted pregnancy, cervical cancer would be eliminated, sexually transmitted infections would become a thing of the past and assisted reproduction would be freely available. Approaching these ideals is undoubtedly the direction of travel and, whilst unachievable, these are some of the sexual health standards by which the commissioners will be judged. Good luck!
Acknowledgments
The authors would like to thank Shona Haining, Head of Research and Development, NHS North of Tyne Primary Care Trust, for helpful comments on this submission.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.