Article Text

Statistics from Altmetric.com
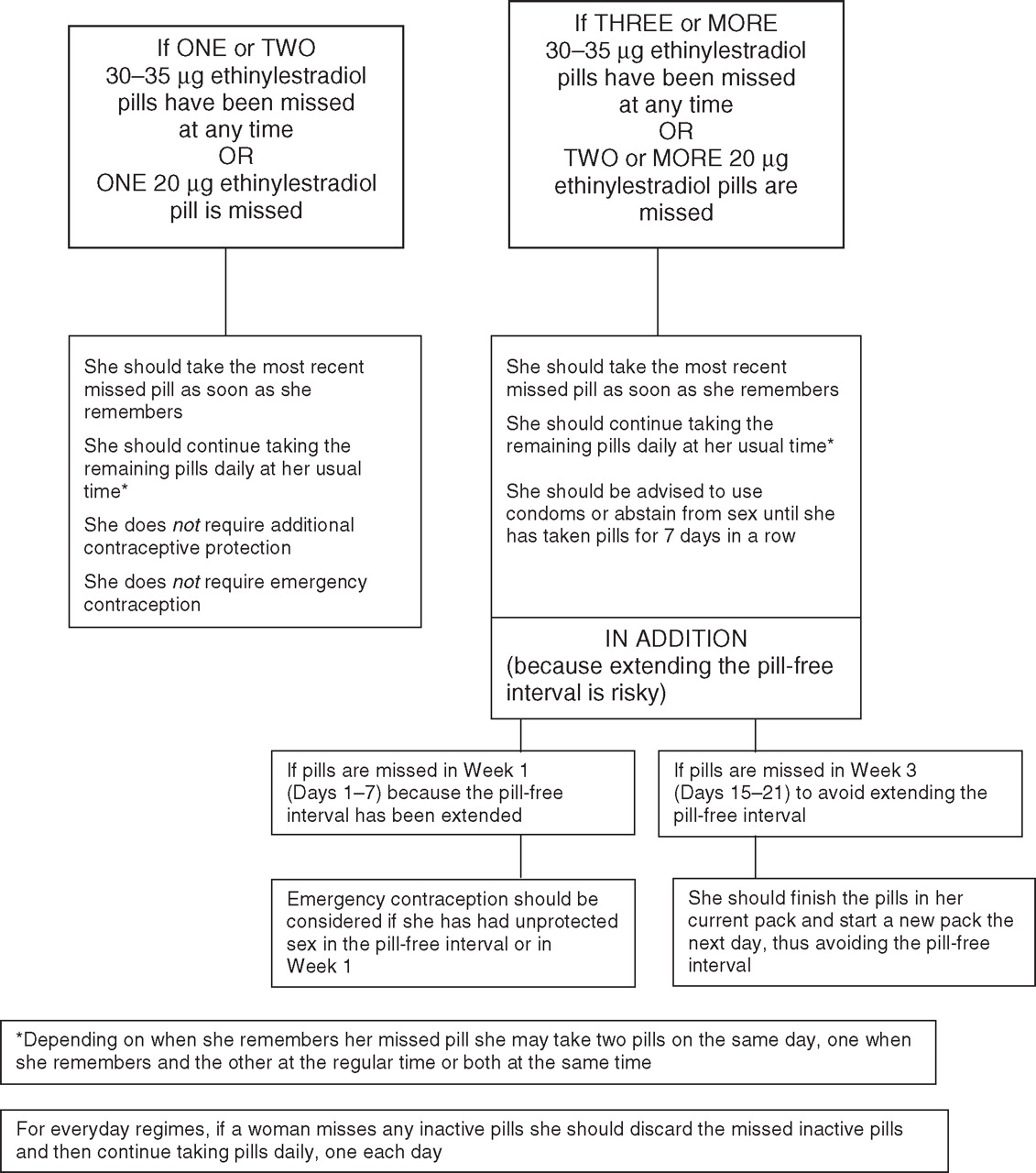
In 2005, the Clinical Effectiveness Unit (CEU) of the then Faculty of Family Planning and Reproductive Health Care adopted the World Health Organization (WHO) ‘missed pills’ guidance (Figure 1).1 Many clinicians criticised this change2,–,5 as these new rules appeared to be complex and caused confusion at the grass roots level.6,–,8 There were also concerns that liberalising the ‘missed pills’ guidance (Box 1)9 would lead to additional unplanned pregnancies among pill-takers and did not support safer sex messages or the importance of correct and consistent pill-taking.2 3 5

{kind=link}
Advice from 2005 for women missing combined oral contraceptives (30–35 µg and 20 μg ethinylestradiol formulations).1
Box 1 ‘Missed pill’ rules in the Summary of Product Characteristics9
▶ If the forgotten tablet is taken within 12 hours, no further precautions are necessary, further tablets should be taken at the usual time.
▶ If one or more tablets are forgotten for more than 12 hours, contraceptive protection will be reduced. The patient should take the last forgotten tablet, even if this means taking two tablets in 1 day, and then continue to take tablets at the normal time. Additional contraceptive precautions should be taken for the next 7 days, and the patient should follow ‘the 7-day rule’.
Unfortunately the 2005 changes appeared to have been based on old papers since superseded.10,–,16 Even at that time there was evidence contradicting a relaxing of the rules.17,–,19 The CEU admitted they did not consider recently published evidence from 2003 and 2004,10 which was worrying as Pierson et al.19 demonstrated presumed ovulation in 13–19% of 30–35 μg triphasic pill-users following a 3-day dosing error thereby extending the pill-free interval.
Since then further evidence has been published suggesting that hormone-free intervals of 7 or more days can result in breakthrough ovulations and a significant increase in pill failure.20,–,22 One of the arguments posed suggested that even though studies reported higher ovulation rates, failure had not been linked with the ‘pill-free’ interval10 and these women did not become pregnant. However, it should be pointed out that women taking part in these studies used abstinence or barrier methods when pills were missed. Studies exploring ovarian follicular activity when extending the hormone-free interval include small numbers of women and are not powered to detect wide individual variation.23 Authors of a systematic review in 2006 acknowledged that these studies also gave varied definitions of ‘ovulation’ and this inconsistency questions their methodology.23 Accurate detection of ovulation requires frequent and detailed endocrine and ultrasonic evaluation.
The ‘missed pill’ guidance in combined hormonal contraceptives' Summary of Product Characteristics leaflets is overcautious, particularly if pills are missed mid-packet (Box 1).9 In 2010, the UK's Medicines and Healthcare products Regulatory Agency (MHRA) recognised that there was a need to simplify these rules. The MHRA organised a meeting with representatives from a number of key UK organisations including the Faculty of Sexual and Reproductive Healthcare (FSRH), the FPA (Family Planning Association) and the pharmaceutical industry. The aim was to produce standardised guidance on the starting of combined hormonal contraceptives and on ‘missed pills’, emphasising the need for regular pill-taking and not ‘missing pills’ around the pill-free interval.
The MRHA ‘24-hour missed pill advice’ (Box 2) is clear.24 No action needs to be taken until 24 hours or more has elapsed from the usual ‘pill-taking’ time. If this occurs, anywhere in the packet, the forgotten pill needs to be taken and the next pill when it is due – this may mean taking two pills in 1 day. No additional contraception is required.
Box 2 Medicines and Healthcare products Regulatory Agency (MHRA) combined oral contraception Combined Oral Contraceptive (COC) Pill Advice 201124
Starting the pill.
▶ You can start the pill any time in your menstrual cycle if you are sure you are not pregnant.
▶ If you start the pill on the first day of your period you will be protected from pregnancy immediately.
▶ You can also start the pill up to, and including, the fifth day of your period and you will be protected from pregnancy immediately.
▶ If you start the pill at any other time in your menstrual cycle you will need to use additional contraception, such as condoms, for the first 7 days of pill taking.
If you forget to take a pill or start a pack late
▶ Missing pills or starting the pack late may make your pill less effective. The chance of pregnancy after missing pills depends on when pills are missed and how many pills are missed. A pill is late when you have forgotten to take it at the usual time. A pill has been missed when it is more than 24 hours since the time you should have taken it.
▶ If you miss one pill anywhere in your pack or start the new pack 1 day late, you will still have contraceptive cover. However, missing two or more pills or starting the pack two or more days late (more than 48 hours late) may affect your contraceptive cover. As soon as you realise you have missed any pills, take the last pill you missed immediately. In particular, during the 7-day pill-free break your ovaries are not getting any effects from the pill. If you make this pill-free break longer by forgetting two or more pills, your ovaries might release an egg and there is a real risk of becoming pregnant.
▶ Follow the advice below. If you are not sure what to do, continue to take your pill and use additional contraception, such as condoms, and seek advice as soon as possible.
If you have missed one pill, anywhere in the pack:
▶ Take the last pill you missed now even if it means taking two pills in 1 day
▶ Continue taking the rest of the pack as usual
▶ No additional contraception needed
▶ Take your 7-day break as normal.
If you have missed two or more pills (i.e. more than 48 hours late), anywhere in the pack:
▶ Take the last pill you missed now even if it means taking two pills in 1 day
▶ Leave any earlier missed pills
▶ Continue taking the rest of the pack as usual and use an extra method of contraception for the next 7 days
▶ You may need emergency contraception – see below
▶ You may need to start the next pack of pills without a break – see below.
Emergency contraception
▶ If you have had unprotected sex in the previous 7 days and you have missed two or more pills (i.e. more than 48 hours late) in the first week of a pack, you may need emergency contraception. Get advice from your contraception clinic, family doctor, or a pharmacist about this.
Starting the next pack after missing two or more pills (more than 48 hours late)
If seven or more pills are left in the pack after the last missed pill:
▶ Finish the pack
▶ Have the usual 7-day break.
If less than seven pills are left in the pack after the missed pill:
▶ Finish the pack and begin a new one the next day (this means missing out the break).
If two or more pills are forgotten (more than 48 hours late) only the last ‘forgotten’ pill is taken and the next pill taken at the usual time – this may mean taking two pills in 1 day. Additional contraception is needed for the next 7 days. If there are fewer than seven pills left in the pack, the pack should be finished and a new pack started the next day missing out the break.
The ‘emergency contraception (EC)’ advice, however, is confusing. The MHRA suggest that only women “who have unprotected sex in the previous 7 days and have missed two or more pills in the first week of their pack” should seek advice about EC. What about those who have repeated unprotected sex from the start of the hormone-free interval? They could still receive EC. Improved wording would read that “women who have unprotected sex during the hormone-free interval or in the first week of pill taking AND have missed two or more pills in that first week should seek advice about emergency contraception”.
True pill failures still occur and recent data suggest that a standard 7-day hormone-free break is too long for a small number of women.22 25 Six years after the publication of the WHO ‘missed pill’ guidance26 and CEU adoption of these rules a seminal paper has been published that clearly demonstrates the importance of the hormone-free interval for contraceptive efficacy. The International Active Surveillance of Women Taking Oral Contraceptives study in the USA followed 52 218 women prospectively in a controlled, non-interventional manner.20 The aim was to analyse contraceptive failure in those taking oral contraceptives. Total oral contraceptive exposure was 73 269 woman-years and a total of 1634 unintended pregnancies occurred. On closer examination, only 229 (14%) of these pregnancies arose in women who reported that they had taken their pills as directed. In answer to a direct query, the study authors have also reported that ‘non-perfect’ use was most frequent among adolescents.27 When studying women of all age groups, those taking a 24-day regimen containing a progestogen with a long half-life were less likely to have an unplanned pregnancy compared with those taking a conventional 21-day regimen. The adjusted hazard ratio was 0.7 (95% CI 0.6–0.8). Importantly, this reduction of contraceptive failure was even more pronounced in adolescents.27 This ‘real life’ study of pill-users demonstrates the dangers of the hormone-free interval and points the way to further research into more flexible pill regimens where hormone-free intervals are decreased and overall efficacy improved.
References
Footnotes
-
Competing interests The author has received honoraria for lecturing, expenses for attending scientific conferences and research grants from a number of pharmaceutical companies including Bayer Schering Pharma, Schering-Plough Limited and Merck Sharp & Dohme Limited (MSD).
-
Provenance and peer review Commissioned; internally peer reviewed.