Article Text

Statistics from Altmetric.com
- Education And Training
- Family Planning Service Provision
- Natural Family Planning
- Reproductive Health Politics
- Service Delivery
- Historical
Background and guidance
The lactational amenorrhoea method of contraception (LAM) was formalised over 20 years ago1 and the Faculty of Sexual & Reproductive Healthcare (FSRH) guidance on postnatal sexual and reproductive health2 is clear:
“Women may be advised that if they are <6 months postpartum, amenorrhoeic and fully breastfeeding, the lactational amenorrhoea method (LAM) is over 98% effective in preventing pregnancy.
Women using LAM should be advised that the risk of pregnancy is increased if the frequency of breastfeeding decreases (stopping night feeds, supplementary feeding, use of pacifiers), when menstruation returns or when >6 months postpartum.”
Yet a recent survey3 found “particular inconsistencies” in the advice given to breastfeeding women in the UK that raises the risk of unplanned pregnancies. Practitioners seem to either dismiss LAM or give the impression that breastfeeding alone can work as contraception:
“I received contradictory advice from the midwife and GP [general practitioner] – the GP believed that breastfeeding was a safe form of contraception, whereas the midwife warned me that it wasn't (but didn't offer any alternatives).”
There was also evidence that many practitioners fail to give advice to breastfeeding women about what action to take when the LAM criteria no longer apply.
LAM, breastfeeding rates and getting guidance into practice
LAM is more than a highly effective, temporary and economical form of postpartum contraception. It can also help to improve breastfeeding rates,4 and hence maternal and child health. For this reason, attempts were made to increase health professional knowledge of LAM in North London, UK through the provision of brief training and the production of a local patient leaflet.5 Unfortunately it seems that most health professionals are still reluctant to tell women about this method of postpartum contraception. As is often the case, guidance is not enough. Practitioners need to be convinced that the guidance is sound and that it will achieve positive patient outcomes.6
Why are people wary of LAM?
Health professionals gave us various reasons for their wariness of LAM, which we discuss below. These responses were anecdotal, rather than systematically gathered, but we believe they are typical of the views held by many practitioners.
The public is also likely to be wary: 90% believe that the contraceptive effects of breastfeeding are a myth.7 LAM is not just a matter of breastfeeding, but the two are often conflated so public beliefs about effectiveness are probably similar to those of most health professionals.
1 “LAM is a natural method. Natural methods are notoriously unreliable.” Some natural methods of contraception are more reliable than others. The Standard Days Method (calendar-based) has a perfect use rate of 95%.8 PERSONA™ (a hormone-measuring device) is around 94% effective.9 The sympto-thermal/fertility awareness-based method requires specialist teaching but is 99.6% effective.8 ,10
LAM is probably the simplest natural method. It is easy to understand, is over 98% effective,10 does not require specialist teaching and has a strong evidence base.1 ,2 ,11
2 “One of my patients/friends/relatives/colleagues got pregnant while breastfeeding.” Breastfeeding alone is not reliable contraception. Further questioning usually reveals that the LAM criteria were not being met.
3 “I don't want women to use a method they're not happy with.” LAM should not be presented as the only postpartum contraceptive option. As for all contraception, the choice should lie with the user. Women should be given clear, unbiased information to help them choose the best contraception for them at this time.
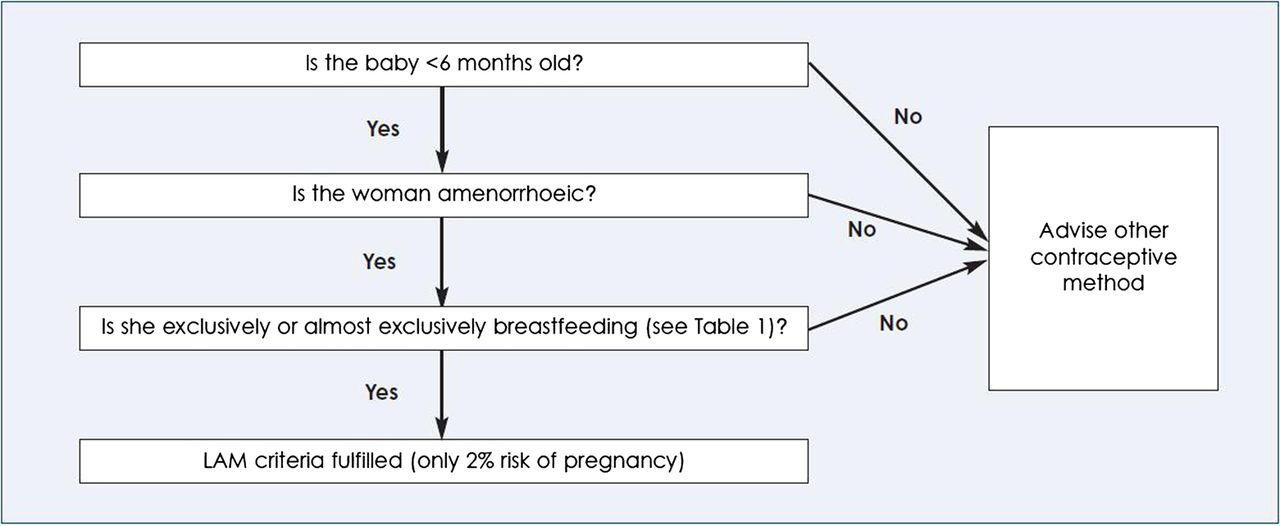
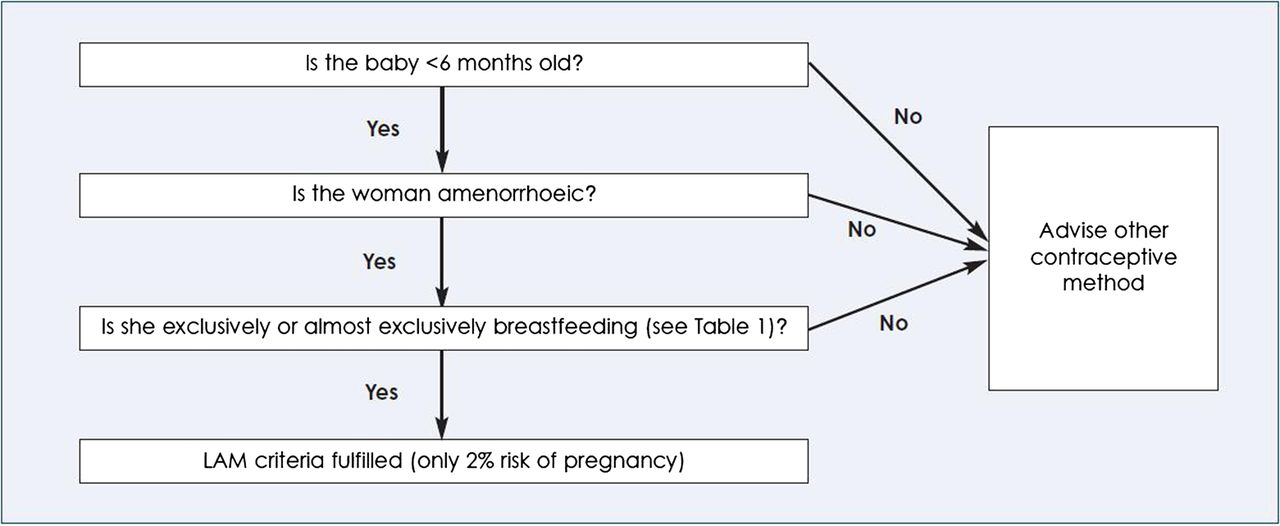
4 “It's too hard to explain.” The algorithm in the FSRH guidance helps (Figure 1),2 but national information for patients is inadequate at present. The widely-used National Health Service (NHS) Choices website simply states: “You can get pregnant as little as 3 weeks after the birth of a baby, even if you're breastfeeding and your periods haven't started”.12 A less prominent part of the website, and the fpa (Family Planning Association) leaflet ‘Contraception Choices – After You've Had Your Baby’,13 includes basic information about LAM but only states it is “up to 98% effective”, not over 98% effective, and does not include information about avoiding pacifiers. The Royal College of Obstetricians and Gynaecologists (RCOG)-endorsed magazine for pregnant women states: “fully breastfeeding does provide some protection but you should not rely on this as a secure form of contraception”.14
{kind=link}
Algorithm relating to use of the lactational amenorrhoea method (LAM).2
5 “We should encourage women to use the most reliable long-acting reversible contraceptive (LARC) methods, not less effective methods like LAM.” Information about LAM and its effectiveness should be given alongside the other postpartum options. Women using LAM are more likely to transition to another method than women who are breastfeeding without contraceptive intent,4 but they should be encouraged to plan so they are ready when LAM criteria no longer apply. An intrauterine device may not appeal to a woman a few weeks after giving birth but it could be a good option when her baby is 3 or 4 months old. Clinicians can be ‘reasonably certain’ that a woman meeting the LAM criteria is not pregnant,2 which simplifies the transition process.
6 “I don't want a patient coming to see me for a termination because I've told her to use a less reliable method.” No contraceptive method completely eliminates the risk of pregnancy. Women who are very concerned can be prescribed an additional method. However, some women are uncomfortable with other methods and so are unlikely to use them, even if they do have a better effectiveness rate. LAM is a good temporary option for these women.
7 “If a woman waits to have her period before switching to another method it's too late; the period means she'll have ovulated and so been at risk of pregnancy.” A woman cannot rely on amenorrhoea alone. Ovulation can occur as early as Day 28 for non-breastfeeding women. Initial cycles for breastfeeding women are associated with infertility as breastfeeding suppresses ovulation and shortens the luteal phase. Menstruation for this group occurs on average 28.4 (range 15–48) weeks after delivery and the mean time to ovulation is 33.6 (range 14–51) weeks.2
8 “Patients never listen. They just want pills.” Giving advice is not the easy option. Many clinicians will have encountered resistance from patients with a bad cold who want antibiotics rather than advice about rest, analgesia and antibiotic resistance. It is easier to provide advice when it is backed up with clear written information (see Response 4).
9 “It only applies to a tiny proportion of women.” In 2010, 81% of women began breastfeeding in the UK. Three months after delivery 17% of women were exclusively breastfeeding and at 5 months just 5%.15 This is not a large number of women, but good quality advice is essential at this time.2 ,3
10 “I don't want my patients to think I'm judging them.” Breastfeeding and parenting are sensitive subjects. Many parents use pacifiers or give formula milk as well as breast milk. It doesn't make them ‘bad parents’, it just means they can't rely on LAM.
11 “I'm not a breastfeeding expert; they might ask me tricky questions.” Breastfeeding has to be going well for LAM to be effective. If the patient needs breastfeeding support, refer them to their local infant feeding team or the National Breastfeeding Helpline (Tel: 0300 100 0212).
Concluding remarks
We need better national information for patients about LAM. This will help health professionals to provide clear and consistent advice, in line with the FSRH guidance. However, information for patients will not make a difference unless family planning practitioners, and those who rely on them for advice, trust the evidence.
Further research may be helpful, but the evidence base for LAM is strong. It is an effective temporary postpartum contraceptive option, it can help to improve breastfeeding rates, and there are almost no costs involved. Breastfeeding women should be routinely informed about all suitable methods of contraception and especially LAM, the 2% failure rate, and the need to have another contraceptive method ready for when any of the criteria change. Women should be receiving the same message whether they look at the NHS Choices website, or speak to their midwife, health visitor or family planning practitioner.
Footnotes
Competing interests The authors are both fertility awareness teachers and so have an interest in promoting methods that are based on recognising the physiological signs that indicate when a woman is fertile.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue