Article Text

Abstract
Polycystic ovary syndrome (PCOS) is the commonest endocrine disorder affecting women of reproductive age. Some 20% of women will have polycystic ovaries on an ultrasound scan and around 7% of women have the additional clinical or biochemical features of PCOS. As a complex multisystem disorder its background can be confusing to understand. They key feature, however, is an increased production of androgen by the ovaries. This review uses ovarian biology to describe a strategy to aid understanding and explanation of PCOS. This framework can be also be used to teach about PCOS and to inform different approaches to its management.
- polycystic ovary syndrome
Statistics from Altmetric.com
Key message points
-
Polycystic ovary syndrome (PCOS) is a common condition affecting 7% of women but its background can be confusing to understand.
-
The key feature is increased production of androgen by the ovaries.
-
Understanding ovarian biology clarifies pathways to androgen increase and provides a framework to facilitate teaching on PCOS.
-
This approach can be also used to inform management strategies.
Introduction
Polycystic ovary syndrome (PCOS) is the commonest endocrine disorder to affect women in their reproductive years. Around 20% of women have the characteristic appearance of polycystic ovaries on ultrasound scans1 and 7–8% have the additional clinical and biochemical features of PCOS itself.2 As obesity increases the proportion of women with polycystic ovaries who develop the syndrome, the current epidemic of obesity is likely to make PCOS even more common.3
Polycystic ovaries found on ultrasound scanning will often have no clinical effects, but PCOS is the most common diagnosis made in women presenting with amenorrhoea, oligomenorrhoea or heavy, irregular and prolonged periods. It is the commonest cause of hirsutism and of infertility due to anovulation. Women with PCOS have increased concentrations of circulating androgens and there is a marked association with insulin resistance, dyslipidaemia, obesity, gestational diabetes, type 2 diabetes and heart disease. In addition, it is an established cause of endometrial hyperplasia and it is therefore linked to endometrial cancer. The short- and long-term consequences of PCOS represent an increasing burden on health resources.
In recent years there has been increasing consensus about the criteria required to establish the diagnosis of PCOS. Two out of the three features below are used when other causes of those clinical features have been excluded.4 Exclusion of these other, much rarer, causes often needs no more than a routine clinical assessment.
The three features are:
-
anovulation or oligo-ovulation;
-
the presence of polycystic ovaries on pelvic ultrasonography;
-
clinical and/or biochemical signs of hyperandrogenism.
While awareness of PCOS, its diagnosis and associated morbidity is high, its basic pathophysiology is often poorly understood. This article presents a framework for teaching and increasing understanding about the causes and management of PCOS.
An approach to teaching and learning about PCOS
Undergraduate students, nurses, specialist trainees and even trained gynaecologists often find PCOS difficult to understand, particularly as the clinical features vary from patient to patient. One strategy that can be used when teaching about PCOS is to go back to basic ovarian biology and to use that as a starting point. This leads to a framework that lends itself to formal presentation, but also to informal illustrations in the clinic or in a tutorial. In addition it allows the management strategies to be described and understood. While different experts may have alternative views of its pathophysiological basis, and some assumptions can be questioned, the following model gives a useful framework to build upon and to introduce key concepts and management pathways.
In this framework there are six stages of development of information on the biology of the ovary and the factors that interact with it that help to clarify the background to the development of PCOS. Knowledge of these stages is then used as the key to understanding the approaches available for its management.
How follicles make estrogen
The first stage in this approach is to look at the production of sex steroids, particularly estradiol, within the ovarian follicle (Figure 1a). The follicle has two steroidogenic cell layers: the outer theca cell layer and the inner granulosa cell layer, separated by a basement membrane5 (Figure 1b). It is the granulosa cells that are responsible for the synthesis and secretion of estradiol. They do this initially under the stimulation of follicle-stimulating hormone (FSH) from the anterior pituitary gland, which binds to and activates their FSH receptors6 (Figure 1c).

The pathway involved in estrogen synthesis in the ovary. Granulosa cells (G), theca cells (T) and the oocyte (O) are the key cells in the follicle. It produces estradiol (E) from cholesterol (C) after stimulation by follicle-stimulating hormone (FSH), with androgen (A) as an intermediary. See text for an explanation of stages a–f.
Estradiol is a sex steroid and all steroids are derived from cholesterol.7 Cholesterol therefore has to be changed into estradiol by enzymatic modification through a series of intermediate steroids. In the pathway from cholesterol to estrogen, the step before estrogen is androgen (Figure 1d). Androgen is converted into estrogen by the action of the aromatase enzyme7 (Figure 1e). Granulosa cells contain large amounts of aromatase but they do not express the proteins and enzymes (steroidogenic acute regulatory protein, cholesterol side chain cleavage enzyme, 3β-hydroxysteroid dehydrogenase and 17α-hydroxylase) that are required for the conversion of cholesterol into androgen, so they cannot produce androgen themselves (Figure 1f).
As they cannot synthesise the androgen substrate, in order to make estradiol the granulosa cells need to get androgen from another source. The androgen is made in the theca cells and converted into estrogen in the granulosa cells (Figure 2a). Theca cells produce androgen under the stimulation of luteinising hormone (LH) from the anterior pituitary gland, which activates their LH receptors (Figure 2b).8 Thus to facilitate follicular estradiol secretion, LH causes the production of androgen from cholesterol in theca cells, and FSH promotes the conversion of those androgens into estrogens in the granulosa cells (Figure 2c). This synergy between the theca and granulosa cells is known as the two-cell, two-gonadotrophin model of estrogen synthesis9 and the hormones are physiologically balanced (Figure 2d).
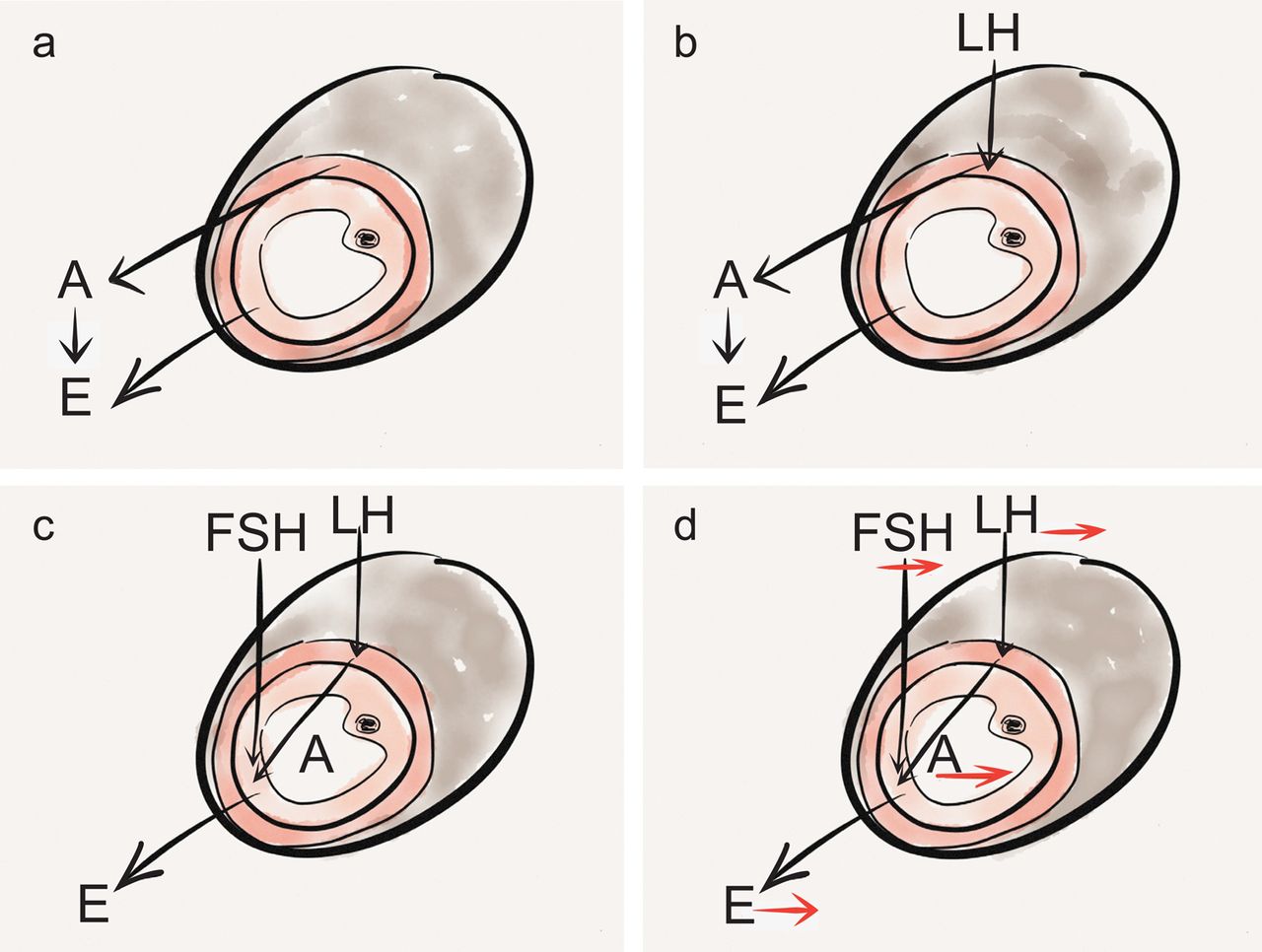
Illustration highlighting the two-cell two-gonadotrophin model of ovarian estradiol synthesis and its regulation. Luteinising hormone (LH) stimulates androgen (A) from theca cells which are converted to estrogen (E) in granulosa cells by follicle-stimulating hormone (FSH). See text for an explanation of stages a–d.
The effect of increased androgen on the ovary
The second stage in describing the development of PCOS is to highlight that the development of a polycystic ovary is associated with increased exposure to androgens as these have their own effects on follicular growth and development. A polycystic ovary contains an increased number of small antral follicles which are the small fluid-filled follicles that are seen on naked-eye inspection of opened polycystic ovaries and are clearly visible on ultrasound scanning. They are not 'cysts’ as they contain a potentially healthy oocyte10 and they can be stimulated to grow normally by exogenously administered FSH.11 This is why women with PCOS are at a much greater risk of developing ovarian hyperstimulation syndrome after administration of FSH during assisted conception.12 The ovarian ‘cysts’ in PCOS are therefore essentially paused follicles, with reduced cell growth as well as reduced cell death (atresia).
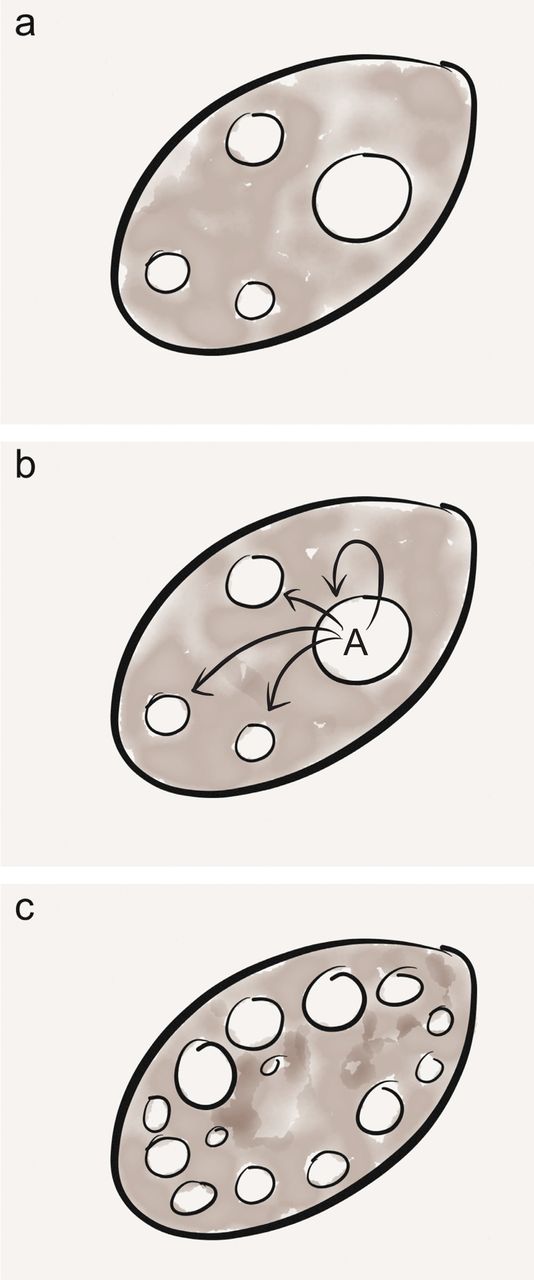
Androgen inhibits the growth of larger antral follicles but, if anything, stimulates the growth of smaller antral follicles (Figure 3a–c). Treating rhesus monkeys with normal ovaries with exogenous androgen for just 10 days resulted in a polycystic ovarian morphology, with an increased proportion of small antral follicles showing more cell proliferation in smaller follicles and less atresia in the remaining follicles.13 This highlights the ability of androgen to promote follicular growth and survival, inhibit later follicular development and directly cause a polycystic ovarian morphology.
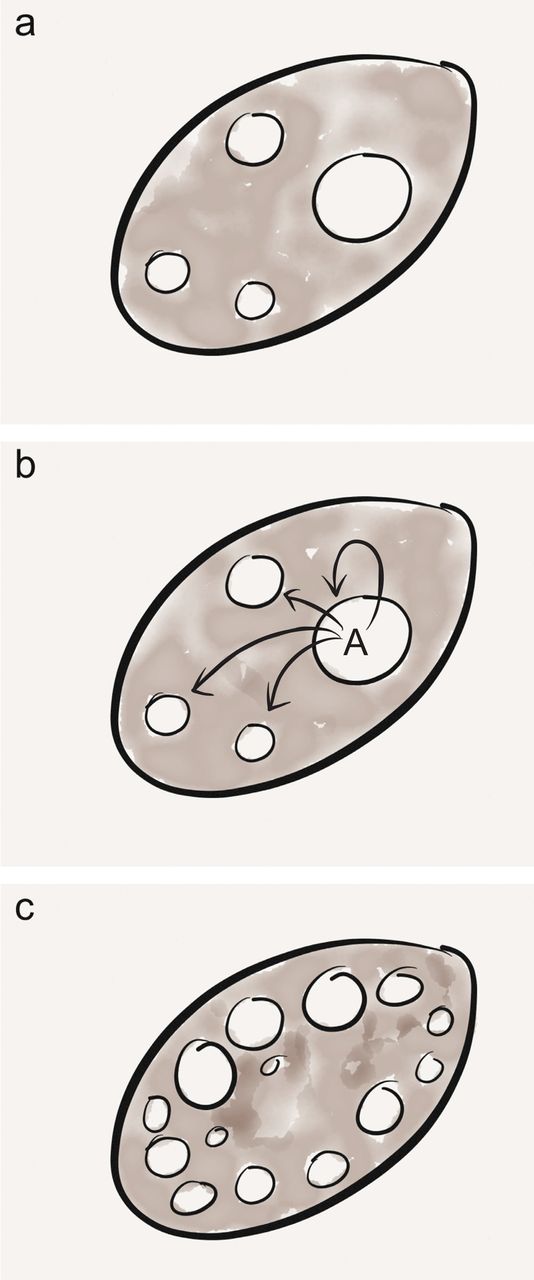
Diagram highlighting the role of androgens (A) in the conversion of a normal ovary to one with a polycystic ovarian morphology. See text for an explanation of stages a–c.
Clinically, this polycystic ovarian morphology is associated with increased endogenous androgens. Conditions in which endogenous androgen levels are pathologically raised include androgen-secreting tumours and late-onset congenital adrenal hyperplasia, in which adrenal androgen secretion is increased.14 Women with both these conditions develop polycystic ovaries.15 The response of the ovary to increased androgens is therefore the development of a polycystic morphology and inhibition of later follicular growth. This results in an increased incidence of anovulation.
Why the ovary might experience more androgen
The third stage is to discuss the mechanisms by which the ovary might be exposed to increased local androgen concentrations. Using the two-cell, two-gonadotrophin model illustrated in Figure 2d it can be demonstrated that if a hormone imbalance occurred, such that circulating LH concentrations were higher than FSH concentrations, ovarian androgen production would increase (Figure 4a). Previously an increased LH:FSH ratio was thought to be required for the diagnosis of PCOS. This is no longer part of the diagnostic criteria, which focus on the resulting increased androgens.4 However, it is clear that women with PCOS are more likely to have increased basal LH concentrations16 as well as increased LH pulse amplitude and frequency.17

Illustration highlighting the ‘sponge’ analogy for the role for sex hormone binding globulin (SHBG) in reducing luteinising hormone (LH)-dependent thecal androgen (A) availability, and the link of SHBG to weight and to the increase in free androgen when its level reduces. This does not affect follicle-stimulating hormone (FSH)-stimulated estradiol (E) secretion. See text for an explanation of stages a–i.
While chronic anovulation can result in raised LH concentrations,18 it is likely that the LH:FSH imbalance is something that women with a tendency to PCOS are born with and that this causes anovulation. There is increasing evidence from human and animal models that PCOS can be programmed by increased fetal exposure to androgen before birth.19 ,20 This may permanently programme increased basal LH secretion21 as well as augmenting the amount of LH released in response to gonadotrophin-releasing hormone (GnRH)22 and thus the amplitude of LH pulses. One way the ovary can be exposed to increased androgen is therefore by an increased LH:FSH ratio, which may be prenatally programmed.
Regulation of androgen action
The fourth stage is to describe a regulator of androgen bioavailability. This could be imagined as a ‘sponge’ that can mop up excess androgen (Figure 4b) in order to prevent it affecting follicular growth and development. The sponge could normalise slightly increased ovarian androgen production (Figure 4c). However, if the sponge is small it would not fully mop up the excess androgens that are normally produced during follicular estrogen synthesis (Figure 4d). That means that there may be increased androgen bioavailability in the presence of normal LH concentrations – and if there is an increased LH:FSH ratio a small sponge would augment the increased androgen exposure (Figure 4e).
That ‘sponge’ exists in the form of sex hormone binding globulin (SHBG), the circulating protein that binds to and inhibits androgens and to a lesser extent estrogens (Figure 4f). For the purpose of this framework it is now useful to highlight that SHBG is inversely related to weight (Figure 4g).23 As weight increases, SHBG decreases and androgen availability will therefore increase (Figure 4h). This means that polycystic ovaries or PCOS will worsen. Conversely, as weight reduces SHBG will increase and bioavailable androgen will decrease (Figure 4i), meaning that PCOS will improve. Weight is therefore a controller of LH action on the ovary and thus the effects of LH will be exaggerated by obesity.
Regulation of androgen synthesis
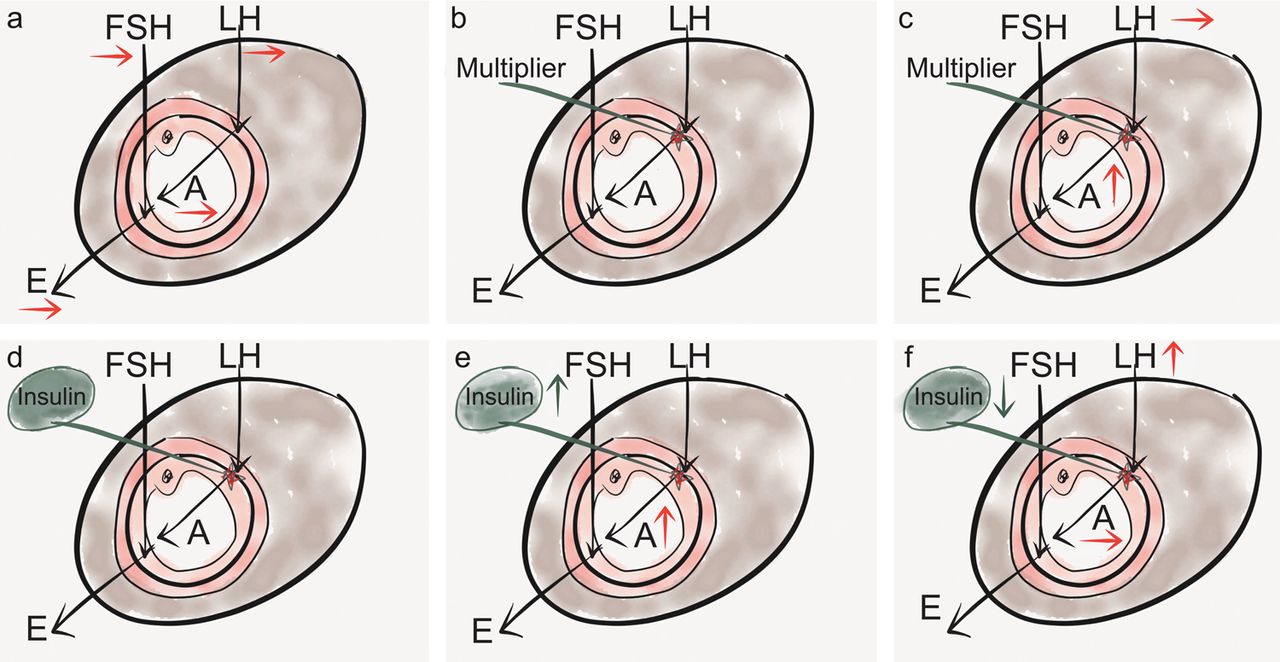
The fifth stage is to focus on the molecular regulation of LH-dependent androgen synthesis by the theca cells (Figure 5a). The key here is to imagine the effect that a multiplier of LH action would have at the level of the theca cell (Figure 5b). The presence of a multiplier would augment androgen production for a given concentration of LH. That means that ovarian androgen could be increased in the presence of normal concentrations of LH (Figure 5c).

Illustration highlighting the role of insulin in augmenting luteinising hormone (LH)-dependent thecal androgen (A) synthesis, and the reduction in that synthesis if hyperinsulinaemia improves. Follicle-stimulating hormone (FSH)-driven estradiol (E) synthesis continues. See text for an explanation of stages a–f.
That multiplier exists in the form of insulin (Figure 5d). This ubiquitous hormone regulates glucose transport and has growth factor and anabolic actions.24 It is also a co-factor that augments LH-induced thecal androgen secretion.25 ,26 In the presence of peripheral insulin resistance (IR), which is a precursor to impaired glucose tolerance, increased insulin concentrations are required to promote glucose uptake in tissues with a key metabolic role, such as muscle and fat. While these may be resistant to the metabolic effects of insulin, the ovary remains sensitive to its growth factor effects. The hyperinsulinaemia associated with IR therefore means that more androgen will be produced in the ovary. As IR worsens and insulin concentrations rise, ovarian androgens will increase and PCOS will worsen (Figure 5e). If IR improves and insulin concentrations fall, ovarian androgens will reduce and PCOS will improve (Figure 5f).
Interaction between weight and IR
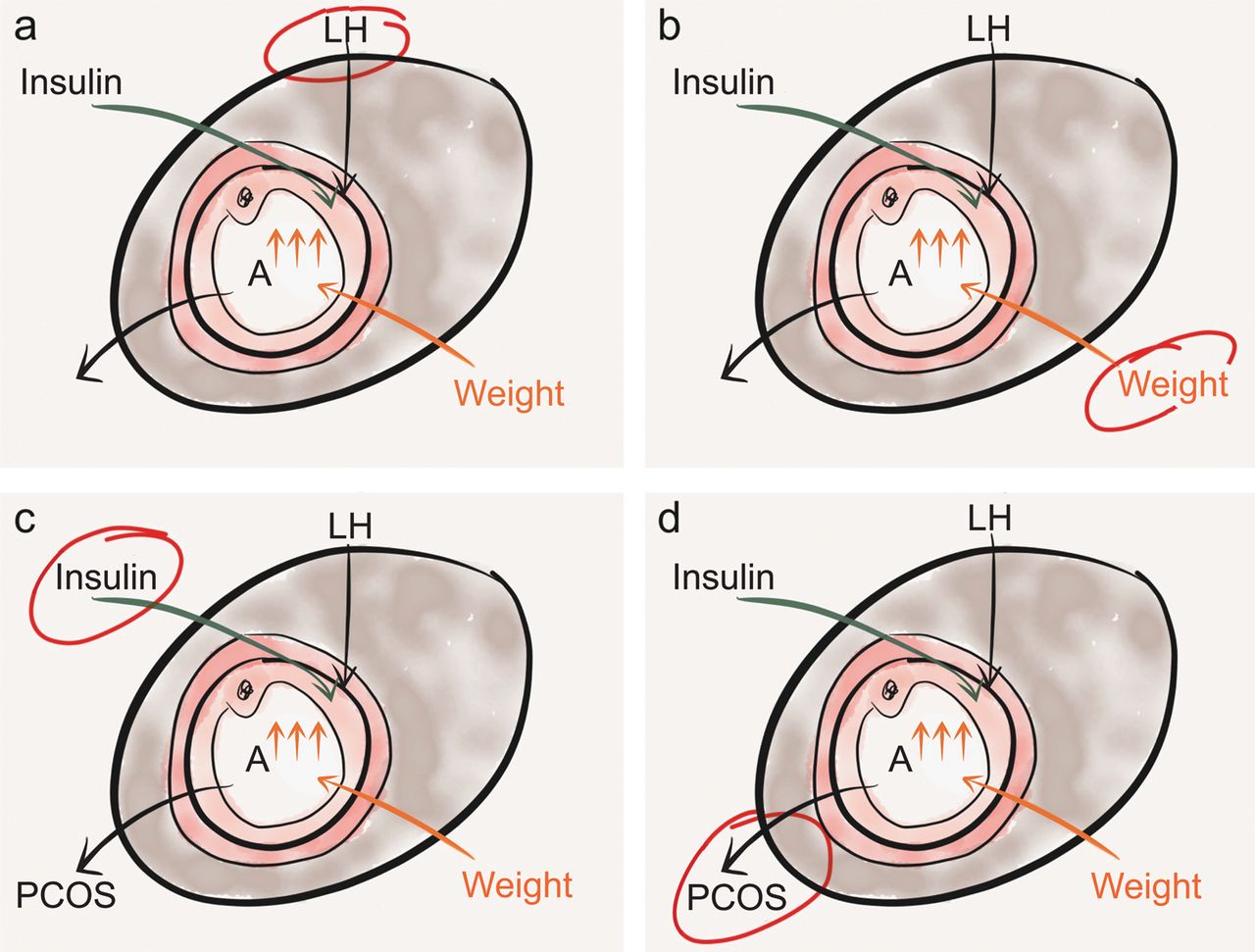
The sixth and final stage in understanding the causation of PCOS pulls together the information gained in the first five stages. As LH-induced androgen concentrations can be modified both by weight (through SHBG change) and by insulin, this can alter the degree by which PCOS is manifested. However the mechanism is not so straightforward, as insulin is an anabolic hormone and the hormone of energy storage.27 That means that high levels of insulin are associated with ease of weight gain and difficulty in weight loss (Figure 6a).28 As weight increases, IR increases and circulating insulin levels rise,29 producing a vicious cycle with weight and IR linked together (Figure 6b). Insulin itself can inhibit hepatic SHBG synthesis.30

Drawing illustrating the interaction between weight and insulin resistance, leading to augmentation of luteinising hormone (LH)-stimulated androgen (A) secretion, resulting in development of polycystic ovary syndrome (PCOS). See text for an explanation of stages a–d.
There are therefore three drivers to increased ovarian androgen production: increased LH, hyperinsulinaemia and increased weight (Figure 6c). So slim women with PCOS have more elevation in LH than obese women with PCOS.31 While some women with PCOS primarily have a high LH:FSH ratio, some are primarily insulin resistant and some have a major weight problem. The common consequence is the augmentation of androgens that results in PCOS (Figure 6d). In reality most women with PCOS will have each of these drivers in varying degrees.
A framework for the management of PCOS
The model where LH-stimulated androgen action is augmented by weight and insulin (Figure 6d) provides a useful framework with which to understand PCOS and to explain it to patients and students. But it also provides a useful approach to describe the strategies available for the management of patients with PCOS. The foci could be targeting gonadotrophin concentrations, reducing weight, lowering insulin or ameliorating the systemic effects of ovarian dysfunction and increased androgen levels.
Targeting gonadotrophins
Any treatment that lowers circulating LH concentrations will reduce ovarian androgen production and improve PCOS (Figure 7a). We do not yet have a treatment to specifically lower LH, so treatment generally involves reducing both LH and FSH. The main way to do that is with the combined oral contraceptive pill (COC), which is the mainstay of the management of PCOS32 if pregnancy is not desired. Any COC will do this effectively, although it has been argued that the more recent, less androgenic pills may be particularly useful.33 As half the androgens in women come from the adrenal gland,34 the combination of ethinylestradiol with an anti-androgen such as cyproterone acetate (co-cyprindiol), or a higher dose of cyproterone acetate in a reverse-sequential regimen,35 may have additional benefit for certain androgenic symptoms, particularly hirsutism.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration highlighting the roles of luteinising hormone (LH), increased weight and hyperinsulinaemia in raising intraovarian androgen (A) that results in polycystic ovary syndrome (PCOS). See text for an explanation of stages a–d.
For fertility treatment, the strategy is to raise FSH levels to facilitate the conversion of androgens into estrogens in order to remove the brake on follicle growth. As estrogens feed back to inhibit FSH secretion, the use of estrogen antagonists, such as clomifene citrate, or aromatase inhibitors such as letrozole, will raise FSH and improve ovarian function. However estrogen is needed for endometrial growth and to stimulate the ovulatory LH surge. Treatment is therefore given only for 5 days at the beginning of the cycle, either from Day 2 or Day 3. If treatment with anti-estrogens at various doses is not effective, then FSH may be directly raised by injections. Gonadotrophin ovulation induction is very successful in the management of subfertility secondary to anovulation in PCOS.36
Targeting weight
Weight loss improves the symptoms PCOS in both non-fertility and fertility contexts (Figure 7b). In the fertility setting the results are quite dramatic.37 ,38 Thus a weight loss strategy is very important in the management of all overweight and obese women with PCOS. A loss of 10% of body weight increased fertility, ovulation rate and menstrual regularity even when women remained obese.37 In addition there were associated improvements in serum biochemistry, blood pressure and self-esteem scores.37 ,38 It is important to highlight diet, with an emphasis on developing a weight maintenance/weight loss cycle involving regular small healthy meals, not skipping meals and avoiding refined carbohydrate.39 However, increased physical activity should always be a key message in weight management. Even in the absence of weight loss, exercise improves PCOS.40
Targeting insulin
Metformin treatment improves insulin sensitivity, thus enhancing glucose clearance, resulting in reduced circulating insulin concentrations (Figure 7c). There is no doubt that metformin can have beneficial effects in some women with PCOS.41 ,42 It can improve feelings of wellbeing, ovarian cyclicity and fertility as a main or as adjunct therapy.43 While metformin reduces hyperinsulinaemia44 and improves metabolic parameters, its effect on weight loss is more controversial.45 The degree of weight loss may relate to how engaged the patient is with a concurrent weight-loss programme. Recent results with metformin have been less impressive than initially reported.46 As not all women with PCOS benefit equally from metformin it may be that the key is adequate patient selection. More research is needed into such personalised medicine. However, metformin remains one of the tools available in the management of PCOS. The data on its prolonged use and discontinuation are scanty and variable, so it should not yet be used in the long-term with a goal of preventing future health problems.47–49 A current improvement in symptoms associated with PCOS seems a sensible rationale for its continuation.
Holistic targeting
One of the main areas to focus on is endometrial protection. Women with PCOS who are anovulatory are exposed to unopposed estrogen and are at risk of both prolonged heavy bleeding and the development of endometrial hyperplasia.50 It is generally advocated that women with PCOS who are amenorrhoeic should have three or four periods (in the form of withdrawal bleeds) a year to maintain endometrial health.51 A common strategy is to use an intermittent progestogen such as medroxyprogesterone acetate 10 mg twice daily for 7 days or once daily for 10 days. A few days after stopping treatment a withdrawal bleed will occur. If this is particularly heavy it may be that a shorter time between induced periods is required. An alternative approach is to use a COC or the levonorgestrel intrauterine system, both of which will provide full endometrial protection as well as effective contraception, as occasional ovulation could occur despite the amenorrhoea.
Hirsutism is a problem for many women with PCOS. While hormonal treatments such as the COC are designed to reduce ovarian androgens by lowering gonadotrophins, as already mentioned approximately 50% of androgens in women are of adrenal origin.34 Increased androgen promotes the transformation of vellus hair into longer, thicker and more noticeable terminal hair and sometimes reduction of ovarian androgen is insufficient alone to reverse this process. Management of hirsutism may therefore require additional treatments such as cosmetic strategies, local treatment such as topical eflornithine cream or laser therapy (which can be very effective in suitable patients, particularly those with darkly pigmented hair) or systemic treatment with an anti-androgen such as cyproterone acetate52 ,53 (Figure 7d).
Conclusion
PCOS is a common condition with a varied phenotype. While there might be alternative views on some elements of any framework to understand and manage the syndrome, it is hoped that practitioners involved in teaching students and trainees, and in managing patients, will find that this approach to understanding the condition is helpful.
References
Footnotes
-
Author's note This review article is based on a presentation given at a ‘Meet the Expert’ session at the annual meeting of the British Endocrine Society in 2012.
-
Competing interests The author is supported by a Scottish Senior Clinical Fellowship from the SFC with grant support from the Medical Research Council (G0901807).
-
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue