Article Text

Statistics from Altmetric.com
Why was change needed?
Women living in remote and rural areas of the UK face inequalities in provision of abortion services compared to their urban counterparts. Distances to travel, lack of providers, and legal restrictions that require administration of both mifepristone and misoprostol at the abortion service hamper access to, and provision of, abortion. NHS Highland provides care for women from a wide geographical area in the far north of Scotland, much of which is remote and rural and includes small islands. Abortion care is provided from a single National Health Service hospital department of obstetrics and gynaecology in Inverness. For some women, this means that they need to travel distances of over 100 miles to be assessed for an abortion, often using multiple modes of transport (including ferry and plane). Although abortion rates in this region are lower than the Scottish average (9.1 vs 11 per 1000 women aged 15–44 years), the total number of women having an abortion in the region is much lower than most parts of Scotland (fewer than 500 annually), reflecting the smaller population.1 This, combined with a lack of abortion providers in the region, means that the dedicated clinic for women requesting abortion takes place only once per week, adding to delays for some women. These factors undoubtedly contribute to the consistent failure to meet national standards for sexual health that recommend that 70% of women seeking abortion should undergo the procedure at 9 weeks’ gestation or earlier (i.e. 67% in 2014).1 ,2 We piloted and evaluated four new initiatives in the service aimed at improving access to abortion and minimising delays in provision.
How did we go about implementing change?
The chair of the local research ethics committees confirmed that ethical committee approval was not required for this health services research. The initiatives were piloted between June 2010 (or June 2011) and August 2013 and were:
Assessment for abortion by telephone consultation. To minimise the need for additional travel for women who lived on the islands, telephone assessments with a specialist nurse working in the abortion service were arranged. These were organised by hospital clerical staff and scheduled for 45 minutes on a single weekday afternoon. Women needed to provide a telephone number at which they could be contacted.
Early surgical abortion under local anaesthesia using manual vacuum aspiration (MVA). This offered women the possibility of same-day treatment as assessment and earlier discharge home after the procedure (compared to surgical abortion under general anaesthesia). Women who were ≤9 weeks’ gestation (based on ultrasound) were eligible for MVA. Operator availability was the key issue in determining availability and waiting times as this was performed by a single doctor (LC). The procedure used was similar to that described by others.3 All women received cervical treatment with misoprostol (400 μg sublingually 2 hours pre-procedure) in line with Royal College of Obstetricians and Gynaecologists recommendations.4 Empirical analgesia (e.g. 1 g paracetamol and 800 mg ibuprofen if no contraindications) was provided 30 minutes pre-procedure. Mepivicaine was the local anaesthesia used for paracervical block.
Early medical abortion (EMA) as an outpatient (i.e. women go home to expel the pregnancy after receiving misoprostol at the hospital).5 Women were considered eligible if they met the criteria in Box 1. The regimen used consisted of a single oral dose of 200 mg mifepristone followed 24–48 hours later with 800 μg misoprostol administered vaginally.4 ,5
Provision of mifepristone and/or misoprostol at a smaller rural hospital within the region. This allowed women who lived within the Caithness area and who had been assessed for EMA by the abortion service in Inverness (which remained responsible for overall care) to have EMA as an outpatient procedure at the local rural hospital.
Eligibility criteria for early medical abortion as an outpatient
▸ ≤9 weeks’ ultrasound confirmed intrauterine pregnancy
▸ ≥18 years of age
▸ Certain of decision
▸ Adult to accompany them home after misoprostol and be at home with them
▸ Reside within 30 minutes’ travel time from clinic
▸ No medical contraindications to medical abortion
▸ No significant medical conditions
▸ Does not require interpreter
▸ No cause for concern (no child protection issues, domestic violence, abuse, etc.)
What outcomes resulted from the change in practice?
A total of 48 telephone consultations were arranged (June 2011–August 2013). Four women did not answer the telephone call, two decided to continue with the pregnancy and one further woman had a miscarriage. Of the 41 women proceeding to abortion, six had an MVA at a single clinic visit, five had an MVA but stayed overnight in the hospital's patient accommodation (as round trip travel not possible), 16 chose medical abortion and 14 had a surgical abortion under general anaesthesia. The telephone consultation service permitted scheduling of all the surgical abortions (n=25; 61%) as a single hospital visit.
A total of 31 MVA procedures were performed during the pilot (June 2011–August 2013). Self-administered anonymous questionnaires on the experience of the procedure were completed by 30 women (a 97% response rate) following MVA. Ten (33%) women rated discomfort during MVA as ‘not as bad as expected’ and 16 (53%) stated that discomfort was ‘as they had expected’. Most (n=26, 83%) women stated that they would choose this procedure again (if required) and recommend it to a friend. High uptake of effective methods of contraception was noted in this pilot with 23 (74%) women leaving the service with a long-acting reversible method of contraception; in 17 (55%) women this was an intrauterine method.
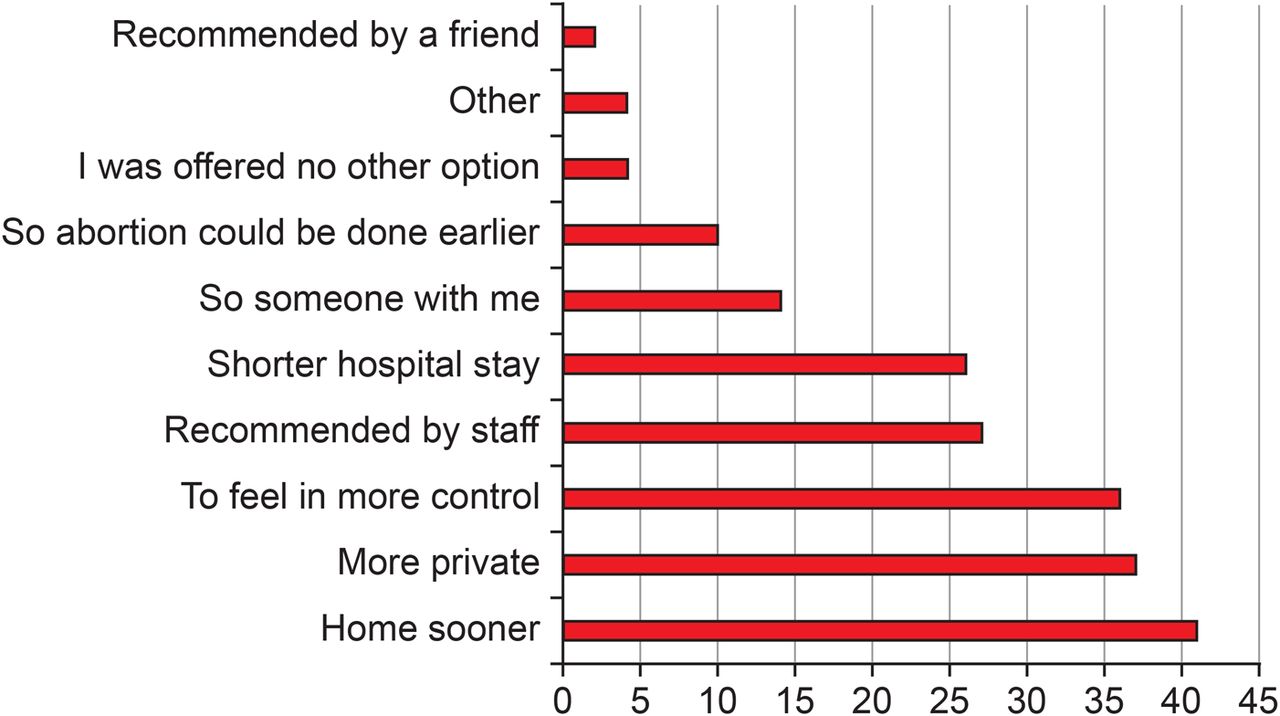
Only 34% of all women referred to the service over the study period (June 2010–August 2013) lived within 30 minutes’ travel time from the hospital, and so only a minority of women met the eligibility criteria for outpatient EMA on the basis of geography alone. A total of 169 women chose to have an outpatient EMA during the pilot and 104 (62%) completed self-administered anonymous questionnaires at a routine 2-week follow-up about the reasons for choosing outpatient EMA (Figure 1) and their experience. Most (91/104; 87%) women indicated that they would opt for outpatient EMA if faced with a further unintended pregnancy, 10 (10%) women were unsure and only three (3%) stated they would not choose this method. Acceptability of outpatient EMA to Highland women was also supported by 97/104 (93%) indicating that they would recommend it to a friend, with six (6%) women being unsure. Only one woman said she would not recommend it.

{kind=link}
Reasons selected by respondents (n=104) from a predefined list for choosing outpatient early medical abortion (EMA).
During the pilot (June 2011–August 2013) a total of 69 women received the first part of EMA (mifepristone) locally at Caithness Hospital. However, only one woman received misoprostol at this hospital, which permitted her to have outpatient EMA. The sporadic nature of presentation of women from this area who wanted to have outpatient EMA (and who were eligible) meant that it was difficult for local staff to build up confidence in administering prescribed medical abortion drugs. As a consequence, medical abortion drugs at this site expired during the pilot period and staff felt that they had insufficient expertise to deliver full EMA care. Other difficulties encountered were that staff turnover at the rural hospital made providing this service difficult, as those lacking familiarity with medical abortion were unwilling to administer the drugs. In addition, contacting the appropriate staff member in the rural site to arrange for the woman to attend for medication was time consuming. Furthermore, women from this area were not always keen to attend the local hospital for care, desiring ‘anonymity’ at the main hospital in Inverness.
What advice would we give to others considering similar action?
Of the initiatives piloted to improve timely access to abortion in our remote and rural setting, we found that telephone consultations and MVA were perhaps the most successful. Telephone consultations allowed for exchange of information, and for those suitable and wishing an MVA permitted treatment during a single hospital visit. The provision of intrauterine contraception at MVA may also overcome the barriers of accessing this method of contraception after abortion within a remote and rural setting.
The legal restrictions in the UK mean that women undergoing EMA must receive misoprostol on licensed premises,4 which essentially prohibits those who live far from an abortion service from opting for outpatient EMA. Thus hospital admission for EMA will always be needed to a greater degree in remote and rural settings. This restricts choice for women but also has an inevitable impact on hospital resources. The 30 minutes’ travel time criterion for EMA was originally chosen because of concern that misoprostol may start working soon after administration and that women might experience excessive pain or bleeding during their journey home and find it difficult to travel back to the service. However, given our accumulated experience and studies from Norway showing the safety of home EMA for women living in remote areas up to 1 hour's travel from hospital settings, we have now expanded outpatient EMA to women who live 1 hour away.6 Although we tried to facilitate access to EMA by establishing a link with a rural hospital licensed to administer treatment, the small workload meant that providing and maintaining this service was extremely difficult. Promotion of EMA from this (or future) satellite hospitals has ceased. In addition, the total number of women having abortion in our region has meant that the time taken to evaluate these initiatives has been considerable.
Footnotes
Twitter Follow lynn macKay at @lmack20
Funding The work was undertaken with support of the Scottish Department of Sexual Health and Blood Borne Viruses as part of a series of initiatives aimed at improving the patient journey through abortion.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue