Article Text

Abstract
Background Repeat termination of pregnancy highlights the issues of unplanned pregnancies and effective post-termination contraceptive practices.
Objective To examine the risk factors at the time of a first termination that are associated with subsequent repeat termination.
Design Registry-based study.
Setting Grampian region of Scotland, UK.
Methods A retrospective study using data from the Termination of Pregnancy Database, NHS Grampian for the period 1997–2013. Associations between repeat termination and women's sociodemographic characteristics and contraceptive use were assessed using multivariable logistic regression models.
Results This study showed that 23.4% of women who had an initial termination (n=13 621) underwent a repeat termination. Women who had repeat terminations were more likely to be aged under 20 years at their initial termination with an adjusted odds ratio (AOR) of 5.59 [95% confidence interval (CI) 4.17–7.49], to belong to the most deprived social quintile [AOR 1.23 (95% CI 1.05–1.43)], and to be more likely to have had two or more previous livebirths [AOR 1.51 (95% CI 1.12–2.02)] or miscarriages [AOR 1.40 (95% CI 1.02–1.92)]. The likelihood of having a repeat termination was increased in women who had a contraceptive implant as post-termination contraception [AOR 1.78 (95% CI 1.50–2.11)] compared to women who left with none or unknown methods following the first termination. In those who had repeat terminations, women who had an implant or Depo-Provera® were at increased odds of repeat termination in the 2–5 years interval compared to the 0–2 years after their initial termination.
Conclusions Teenage pregnancy, social deprivation, two or more previous livebirths or miscarriages at the time of the initial termination were identified as risk factors for repeat terminations. Post-termination contraception with implants and Depo-Provera® were associated with repeat termination 2–5 years after the first termination.
- abortion
- epidemiology
- long-acting reversible contraception
Statistics from Altmetric.com
Key message points
Risk factors for repeat terminations of pregnancy include younger age at initial termination, belonging to a more deprived Scottish Index of Multiple Deprivation quintile and engaging in risky sexual behaviour.
Women who had a progestogen implant for contraception following their first termination had an increased likelihood of a subsequent termination.
Depo-Provera® and implants offer protection from repeat termination for up to 2 years after the initial termination, but thereafter become risk factors.
Introduction
Terminations of pregnancy have been noted to be declining in Scotland from 13.1 per 1000 women in 2008 to 11 per 1000 women in 2014. However, around one-third of these women in 2012 had had one or more previous terminations and the rate of repeat terminations has remained static at 3.6 per 1000 women of reproductive age in 2008 to 3.5 in 2014.1
Repeat termination is a measure of unplanned pregnancy and unmet contraceptive need in the community. With the legalisation of pregnancy termination in the UK through the Abortion Act 1967, unsafe termination is no longer a major cause of mortality and morbidity, but there are adverse effects of repeated terminations of pregnancy on reproductive health, namely, preterm delivery in subsequent wanted pregnancies.2 ,3 From a public health perspective there is a need to identify women at risk of having repeat terminations and put in place targeted interventions to prevent unplanned pregnancies. Repeat terminations are noted to be associated with a number of factors such as increased parity,4–6 poor relationships7 ,8 and deprived socioeconomic circumstances.7 ,9 ,10 A number of studies highlighted that these women are more likely to be using a method of contraception before or at the time of conception, which may indicate high failure rates in contraceptive method or in method use in these women.11–14 However, these data are likely to be self-reported and consequently are prone to social desirability bias. The majority of these studies rely on case note review or self-reported surveys and are therefore limited in sample size and are prone to recall bias. Register-based studies have the advantage of large number of participants, and population-based registers can potentially reduce or eliminate selection bias, but individual records of terminations are rarely linkable due to reasons of confidentiality and anonymisation. The Termination of Pregnancy (TOP) Database in Grampian offers the unique opportunity to explore the risk factors associated with repeat terminations in a population served by a single sexual health service clinic. This database was started in 1992, and has been continuously and contemporaneously recording and storing information on all terminations carried out at Aberdeen Royal Infirmary. The unresponsive rate of repeat termination within Scotland accentuates the need for an examination of this cohort in order to inform effective service delivery and aim interventions at a specific demographic. Thus, this study aimed to examine the risk factors for repeat termination that were present at the time of the first termination, using routinely collected anonymised health care data.
Methods
Ethical approval to carry out the study was granted by the North of Scotland Research Ethics Service and NHS Research and Development approval was given for non-commercial use of NHS data (REC Ref. No: 14/NS/0034). Permission to use the data was also obtained from the steering group of the TOP Database.
This was a case control study using routinely collected data from the TOP Database NHS Grampian extracted from January 1997 to December 2013. The year 2010 was chosen as the cut-off for women having their first termination who were also identified from the same database, allowing a 3-year follow-up period to 2013 in order to identify any subsequent termination within the follow-up time. The database collects information on all terminations at Aberdeen Royal Infirmary, the only termination service provided to Aberdeen city and Aberdeenshire, excluding approximately 150 terminations each year from Moray that are managed in Elgin. The relevant variables extracted included age at the first termination, Scottish Index of Multiple Deprivation (SIMD), previous obstetric history including miscarriage, ectopic pregnancy and live births, self-reported contraceptive use at time of conception, self-reported method failure and emergency contraceptive usage, post-termination contraceptive method, method of termination, gestational age at termination, and sexually transmitted infections (STIs).
The outcome measure was repeat termination and was defined as women who had two or more terminations within the time period of the study and these were obtained by matching by CHI number, a unique identifier given to all persons registered with a general practice in Scotland. The matching and linking of data was done by the data management team, University of Aberdeen and the anonymised data were released to researchers for analysis. The predictor variables were taken from the proforma routinely completed prior to the initial termination. Tests for STIs were undertaken for most women.
Statistical analyses used Statistical Package for Social Sciences (SPSS) V.22 (IBM Corporation, Armonk, NY, USA). All continuous variables (e.g. age) were categorised into clinically meaningful groups for analysis. Baseline sociodemographic characteristics were compared between women with single and multiple terminations using the Chi-squared (χ2) test. A p value of <0.05 was taken to indicate statistical significance. Multivariable logistic regression models were used to assess factors associated with repeat termination while simultaneously adjusting for other variables in the model. Complete case analysis was used in this analysis and only those terminations with a completed method of termination were included in the analysis. Each explanatory variable was presented as odds ratios (ORs) with 95% confidence intervals (CIs).
A further analysis was undertaken to examine the factors that were associated with time intervals between the first and second terminations. The most appropriate time interval cut-offs were chosen based on the distribution of the data. As the majority of repeat terminations occurred before an interval of 5 years, the time period between two terminations was grouped into more or less than 2 years with less than 2 years being the reference category.
Results
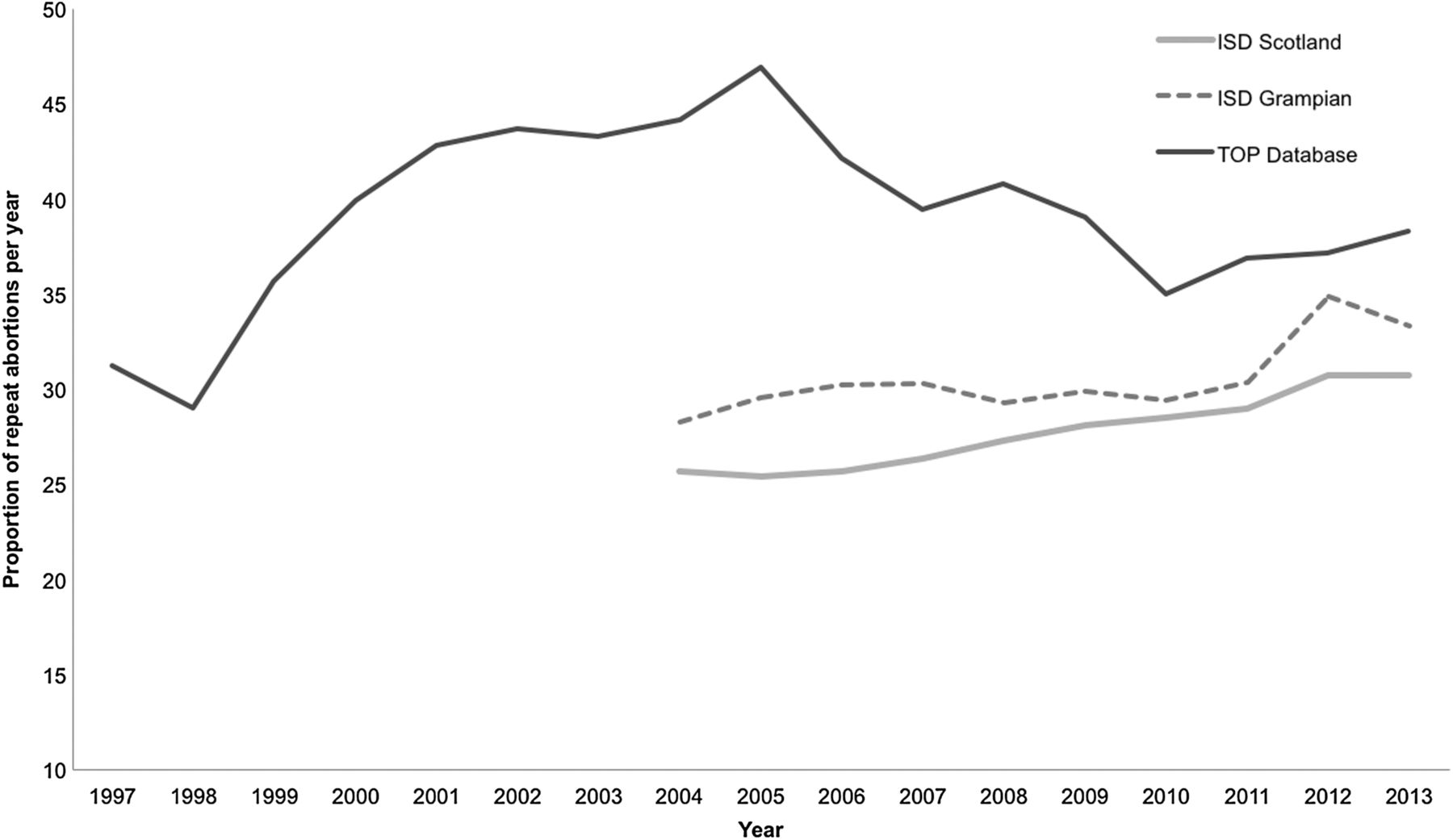
There were 14 978 individual women who had one or more terminations recorded in the database; 1357 cases were excluded as they did not have a recorded termination method, giving a total of 13 621 women. The number of women who had at least one further termination recorded was 3,192 (23.4%). Figure 1 shows the time trends in the proportion of repeat terminations in Grampian as obtained from data sources, and highlights that Grampian has had a higher proportion of repeat terminations than the Scottish average. The Scottish and Grampian proportionate yearly rate as reported by the Information and Services Division of NHS Scotland (ISD) has been increasing over time, with only the most recent 2 years showing a decline. Conversely, analysis of data from the TOP Database in Grampian shows that although the proportion of repeat terminations is higher than that reported by ISD both for Grampian as well as Scotland as a whole, it has been declining since 2005.

{kind=link}
The proportion of repeat terminations across time in Aberdeen, NHS Grampian and Scotland. Aberdeen data provided by the Termination of Pregnancy (TOP) Database. Scottish and NHS Grampian data provided by the Information Service Division (ISD), NHS Scotland.1
Comparison of characteristics of women with single and multiple terminations
Bivariate analysis comparing women with repeat terminations to women with one termination is presented in Table 1. Women with repeat terminations were more likely to be younger, have a positive chlamydia test result, have been tested for syphilis and blood borne virus (BBV) and have had a progestogen implant as their post-termination contraceptive at the time of their first termination. There was no statistically significant difference between the two groups in terms of the method of contraception at the time of conception.
Comparison of baseline characteristics between women with one and two or more terminations
Factors associated with repeat terminations
Table 2 shows the results of the mulitvariable analysis of those with a repeat termination compared to women with a single termination. After mutually adjusting for all other factors included in the logistic regression model, the following groups showed increased odds of having a repeat termination: age below 20 years at the initial termination [adjusted OR (AOR) 5.59 (95% CI 4.17–7.49)]; women with two previous live births at the time of their initial termination [AOR 1.51 (95% CI 1.12–2.02)]; and women in the most socially deprived category when compared to those in the least deprived group [AOR 1.23 (95% CI 1.05–1.43)]. There was no significant association with the trimester of gestation at which the termination was undertaken. Women with a surgical termination, in comparison to medical terminations, had a decreased likelihood of a repeat termination [AOR 0.85 (95% CI 0.77–0.94)]. When examining contraception use at conception at the time of initial termination, there was no statistically significant association for any of the contraceptive methods used. With regard to post-termination contraception, women who were fitted with an implant after their initial termination had increased odds of a repeat termination [AOR 1.78 (95% CI 1.50–2.11)] compared with none, unknown or natural methods of contraception. Changing the reference category to hormonal methods had little effect on the findings.
Risk factors for repeat terminations compared to one termination
Factors associated with longer interval between terminations
The time interval between the first and the second termination within the repeat termination group was a median of 30 months with an interquartile range of 14–58 months. Table 3 presents the factors associated with a time interval of more than 2 years between first and second terminations in women who had repeat terminations. Age at initial termination was no longer a statistically significant association. Women with three or more previous pregnancies were less likely to have an inter-termination interval of more than 2 years [AOR 0.33 (95% CI 0.21–0.53)]. Two previous live births, in comparison to no live births, increased the likelihood of a longer (>2 years) interval between terminations. Those with a longer inter-termination interval were at decreased odds of having been tested for a STI BBV [0.45 (95% CI 0.32–0.64)]. These women were also less likely to have a medical termination. Women discharged with either Depo-Provera® or implant compared to none or unknown or natural methods following the initial termination were at increased odds of a longer time interval to the next termination, with odds of 2.36 (95% CI 1.70–3.28) and 2.21 (95% CI 1.57–3.11), respectively.
Risk factors for repeat terminations: comparison of repeat terminations within 2 years versus after 2 years of the initial termination
Discussion
Main findings
This is the first comprehensive analysis of the determinants of repeat termination using a large population-based database in the UK. Women with repeat terminations were more likely to be below 20 years of age at their first termination, have had two live births, or belong to a more deprived SIMD quintile. This study showed that at the initial termination there were no statistically significant differences in the contraceptive method before the first termination. However, women with more than one termination were more likely to have had an implant as their post-termination contraceptive method. The examination of inter-termination time intervals within the repeat termination group showed that women who chose either the implant or Depo-Provera were more likely to have a repeat termination 2–5 years after their initial termination.
Strengths and limitations
This study had one of the largest sample sizes in the published literature on repeat terminations, thus reducing the likelihood of a type II error. The quality of the data, collected by dedicated nursing staff at the time of termination and entered by a trained coder into the database, adds validity to the study. As the TOP Database collects all terminations in the geographically defined area of Grampian, in North East Scotland, selection bias is likely to be minimal. The ability to link terminations occurring in the same woman is a special advantage of using this database, as reproductive histories can be constructed automatically without taking recourse to case note review or self-reported history where under-reporting can occur.
Despite this, some under-reporting of repeat terminations is likely to occur as women may have had another termination in a different health board or hospital and women who have moved into this health board area may have had a previous termination in another region. Similarly, we have analysed data from 1997 as recorded in this database, therefore it is possible that we may have misclassified some women who had a termination prior to this time period. We anticipate that this misclassification is likely to be small as Grampian has a relatively stable population and a lead period of 5 years between 1992 and 1996 was given for the analysis in order to minimise this misclassification. In addition, changes in demographic factors may have occurred between the initial and subsequent termination that were not taken into consideration in the analysis. We were unable to examine some risk factors implicated in the literature such as smoking, substance misuse, ethnicity, marital status and domestic abuse as the TOP Database did not collect information on these variables. Furthermore, the study findings may be limited by residual confounding from other unmeasured or poorly measured factors.
Context of findings
This study has found that the rates of repeat terminations recorded in the TOP Database in Grampian are higher than the Scottish average despite using the same method to calculate the rate in both cases.1 The rate of repeat termination is of course dependent on the total number of terminations if this is used as the denominator. An increase in the rate of repeat terminations may reflect either an increase in the number of repeat terminations or a decrease in the total number of terminations.15 We used the same denominator as ISD statistics to maintain comparability. This highlights that ISD may have been under-reporting the proportion of repeat terminations in Scotland. A possible explanation for this may lie in the data collection method. The women in this database are matched using their CHI number by data management staff while ISD's data on repeat termination is collected as a self-reported measure.
Other studies have found that women with repeat terminations were younger at their initial pregnancy, which is consistent with the present study.8 ,9 ,16 Women who are sexually active early in life are exposed for longer to pregnancy risk during their reproductive years, thus increasing the likelihood of having a subsequent unwanted conception leading to termination.
This study confirmed the findings of other studies that parity increases the likelihood of a repeat termination,4 ,6 with two previous live births at the initial termination increasing the risk. Kirkman et al.17 reported that women with higher parity who had an abortion did so because they did not want to look after another child. This study also showed that women from the most deprived socioeconomic quintile had an increased likelihood of a repeat termination. This is consistent with previous research.7 ,9 ,10 Furthermore, these women were more likely to have been tested for a BBV and in the bivariate analysis were more likely to test positive for a chlamydial infection. This result is supported by the limited literature that has examined the association with STIs.12 Previous research has shown that women from deprived areas and who are younger at sexual debut are more likely to engage in risky sexual behaviours with unprotected sexual intercourse,18 which increases the risk of STIs as well as pregnancy. 19
Contraceptive usage at conception at the initial termination in both groups was very similar. However post-termination contraception was different as women who chose implants had an increased likelihood of a repeat termination. These women in particular were more likely to have their second termination between 2 and 5 years after their first termination. A number of studies have highlighted that use of long-acting reversible contraception (LARC) after an initial termination may be an effective approach to contraception, but among women who have repeat terminations, there is a suggestion that the discontinuation rate of LARC may be high.10 ,20–23
Women who used implants and Depo-Provera (forms of LARC) were less likely to have a repeat termination within 2 years, which was consistent with previous cohort studies. These studies had relatively short follow-up periods and showed that in the short term, use of LARC reduced the risk of repeat terminations.22 ,23 A case note review in Edinburgh showed that implants and intrauterine device (IUD) methods reduced the likelihood of a subsequent termination; this study had a follow up of 2 years, which would be consistent with the findings of the current study.24 Our study is able to build upon the literature to show that beyond a 2-year interval these women were more likely to have a repeat termination. Published evidence showed that the continuation rate of Implanon® after 2 years was 47% in a Scottish population.25 A possible explanation for this is that these LARC methods are known to have side effects such as irregular bleeding, which have been found to be one of the main reasons for their discontinuation.26 ,27 Furthermore, missed appointments and irregular bleeding are the main reasons for poor continuation rates of Depo-Provera.28 Finally, discontinuation of LARC methods may also be the result of their over-promotion: they may not reflect the women's own contraceptive choice, thus a ‘woman-centred’ approach may be more appropriate in post-termination contraceptive counselling.29
Clinical and research implications
Our findings show that two groups of women would benefit from targeted preventive strategies to tackle repeat terminations. The first group comprises young women who start their reproductive life early, belong to a deprived social class and engage in risky behaviour. They have previously been targeted extensively through school health programmes and there is emerging evidence to show that these interventions are having an effect.30 ,31 The second group of older women with two or more children are largely a neglected group and warrant postnatal contraceptive counselling and follow-up with active involvement from the woman herself. Although it is established that LARC is effective, discontinuation rates of implants and Depo-Provera injection are high, making repeat terminations more likely. Moreover, the high rate of medical terminations make implants a more common post-termination contraceptive practice. IUD insertion after medical terminations may become as common as that after surgical terminations in the future. A targeted call/recall system of follow-up in the community may also be effective in reducing discontinuation rates of contraception, although there is limited evidence to support this and it is practically difficult to implement. Downloadable mobile phone applications may play an important role in the future in reminding women that their contraceptive implant is due for renewal. Further research into effective interventions needs to be designed on qualitative research into women's own choice and assessed by means of randomised controlled trials.
Acknowledgments
The authors thank Mr Peter Szchechina and Mr Alastair Soutar for extracting the data for this study and Professor Allan Templeton for initiating the TOPS Database in Grampian and for critically evaluating the manuscript.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Funding Sexual Health and Blood Borne Virus Managed Care Network, Department of Public Health, NHS Grampian.
Competing interests None declared.
Ethics approval North of Scotland Research Ethics Service and NHS Research and Development approval was granted for non-commercial use of NHS data (REC Ref. No: 14/NS/0034).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data can be obtained by an application to the Termination of Pregnancy Database, NHS Grampian.
Linked Articles
- Highlights from this issue