Article Text

Abstract
Introduction HIV infection and pregnancy are both common among female sex workers (FSW), indicating the need for prevention of mother-to-child transmission (PMTCT) among FSW.
Methods FSW were enrolled into studies in Swaziland, Burkina Faso and Togo using respondent-driven sampling. Women completed interview-administered socio-behavioural surveys and HIV counselling and testing. This secondary analysis describes contraceptive use and attempted pregnancy among reproductive-aged FSW (16–49 years). Robust Poisson regression with generalised estimating equations to account for clustering within recruitment networks was used to separately estimate associations between current unmet contraceptive need and attempted pregnancy among FSW.
Results Overall 1666 FSW were enrolled, 1372 (82.4%) of whom had ever been pregnant. In Togo and Burkina Faso, 83 FSW reported a prior HIV diagnosis and having a child, of which 12.1% (10/83) reported a child known to be HIV-positive. Twenty-five per cent of FSW had an unmet need for contraception; 9% of FSW employed dual contraception, including highly effective non-barrier methods and consistent condom use. Consistent condom use varied substantially by partner type and was higher with clients than non-paying partners. Nineteen per cent (n=313/1666) of FSW were trying to conceive. HIV-positive, undiagnosed FSW were more likely to be trying to conceive as compared to HIV-negative FSW; among 98 HIV-positive women trying to conceive, 25.5% were on antiretroviral therapy.
Conclusions FSW have varying reproductive goals and contraceptive usage. Efforts to improve coverage of comprehensive family planning – including efforts to increase HIV testing and engagement in treatment among FSW trying to conceive – are necessary for PMTCT.
- epidemiology
- family planning service provision
- needs assessment
- female sex workers
- prevention of mother-to-child transmission
Statistics from Altmetric.com
- epidemiology
- family planning service provision
- needs assessment
- female sex workers
- prevention of mother-to-child transmission
Key message points
In Burkina Faso and Togo, 12% of female sex workers (FSW) with children and a prior HIV diagnosis reported a child living with HIV.
Only one-quarter of FSW living with HIV and currently trying to conceive were on antiretroviral therapy, demonstrating opportunities to reduce mother-to-child-transmission risks.
FSW across three sub-Saharan African countries had high unmet family planning needs, including contraception as well as preconception care for women trying to conceive.
Introduction
HIV prevalence has been estimated to be 13.5 times greater among female sex workers (FSW) as compared to other women of reproductive age in low- and middle-income countries.1 Pregnancy, both intentional and unintentional, is also common among FSW.2 ,3 High numbers of sexual partners and inconsistent condom use, often due to experiences of sexual violence, contribute to both HIV acquisition, as well as unintended pregnancy.1–5
The prevention of unintended pregnancies among women living with HIV is the second pillar of the World Health Organization's four-pronged prevention of mother-to-child transmission (PMTCT) approach.6 This PMTCT component is particularly relevant for FSW, who may be less likely to access antenatal care services, including antiretroviral therapy (ART), during pregnancy.7 Prevention of unintended pregnancy among HIV-negative FSW is also important as a PMTCT strategy. Many FSW continue to sell sex during pregnancy, which is associated with sustained vulnerabilities for primary HIV infection during pregnancy,7 ,8 and thus there are high and sustained risks for vertical HIV transmission from mother-to-child.9 ,10
Prevention of unintended pregnancy alone is not adequate as a comprehensive PMTCT approach among FSW.7 Women who sell sex, like other women, often have desires or plans to expand their families.3 ,11 Pregnancy planning in the context of sex work is more complex though, as FSW may have different reproductive goals with different sexual partners including husbands and other non-paying partners, as compared with clients. When pregnancy goals diverge across clients and non-paying partners, contraceptive methods are limited to short-term barrier methods which have higher failure rates.12 Additionally, women engage in sex without condoms in order to conceive, which places them at greater risk for primary HIV infection or super-infection in the peri-conception period.
Thus fertility desires, alongside contraception, should be considered when evaluating unmet family planning needs of FSW and adequacy of PMTCT efforts. The objective of this analysis is to consider comprehensive family planning needs among FSW, including the demand for preconception services, across three sub-Saharan African countries.
Methods
Recruitment methods and study population
This was a secondary analysis using data from three cross-sectional respondent-driven sampling (RDS) studies carried out with FSW in Swaziland, Togo and Burkina Faso. Methods for RDS studies have been previously described.13 Briefly, RDS is used to recruit hard-to-reach populations, including FSW, through leveraging peer recruitment. A few purposively selected and well-connected individuals who met study eligibility criteria were invited to participate in the study at each site and function as ‘seeds’. The ‘seeds’ subsequently invited up to three eligible peers they knew to participate using a coupon provided by the study. The peer-referral process continued with each new recruit inviting up to three new eligible peers until recruitment targets were met. Each participant was linked to their recruits through the coupon system.
Specific catchment areas included Manzini, Mbabane, Piggs Peak and Lavumisa in Swaziland, Ouagadougou and Bobo-Dioulasso in Burkina Faso, and Kara and Lomé in Togo. Methods for recruiting and enrolling participants across countries were similar. FSW were eligible to participate in the studies if they were born female, reported sex work within the past 12 months (sex work had to be the principal revenue source in the past 12 months in Togo and Burkina Faso, but not Swaziland) and presented a valid RDS coupon. In Swaziland, FSW ≥16 years were enrolled, whereas studies in Togo and Burkina Faso included FSW ≥18 years old. Only women of reproductive age (≤49 years) are included in these analyses. Informed consent was administered in the locally spoken languages at each location. Study participation was anonymous and all study-related procedures were conducted in private rooms at secure study sites. Participants received reimbursement for time and travel costs.
At each site, procedures included a 45–60-minute interviewer-administered questionnaire covering demographics, stigma and human rights violations, sexual and reproductive health and behaviour, and participation in HIV prevention and care. Participants underwent rapid HIV testing, including pre- and post-test counselling in accordance with national guidelines. Referrals to care were provided for all participants with reactive HIV test results. Participants were excluded from the analysis if they did not complete all study procedures, including HIV testing.
These analyses combine study populations across three countries in order to assess the reproductive health needs of a large sample of sub-Saharan African FSW, which include representation of women from countries with diverse HIV epidemics. National adult HIV prevalence estimates across the three countries are 1.0% [95% confidence intervals (CI) 0.8–1.1%] in Burkina Faso, 2.9% (2.5–3.5%) in Togo, and 26.5% (24.6–28.3%) in Swaziland.14
Ethical approval was received from the Swaziland Scientific and Ethics Committee, the Health Research Ethics Committee of Burkina Faso, the National Ethics Committee of Togo and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
Statistical analysis
Descriptive statistics for the sample are presented and sample distributions across sites and key variables are compared using Chi-squared (χ2) statistics. RDS-adjustment techniques are not appropriate when sample populations across study sites are combined.15 As such, this article reports non-RDS-adjusted estimates from a diverse sample, but estimates should not be inferred to represent population-level estimates.
This analysis focuses on two key PMTCT approaches, including prevention of unintended pregnancy among FSW living with HIV or at high risk for HIV acquisition, and safe pregnancy planning needs for FSW desiring children. Thus, factors associated with an unmet need for contraception were assessed using robust Poisson regression to estimate crude (bivariate) and adjusted (multivariate) prevalence ratios (PRs) and 95% CIs. Models assessing unmet need for contraception use were restricted to FSW who reported that they were not currently trying to conceive. The outcome, unmet need for contraception, was defined as not using a highly effective method of contraception, including injectable or oral contraception, intrauterine devices (IUDs), implants, sterilisation or consistent condom use with all clients and non-paying partners during every sex act during the prior 30 days. Women who did not report any sex in the past 30 days with clients or non-paying partners (n=13) were considered to have met contraceptive need. Due to the high method failure rates women using barrier methods of contraception alone experience,12 separate PRs were modelled to assess associations between unmet need for a highly effective non-barrier method of contraception. Highly effective non-barrier methods included injectable contraceptive methods, combined oral contraceptives pills, implants, IUDs and sterilisation. Women using only the diaphragm or cervical foam/jelly (n=6) were considered to have unmet contraceptive need as the consistency of method use was not assessed and even the perfect method use failure rate exceeds 5%.12 PRs were also estimated to assess characteristics associated with currently trying to become pregnant. Women were asked if they were currently trying to become pregnant and those indicating affirmatively were considered to be currently attempting pregnancy.
Robust Poisson regression was used for model estimation as the frequency of the outcomes was greater than 10% (thus the odds ratio would overestimate the PR) and not all log binomial models reached convergence.16 Standard errors accounted for clustering between individuals emanating from the same recruitment seed by using generalised estimating equations. Age and study site were included in all multivariate-adjusted models. Additional characteristics were assessed in the bivariate models based on known relationships and hypotheses, and were included in the multivariate models if they were statistically significant in the bivariate analysis at the p<0.10 level. HIV status was self-reported during the interview and then confirmed through biological testing. Thus we report HIV status based on both self-report and actual biological testing, as reflected through the following categories: HIV-negative, HIV-positive previously diagnosed, and HIV-positive no previous reported diagnosis. Those who were living with HIV and refused to indicate a prior diagnosis were considered not to have a reported prior diagnosis (HIV-positive status unknown). Because all variables assessed had less than 1% missing data, we conducted complete case analyses.
Results
Demographics, HIV and reproductive history
Enrolment of 1705 FSW into cross-sectional RDS studies took place in Swaziland from July to October 2011, in Togo from January to June 2013, and in Burkina Faso from January to July 2013. HIV test results were not available for eight women who were excluded from the analyses. Women >49 years of age (n=31) were also excluded from this analysis. The characteristics of the remaining 1666 FSW are presented in Table 1. Demographic characteristics of participants varied across countries. Crude HIV prevalence in the study populations ranged from 18.3% in Togo to 70.3% in Swaziland.
Demographic overview of cohort overall and by country (n=1666)
The median age of FSW was 25 years [interquartile range (IQR) 22–32]. Overall 1372 (82.4%) women had ever been pregnant. FSW had a median of one living biological child (IQR 0–2). Of women reporting a prior pregnancy, 599 (43.7%) self-reported at least one prior unwanted or unplanned pregnancy when asked if they had ever had an unwanted or unplanned pregnancy. In Togo and Burkina Faso, 83 FSW with a child reported an HIV diagnosis prior to participation in the study, and of these women 12.1% (10/83) reported having a child known to be living with HIV (similar data were unavailable for Swaziland).
Contraceptive use
In terms of contraceptive use, 30% of all 1666 women were using highly effective non-barrier methods of contraception alone to prevent pregnancy, 17% relied on consistent condom use alone and 9% used dual methods – including a highly effective non-barrier method of contraception and consistent condom use with all partners – including clients and non-paying partners. A further 19% of FSW were trying to conceive. The remaining 25% of FSW had an unmet need for contraception. An overall breakdown of contraceptive use by country is detailed in Figure 1. Among women using highly effective non-barrier methods of contraception, 38.7% reported using injectable contraception, 37.3% oral contraceptives, 18.4% implants, 3.3% IUDs and 2.3% were sterilised. Contraceptive use, including condoms, highly effective non-barrier methods, and pregnancy intentions were similar among HIV-negative FSW and women living with HIV (p=0.21). Among the 1349 women not trying to conceive, 653 (48.4%) were using highly effective non-barrier methods with or without consistent condom use, 289 (21.4%) reported consistent condom use alone, and 407 (30.2%) reported neither using highly effective non-barrier methods nor condoms consistently. Overall, 518/1666 (31.1%) FSW reported that a condom had broken during sex in the past 30 days.
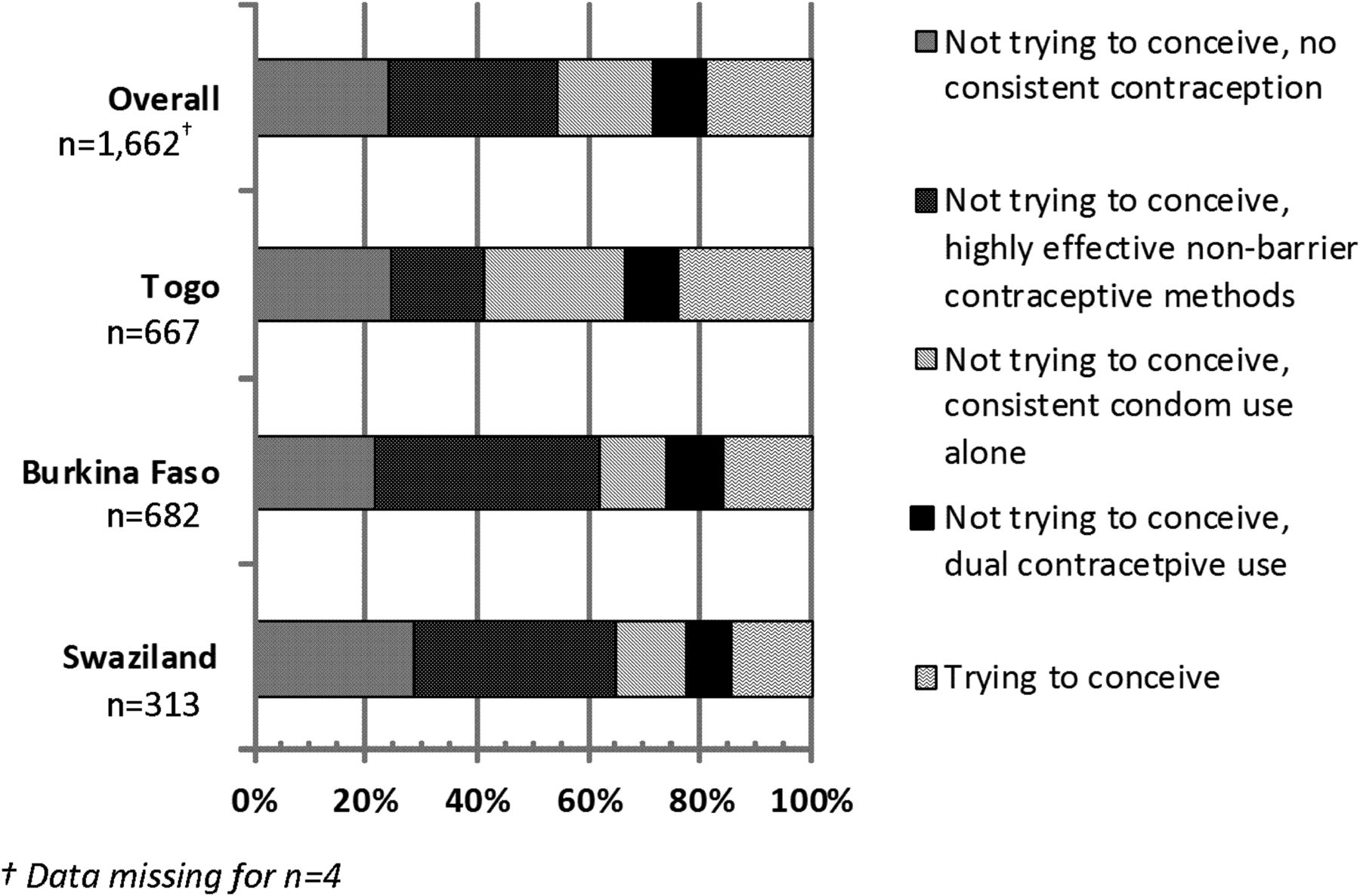
Contraceptive use and unmet contraceptive need overall and by country (n=1662).
Among the subset of women not trying to conceive, we assessed correlates of unmet need for contraception and separately correlates of not using a highly effective non-barrier method (Table 2). In the multivariate model, having a non-paying partner was associated with more than two times greater prevalence of unmet contraceptive need as compared to women only reporting sex with clients during the prior month. Unmet contraceptive need was 21% lower among FSW with one child and 37% lower among FSW with two or more children as compared to women without children. When considering highly effective non-barrier methods specifically, several factors were associated with unmet need for highly effective non-barrier method use in the bivariate analysis (Table 2). In the multivariate models, women were statistically significantly more likely to have an unmet need for highly effective non-barrier methods if they were older (≥35 years compared to 16–24 years), born in a country different from where they currently reside, and if they reported consistent condom use. Associations with highly effective non-barrier method use (those factors inversely associated with the outcome) included having one or more children and a prior history of being raped.
Associations between unmet need for contraception among female sex workers not trying to conceive
Analyses stratified by country were run to assess evidence of heterogeneity in associations observed across the study sites. Inferences were the same in the stratified analyses, with the exception of HIV status. FSW who were HIV-positive and aware of their HIV status in Burkina Faso had greater unmet need for contraception as compared to HIV-negative women, a relationship not observed in the other countries. Additionally, FSW living with HIV who reported a prior HIV diagnosis in Togo and Burkina Faso were more likely not to be using a highly effective non-barrier method as compared to HIV-negative women. HIV-infection status was not independently associated with highly effective non-barrier method use in Swaziland (results not shown).
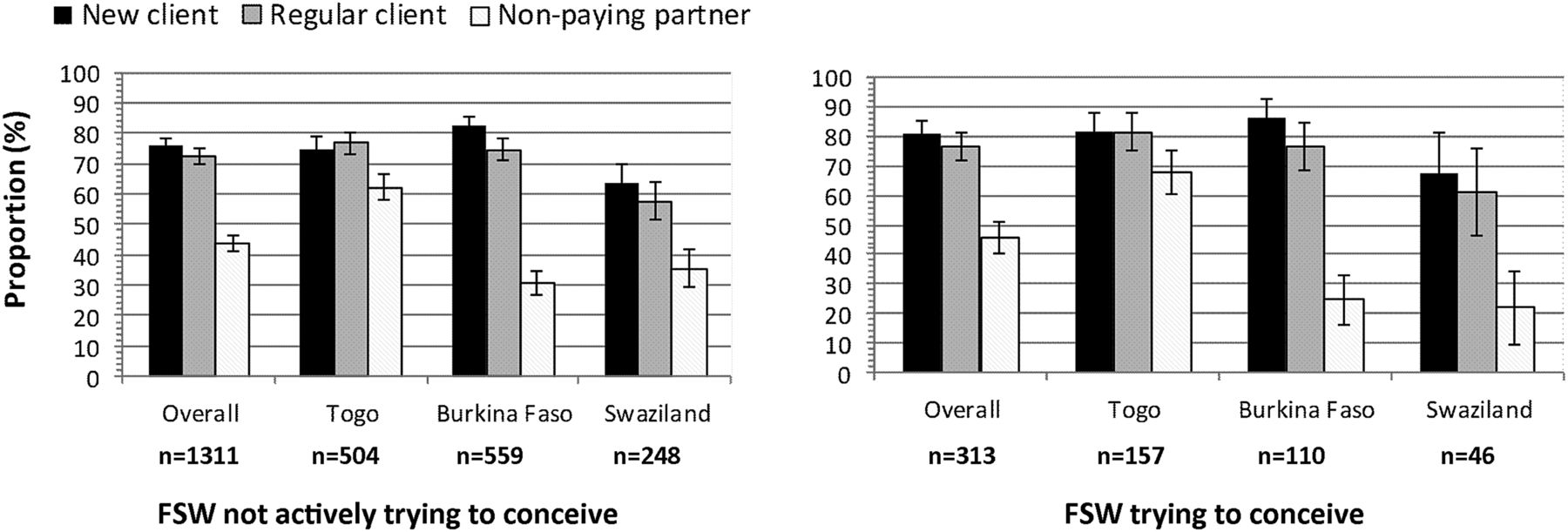
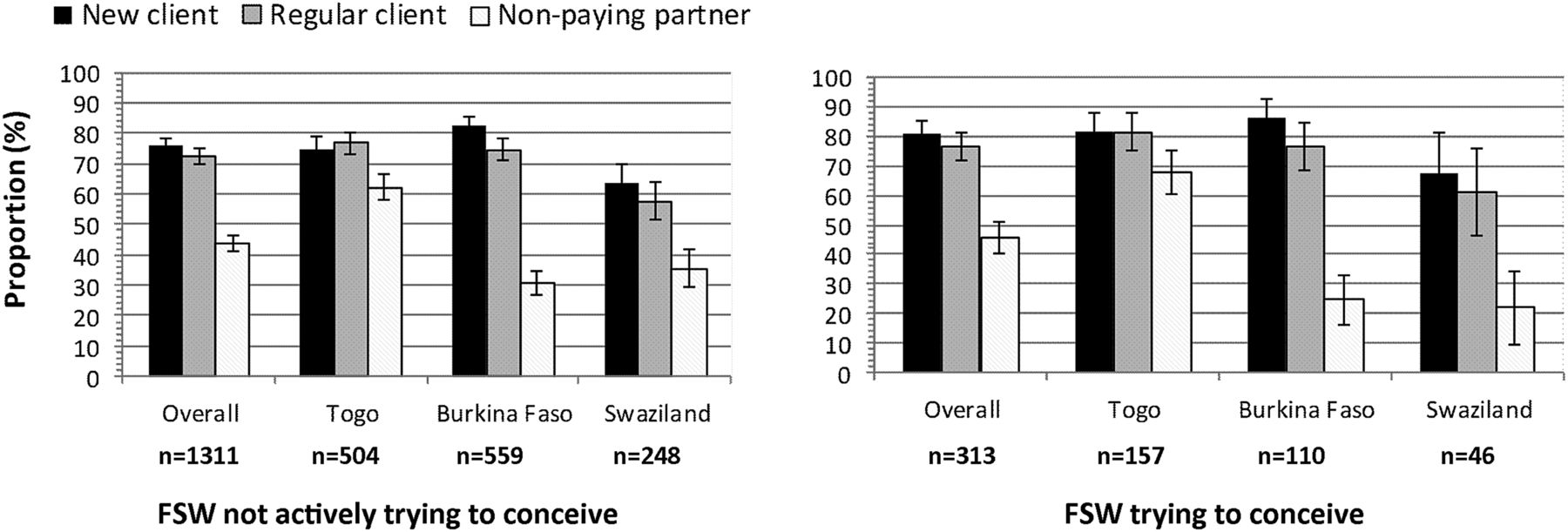
Overall one-third of FSW not trying to conceive (n=442/1349) reported consistent condom use with new clients, regular clients and non-paying partners during the prior 30 days; consistent condom use with partners was similar among the 313 women trying to conceive (36.7%, p=0.18). As illustrated in Figure 2, consistent condom use varied substantially by partner type, with >70% of FSW reporting consistent condom use with clients in most settings, but much lower reported use with non-paying partners. This trend was observed regardless of whether women were currently trying to conceive. Among women not trying to conceive, consistent condom use was similar among FSW who felt it was important to avoid pregnancy (32.4%), as compared to women who were also not trying, but less concerned about whether or not they became pregnant (36.4%, p=0.34). Effective non-barrier method use between these two groups, however, was significantly different (49.8% vs 37.1%, respectively; p<0.01).
{kind=link}
{kind=link}
Condom use during all sex acts in the past 30 days by partner type and by whether women are currently trying to conceive across countries. FSW, female sex workers.
Current fertility desires and attempted pregnancy
Nineteen per cent of all FSW enrolled reported that they were currently trying to conceive. Women with no children or only one child were far more likely to be trying to become pregnant as compared to women with two or more living children (Table 3). Additionally women who were living with HIV, but undiagnosed, were more likely to be trying to conceive as compared to FSW who were HIV-negative. Among women trying to conceive, 16% reported that they had avoided health care services in the past and 23% had experienced difficulty accessing care. Of 98 women living with HIV trying to conceive, 25 (25.5%) were currently receiving ART. Any self-reported symptoms or reported diagnosis of a sexually transmitted infection (STI) in the past year were common among FSW trying to become pregnant (40.9%), and many of these cases had reportedly not been treated (37.6%).
Associations between female sex workers reporting that they are currently trying to conceive
Discussion
These analyses highlight potential gaps in PMTCT programming efforts for FSW. Firstly, FSW had significant and consistent unmet contraceptive needs across countries. Overall 41% of women not currently trying to become pregnant were relying on consistent or inconsistent condom use as their contraceptive method. Unmet contraceptive need was equally high among FSW living with HIV as compared to HIV-negative FSW. We also found that nearly one in five FSW were trying to become pregnant and that women living with HIV, but reportedly undiagnosed, were most likely to be currently trying to become pregnant.
The findings reinforce those of other researchers working in Russia, India and Kenya who have demonstrated a high unmet need for contraception and need for reproductive services for FSW.7 ,17–19 Both highly effective non-barrier contraceptive methods and HIV testing are available within primary health centres in these settings, but making services more convenient may facilitate better uptake of these services. Moreover, among FSW not trying to become pregnant in our analysis, contraceptive use was similar between HIV-negative women and women living with HIV, underscoring the potential risk for HIV mother-to-child transmission (MTCT) in the context of unplanned pregnancy.
A full understanding of unmet contraceptive need is complicated among FSW as fertility desires may not be universal across partners (e.g. non-paying partners versus clients). The methods most reliable to prevent pregnancy with clients, such as injectable methods, the IUD or the implant, cannot be used by women who are trying to conceive with husbands or other non-paying partners. Although consistent condom use is important for both preventing HIV as well as unintended pregnancy, nearly one-third of the women in our studies reported condom breakage in the past month, underscoring that reliance on condoms alone for contraception may be insufficient. In fact, reported levels of consistent condom use were comparable between women who were and were not trying to conceive in our study, suggesting that HIV prevention rather than contraception may be the driving motivation behind condom use. Further assessment of when FSW trying to conceive use or forgo condoms with partners (e.g. timing in relation to her menstrual cycle, HIV status of partner, etc.) is important in order to understand what risk reduction methods for HIV acquisition or transmission women are employing or could improve upon during attempted conception.
While positive fertility desires have been documented before among women engaged in sex work,11 ,19 our cross-country data demonstrate the PMTCT importance of considering conception, not just contraception, as part of family planning programming for FSW. In this analysis, FSW living with HIV but without a previous reported HIV diagnosis were 51% more likely to be trying to become pregnant as compared to HIV-negative FSW. Moreover, only 25% of HIV-positive FSW trying to become pregnant were on ART, increasing the probability of HIV acquisition among partners and infants. Safer conception care to FSW is thus necessary to minimise HIV acquisition among FSW trying to conceive, as well as onward transmission to sexual partners of HIV-positive FSW and infants. Preconception approaches for FSW and women living with HIV in general may include STI screening and treatment, HIV testing, provision of folic acid, determination of ART eligibility, and ART when eligible for women living with HIV.20–22
Data documenting MTCT of HIV rates among FSW are largely unavailable. Given the frequency of pregnancy among FSW,2 ,3 PMTCT programming efforts targeting FSW should be prioritised and evaluated. In our data from Togo and Burkina Faso, 12% of FSW who had a child and reported a known HIV diagnosis had at least one child living with HIV. This subsample is small, but indicates that HIV MTCT may be high among FSW. National PMTCT coverage estimates in Burkina Faso, Swaziland and Togo are 66%, 83% and 86%, respectively, among women known to require PMTCT,14 and whether FSW are equally likely to reached by PMTCT is not known. Data from India suggest that the majority of FSW continue working throughout pregnancy, have limited knowledge of PMTCT, and do not access antenatal care half of the time.7 Taken together these data suggest that risk of vertical transmission may not be evenly distributed across all women living with HIV, though studies to characterise actual MTCT rates among FSW are needed to confirm these PMTCT gaps.
These analyses have several limitations. HIV infection among children of FSW in Togo and Burkina Faso is limited by self-report, high burden of undiagnosed maternal HIV, and likely undiagnosed cases of paediatric HIV. Importantly this data is cross-sectional and temporality cannot be assessed, including whether or not a woman had children before entering sex work or after, and whether or not HIV infections were acquired before or after pregnancy. Future work in this area is needed to fully assess the dynamics around pregnancy, sex work and HIV infection risk. Additionally, data were only collected on the basis of whether women were currently trying to conceive, and the partner with which the FSW was trying to conceive was not assessed. Fecundity was not assessed in these studies, and it is likely that some women indicated as having an unmet contraceptive need were infecund given the frequency of STIs among FSW. Furthermore, although data collection methods were consistent across studies, caution is needed when interpreting the pooled data and results may not be generalisable to other FSW. Although data collection in Swaziland commenced 18 months prior to the other study sites, secular trends were likely to have had less of an effect in this analysis than regional- and country-level differences between HIV epidemics in West and Southern Africa. Stratified analyses were conducted to assess heterogeneity in findings across settings, and although demographics of FSW differed across studies, regression models of associations were largely robust across settings, suggesting that similar reproductive health experiences were present across diverse settings. Finally, we performed secondary analyses that did not directly account for the RDS-sampling methods, which may have resulted in an underestimation of the standard errors. We have used generalised estimating equations to help account for this impact on the standard errors by accounting for clustering within recruitment networks; however, caution is advised in the interpretation of any results in which CIs approach equivalence.
Overall, in our study FSW had both unmet needs for contraception and attempted conception in the absence of routine HIV testing and care among FSW, which pose serious, but addressable, MTCT risks. Voluntary, reliable contraception options, including long-acting methods such as the IUD or implants, should be promoted and importantly are reversible. There is a critical need to also improve consistent condom use with clients, but particularly with non-paying partners of FSW. Furthermore, effective family planning cannot be limited to the prevention of pregnancy, but must encompass preconception and pregnancy needs of women – frequently missing components of family planning approaches.23 ,24 The complexity of different reproductive goals across different types of partners among FSW requires open conversations between health care providers, peer educators and FSW about the advantages and disadvantages of different pregnancy prevention and safer conception strategies. Reproductive goal setting, access to quality services, and early engagement in the HIV treatment cascade among FSW are critical to reduce MTCT risks and promote health among women and infants.
Acknowledgments
The authors are deeply grateful to the women who participated in the studies and to the community groups who provided invaluable insights before and throughout the implementation and analysis phases for these studies. This work could not have been completed without the dedication of the study team members across countries and study sites. The authors are indebted to their commitment to making these studies happen.
References
Footnotes
Funding This work was supported by Project SEARCH, which was funded by the United States Agency for International Development under contract GHH-I-00-07-00032-00, and by the President's Emergency Plan for AIDS Relief.
Competing interests None declared.
Ethics approval Swaziland Scientific and Ethics Committee, the Health Research Ethics Committee of Burkina Faso, the National Ethics Committee of Togo and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data related to sex work may be available from Swaziland, Burkina Faso and Togo upon request. Those interested in working with these data should contact Stefan Baral at sbaral@jhu.edu.
Linked Articles
- Highlights from this issue