Article Text

Abstract
Introduction One of the major concerns with the insertion of intrauterine devices is uterine perforation. Though uncommon, it can be debilitating and result in failure of the device. In this article we review uterine perforation with intrauterine contraception (IUC) in a community clinic in the UK over a 16-year period.
Methods We prospectively collected data on uterine perforations for the years 2000–2015, reviewed associated factors and calculated the annual rate of perforation, estimating if this lay within the expected range of normal variation using statistical process control (SPC) analysis. We analysed the rates of perforation in relation to the time from delivery and to breastfeeding.
Results We identified 30 uterine perforations in 22 795 IUC insertions over the 16 years of observation, with an annual rate ranging from 0 to 4.3 per 1000 insertions, and a mean annual rate of 1.3 per 1000 insertions (95% CI 0.9 to 1.9), which remain within the SPC limits. Twenty-eight of the perforations were in parous women, 87% of whom were within 18 weeks of delivery, peaking at 13 weeks postpartum. Twenty of these were in breastfeeding women. In 3/28 cases for which we have outcome data the device was adherent to or had perforated either the bladder or bowel.
Conclusion Our perforation rate is consistent with other studies. Most of our perforations were within 18 weeks of childbirth, earlier than in a recent major study. We cannot tell from our data if there is a true peak in perforations 3 months postpartum as that may be a time when a high proportion of insertions are done.
- intrauterine devices
- intrauterine systems
- family planning service provision
- ong-acting reversible contraception
- uterine perforation
Statistics from Altmetric.com
- intrauterine devices
- intrauterine systems
- family planning service provision
- ong-acting reversible contraception
- uterine perforation
Key message points
Our mean rate of known uterine perforation following intrauterine contraception insertion (1.3/1000) is consistent with the findings of other studies.
The peak in the number of perforations was around 3 months after delivery and 20/30 perforations were in breastfeeding women.
Facilities for urgent ultrasound in a community contraception service are useful for early detection of perforations or for reassurance of correct fitting position.
Introduction
Uterine perforation following insertion of an intrauterine contraceptive (IUC) is infrequent, and is reported to occur within the region of 1–2 per 1000 insertions.1 2 However, the consequence can be significant as the device may require surgical removal, can damage pelvic and abdominal organs and result in an unwanted pregnancy. In this study we review the perforations accumulated in our Inner West London community contraception and sexual health service over the past 16 years.
The aim of the study was to estimate the rate of perforation, to identify trends and any associated factors, and to compare these to the initial 1-year results of the EURAS-IUD cohort study, which found a higher rate of perforations in women who were breastfeeding and in those who were less than 36 weeks postnatal.1
Methods
We performed a retrospective analysis of known perforations. All IUC insertions in our community contraception and sexual health clinics in West London during 2000–2015 were eligible for inclusion.
Women were routinely followed up at 6 weeks. In the early years we also did routine checks at 6 and 12 months and then annually, but more recently we followed up at 6 weeks only, unless a woman had a problem.
Cases of known perforation were reported to the clinical lead at the time of detection. A few were discovered at audit where the case was known to an individual clinician but not previously reported. We included both partial perforations, where the device was embedded in the myometrium, and complete perforations, where the bulk of the device had passed through the serosal surface of the uterus or was lying in the abdominal cavity entirely outside the uterus, requiring removal via the abdominal route.
The notes of each case were reviewed. We looked for any possible factors that indicated that the clinician fitting the device could have identified the perforation at the time, and any potential risk factors. We reviewed the type of device as well as any personal and medical factors for the woman, including the type of delivery if postnatal, breastfeeding status, time from delivery, parity and any significant documented insertion findings, for example, need for dilation. Notification of each perforation was followed by a discussion with the inserting clinician, who was asked to review the case and fill out an incident form with any reflection on lessons learnt. Any correspondence from secondary care was also included in the review.
The rates calculated were based on the total number of insertions per year over 16 years. We plotted the number of perforations per year and the moving average number per year, which smoothed the curve by adjusting for the rate in the previous 4 years and the following 1 year (lag 4/lead 1). We graphed the number of perforations against number of postnatal weeks and used kernel density estimation to smooth the data. We calculated the cumulative number of perforations against time from delivery, and compared perforations among breastfeeding and non-breastfeeding women.
In view of the inevitable natural variation of biological measurements (in this case the annual uterine perforation rate), a method of assessment was required that would distinguish between random variation and an excess in any particular year. Statistical process control (SPC) allows investigators to draw limits within which random variation occurs. SPC is a branch of statistics that combines rigorous time series analysis methods with graphical presentation of data to assess the stability of processes and to detect meaningful change over time. SPC enables the differentiation of usual, random variation due to inherent factors within the process, from special cause variation, which is indicative of an external influence on the process. This could indicate a sustained deterioration, or improvement, in performance.3 4
Here we used SPC to see if the rate of perforation of IUC devices in our service in any 1-year period was within recognised and expected limits, derived from the rates in previous years. We plotted the mean annual rates of perforation, along with the upper and lower control limits, which are three standard deviations from the mean. If the ‘process’ of IUC insertions is ‘in control’, 99.7% of observations should lie within the control limits and there a probability of 0.0027 of any point exceeding those limits by chance. If the rate of perforation exceeds the upper control limit it is indicative of special cause variation, and requires further investigation to identify any causative factors.
While our service underwent organisational changes during this time, initially as Parkside Services for Women, then merging with Riverside Contraceptive Services to form Westside Contraceptive Service, and finally with Barnet within the Central London Community Healthcare NHS Trust, the service provided varied little over this period, apart from more frequent follow-up in the early years.
All analyses were done in Stata 13.1 (StataCorp, 2013. College Station, Texas: StataCorp LP).
Ethical approval was not required as this study was retrospective and had no bearing on the management of the women under our care.
Results
We inserted 22 795 IUC devices between 2000 and 2015 and identified 30 perforations in that period. Of the perforations following delivery, all were interval insertions performed more than 4 weeks after childbirth, apart from one at 3 weeks and 6 days. The median age of the women with uterine perforations was 34.1 years. The numbers of perforations remained fairly constant over the 16 years with a moving average of around two per year (figure 1).
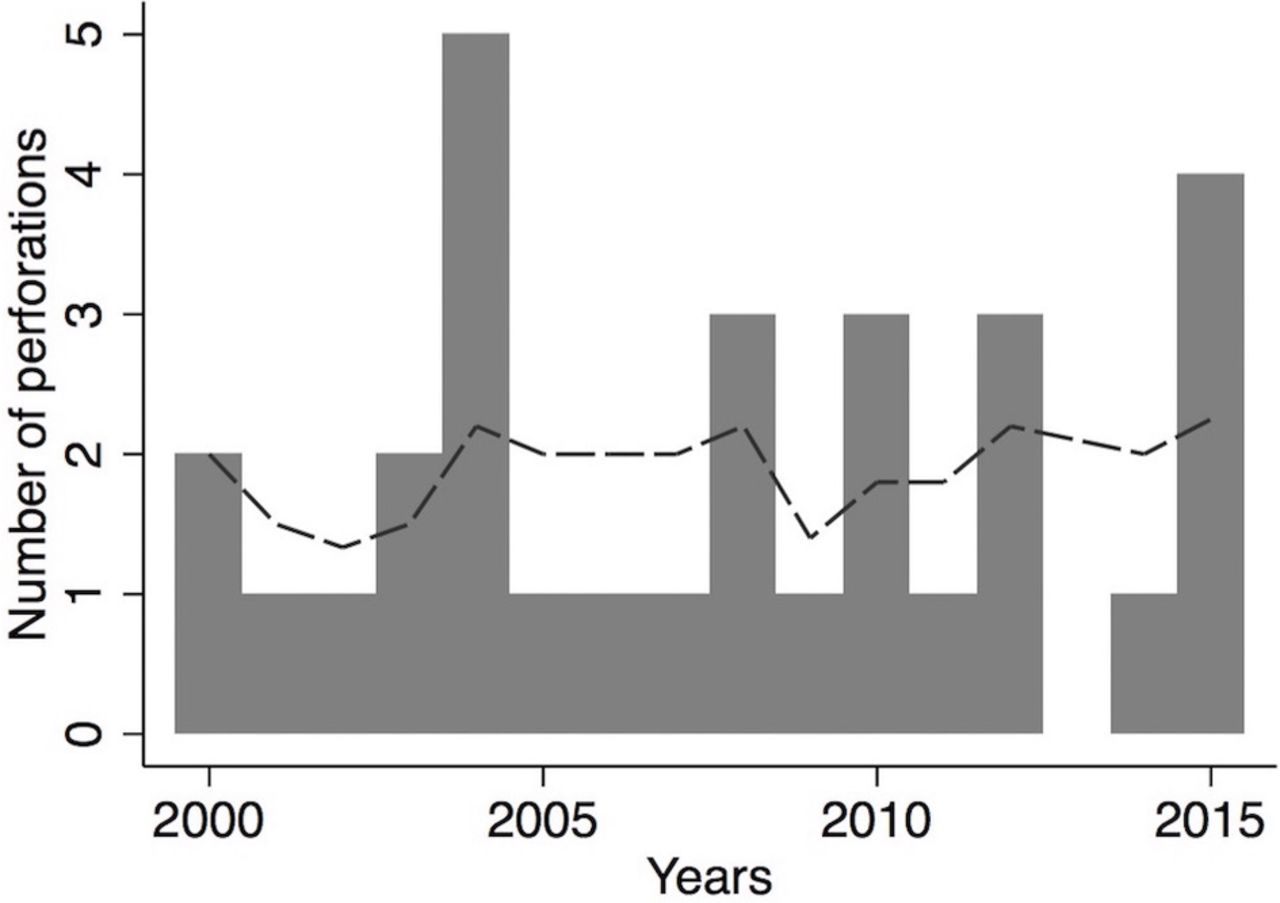
Number of perforations per year (n=30). Moving average around 2 per year (dashed line).
Figure 2 shows the proportion of IUC devices that perforated per year, which ranges from 0 to 4.3/1000. In all years the rate was below the SPC upper confidence limit, which dropped from around 5/1000 to 4/1000 as the number of devices inserted per year increased. The mean annual perforation rate was 1.3/1000 insertions (95% CI 0.9 to 1.9). There were no indications that the variation observed was beyond what would be expected by chance, as the annual rates were at all times below the upper control limit.
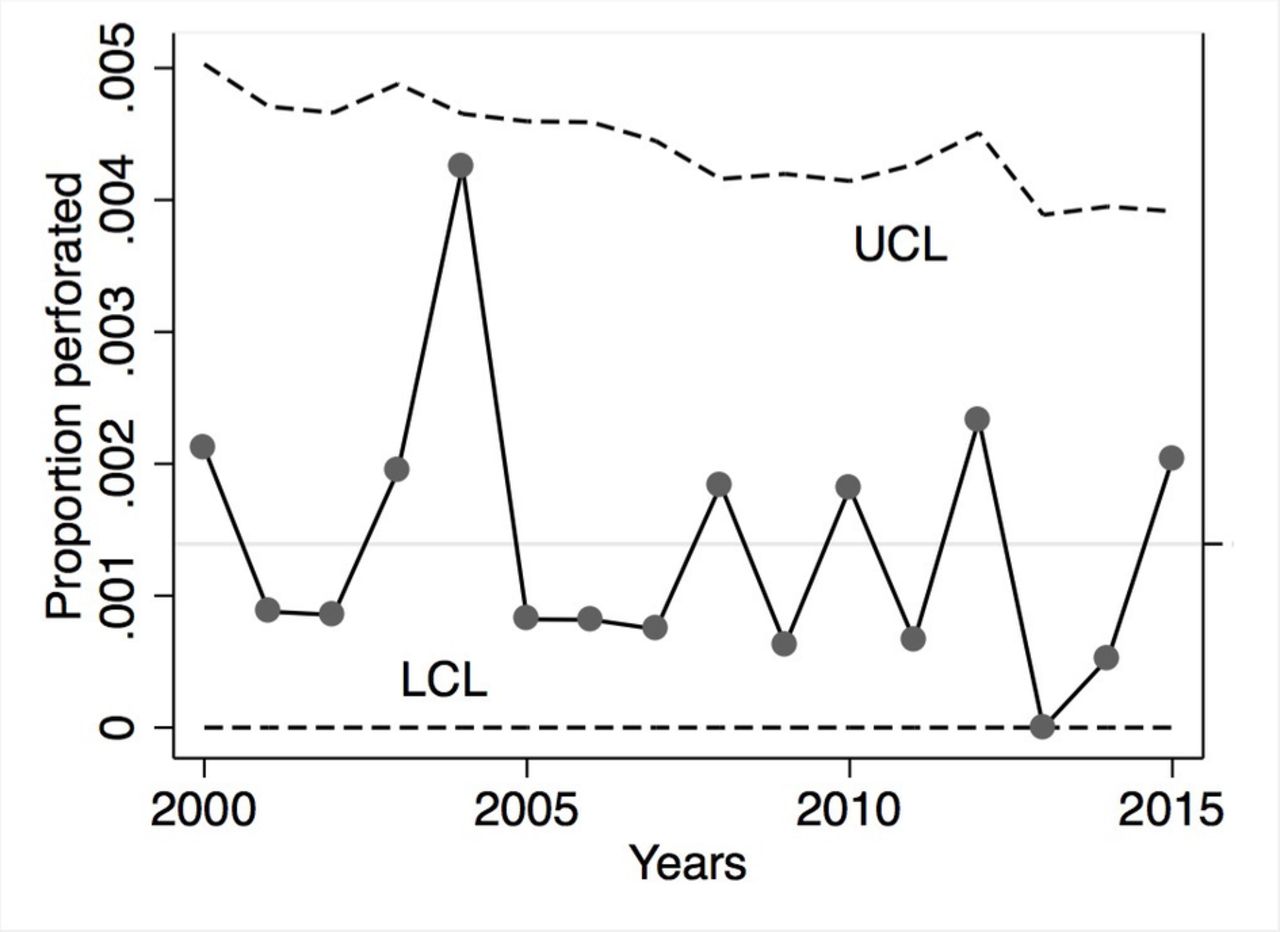
Proportion of perforated devices per year (n=30), with the upper (UCL) and lower (LCL) confidence limits of the statistical process control.
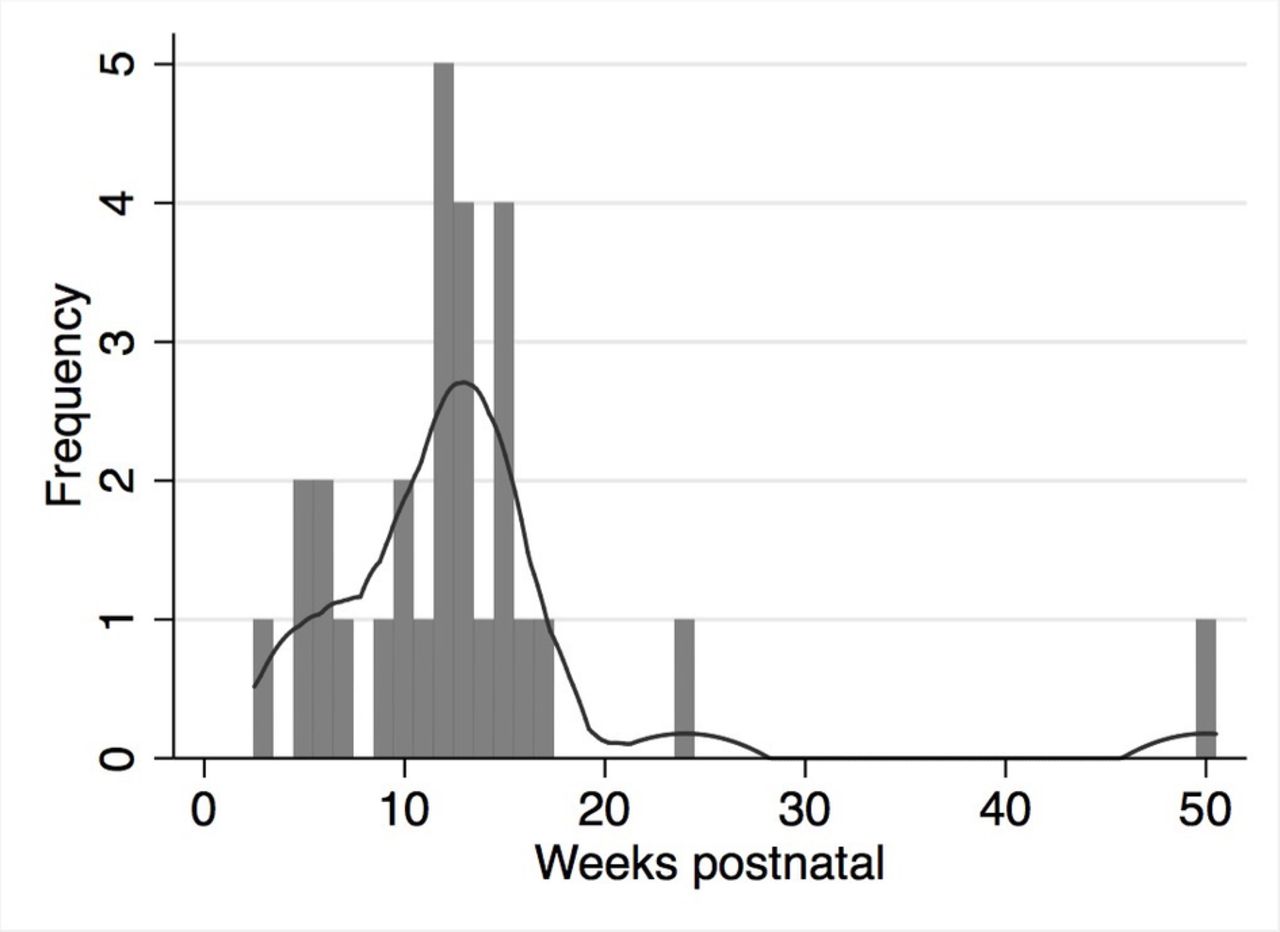
Of the 30 known perforations, 28 were in parous women, 26 (87%) within 18 weeks of delivery. Figure 3 shows the number of perforations peaking at 13 weeks after delivery in the smoothed plot.

Number of perforations and weeks postnatal (n=28). Peak number around 13 weeks postnatal (kernel density plot – solid line).
Twenty of the 30 perforations (66%) were in women known to be breastfeeding at the time of the insertion. The timing of the perforation in relation to delivery did not appear to be affected by breastfeeding status (figure 4). Ten of the 30 perforations (33%) were in women who had had a recent caesarean section. Of these 10, the frequency peaked at 12.5 weeks after delivery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative proportion of perforations by weeks postnatal (n=28) and breastfeeding status at insertion (n=28) (vertical dashed line at 13 weeks).
Table 1 shows the types of device that perforated. No specific device appeared to have a higher risk of perforations as the numbers roughly corresponded to the use of the devices in those years. Twenty of the 30 perforations were complete. Twenty different doctors performed the insertions and no individual clinician appeared to have a higher risk of perforations (data not shown).
For the 28 cases where we had outcome data, six devices were removed in the contraception clinic, two at hysteroscopy, and 18 were removed at laparoscopy, one of which was reported as being ’removed from the ileum’. Two further cases were complicated and are detailed below. Five women conceived as a result of their undiagnosed perforations.
In one complicated case the device was inserted into a ‘bulky’ uterus with a cavity length of 12 cm. The patient reported abdominal pain at the time of insertion and thereafter continuously for 4 months, by which time she was pregnant. An ultrasound scan was unable to locate the IUD but a subsequent scan demonstrated the device in the Pouch of Douglas. At laparoscopy, removal failed as the device was densely adherent to the sigmoid colon and erosion into the bowel could not be excluded. Removal was deferred fearing disturbance of the pregnancy. The patient later miscarried and required evacuation of retained products of conception. Sigmoidoscopy at that time showed intact bowel mucosa. Finally, the device was removed at a second laparoscopy 8 months after insertion. The operation note stated ‘lodged in sigmoid colon/mesentery, tethered by scarring, scarring dissected off and the IUD was removed’.
Patient characteristics, devices used and features of perforation and removal (n=30)
In the other case a device was inserted following failed insertion by a general practitioner. The insertion was apparently normal. When seen 6 weeks later the woman reported intermittent lower abdominal pain and the IUD threads were seen. A month later she had a positive pregnancy test. An ultrasound scan was unable to locate the device. Following a normal vaginal delivery, no attempt was made to locate the device. Three months later she attended an accident and emergency department with severe lower abdominal pain and inability to pass urine. An ultrasound scan did not identify the device but it was seen on X-ray. At mini-laparotomy the device was seen partially perforating the bladder, and following cystoscopy the device was removed abdominally. A check cystoscopy 6 weeks later was normal.
Discussion
We identified 30 uterine perforations by IUCs in our series of almost 23 000 insertions, giving a perforation rate of 1.34/1000. As an ad-hoc case finding method was used this is the minimum number of perforations and there are likely to have been others, which we have not been able to assess. Our rate is similar to the overall rate (1.28/1000) in the large prospective EURAS-IUD study in which there were 81 perforations in 61 000 insertions at 1-year follow-up with a low rate of loss to follow-up (2%).1 The final rate in that 5-year study is expected to be higher. In a cohort study of a single device (Multiload Cu375) in 16 000 women, Harrison-Woolrych et al found that almost half (13/28) of the perforations were detected more than 1 year after insertion.5 We can therefore expect more perforations to be detected from insertions in the latter part of the 16 years of our own study. In a prospective study of 8000 insertions from a teaching hospital where all women were scanned 12 months after insertion of TCu380A IUDs, without prior sounding of the uterus, the perforation rate was 2/1000.6
Data from 53 000 insertions of copper IUDs performed more than 6 weeks after delivery were compiled by the WHO from 26 studies and showed an average perforation rate of 0.6 per 1000 insertions.7 Commenting on this Meirik stated ‘With family planning providers well trained in the insertion of modern copper IUDs, and with optimally designed inserter tubes, this potentially serious complication should be almost completely avoided’.8 In a subsequent WHO randomised IUD trial, the largest such trial to date, it was reported that there were no uterine perforations in over 2000 insertions of the TCu380A and a similar number of the Gynefix frameless IUD at 8 years of follow-up.9 Whether this was due to superior training or the absence of imaging technologies is not known.
All services providing IUC need to monitor their uterine perforation rates and it is therefore necessary to know whether the rate in any particular year is excessive. A medical director may need assurance that an unexpectedly high rate is, in fact, within the bounds of normal routine variation. In 2004 we had an unexpectedly high perforation rate but our SPC demonstrated that this rate was in fact within the bounds expected from normal statistical variation. The control limits do not tell us if our rates were above or below those experienced elsewhere or whether these rates were acceptable. However, they do provide a robust method to detect variation in rates of perforation in an individual service that warrant special attention. To produce a valid control SPC chart, a minimum of 10 data points are needed, so historical records of perforation rates are necessary. The variation over the 16-year period was stable and in control around a mean of 1.3/1000. This gave us some assurance that the rates were not statistically excessive for our service.
Almost all the perforations in our series occurred when insertions were done within 18 weeks of delivery, with only 2/28 occurring later than this, suggesting that the rate is very low for insertions after that time. For the EURAS-IUD study1 the data were dichotomised before and after 36 postnatal weeks ‘following inspection of the data’, which suggests a tailing off of the risk of perforation after 36 weeks. In our series almost all the perforations occurred within half that time. In the absence of data around the timings of all postnatal insertions it is not possible to draw conclusions from our study about the risks in relation to time from delivery. It is possible that more insertions are done at 13 weeks in our service and a peak in perforations is simply a reflection of this rate.
Our data are unable to inform the important decision of whether delaying insertion after childbirth will reduce the risk of perforation, as we do not have data on time of insertion from delivery for those without a perforation. In the 1-year interim report of the EURAS-IUD study1 the trend in rates of perforation in relation to time from delivery was not published, apart from the rate before and after 36 postnatal weeks. This information is important, as it could be of significance for women who choose to delay their IUC fitting because of the perforation risk, and we would hope the final report of that study will provide that information.
Twenty of the 30 perforations (66%) were in women who were breastfeeding at the time of the insertion which is higher than the 43% in the EURAS-IUS study, in which 35/81 perforations occurred in women who were breastfeeding. This may simply reflect different breastfeeding rates in the two cohorts. Our study appears to corroborate the hypothesis that breastfeeding is a factor in perforation risk, although it does not demonstrate causation. In a recent high-quality systematic review of the safety of IUDs in breastfeeding women Berry-Bibee et al concluded that breastfeeding was a likely causative factor.10
The assessment of risk of perforation from time from delivery to insertion, however, is confounded by the risk associated with breastfeeding, as lactation rates are inversely related to time from delivery. While logistic regression analysis will tell us the relative risk associated with each variable, a stratified analysis is more useful for women considering IUC after childbirth as it can give an estimate of the absolute risk. The EURAS-IUD study found that breastfeeding and time from delivery to insertion were independent risk factors. The perforation rate for women who had both an insertion within 36 weeks of delivery and were breastfeeding was 5.6/1000 while the rate for women with neither risk factor was 0.7/1000.1 Interestingly, in our study the proportion of perforations in relation to time from delivery was similar among breastfeeding and non-breastfeeding women. Neither the type of device nor a history of caesarean section appeared to be significant risk factors in our study.
Uterine perforation can have serious consequences. At least two women in our series had extended pain and associated distress, with internal organ involvement. The EURAS-IUD study concluded that ‘there was an absence of serious sequelae should perforation occur, such as bowel or bladder injury, septicaemia or peritonitis’, but this can downplay the significance of the perforation. The two complicated cases reported here had prolonged impact on the women’s lives. In both there were errors not just in the insertion but also due to delayed detection. Any case requiring surgical intervention is significant for the individual, particularly for women with a new baby. Avoidance of perforation, or rapid diagnosis should it occur, could reduce the sequelae.
There are also consequences for the organisation (reputation and litigation) and the clinician (reputation, anxiety and loss of confidence). Litigation is unlikely to succeed if the woman has been appropriately counselled, the counselling documented, and the perforation detected early on follow- up and managed accordingly. Nevertheless potential perforation is a significant concern among clinicians and this may contribute to the reluctance of some clinicians and women to choose IUC, particularly for those perceived as having a higher risk of perforation.
A major weakness in our study is that we have follow-up data only on those women with known perforations. The number reported is therefore the minimum number. Ultrasound facilities have been available during the second half of the period of this study, and women with a partial perforation may well not be diagnosed without this investigation.
Most of the data in this study were drawn from a period in which a 6-week follow-up appointment was standard practice in the UK. It will be interesting to see if late diagnosed perforations become more frequent following the change in advice in 2015 by the Faculty of Sexual & Reproductive Healthcare (FSRH), in which this visit is no longer deemed essential.11
While studies have found that perforation rates are lower among clinicians who have performed more insertions,1 12 in our study perforation occurred even among the more experienced clinicians. While the role of training is very important, it appears that in our service perforation of the uterus with IUCs will not be eliminated. However, it is clear from the description of the two serious cases above, one of which resulted in legal action, that standards of care were deficient in some cases.
Following the publication of the EURAS-IUD study, some clinicians have decided to delay insertions until 3 months after delivery in the belief that later insertion lowers the risk of perforation. While this study cannot show causation, the highest numbers of perforated devices occurred around 3 months after delivery, although we were unable to determine if the rate is highest at this time. There is concern about delay in commencement of a woman’s preferred contraceptive method, as she may be at risk of pregnancy. She may also be inconvenienced by having to attend the service twice, and she may not return. Our guidance to staff is to follow the FSRH guidelines on Contraception After Pregnancy 13 and Intrauterine Contraception,11 where it is advised that if IUC placement is not done immediately postplacentally, it should be done at 4 weeks or more after either caesarean section or vaginal delivery. Future research is required to identify more accurately the increased perforation risk at different times of IUC insertion after delivery, and if there is a significant difference in outcome if the perforation is identified early after insertion. This may have consequences for the provision of ultrasound facilities in specialist services.
All the data in this study were collected from one service, which may be a weakness of the study as it limits the generalisability of the results. Our service acts as a referral centre for difficult insertions, which could potentially create an increase in the perforation rate.
Caliskan et al found that 50% of 18 perforations occurred in the posterior wall of an anteverted uterus or the anterior wall of a retroverted uterus.6 It is possible that relatively rigid introducer tubes may not follow the contour of an acutely anteflexed or retroflexed uterus and may lodge in the wall of a recently pregnant uterus, especially if the woman is breastfeeding. Plastic, or metal curved, uterine sounds may reach the fundus of a vulnerable uterus that straight IUD introducers cannot. Development of softer, more pliable introducers, or ones that can be bent to the shape of a uterus, may be warranted, although demonstrating a reduction in perforation risk would require large randomised studies. A surrogate endpoint, such as location of the device by ultrasound immediately after insertion, may allow high-quality, but smaller, randomised trials.
The findings here, combined with those of the EURAS-IUD study and advice from the UK Medicines and Healthcare Products Regulatory Agency,14 led us to develop a protocol to minimise the risk of perforation and to aid early diagnosis. Our service has in-house ultrasound facilities, which can be accessed easily.
Our protocol includes:
The importance of counselling about the excess risk of perforation after delivery
Having a higher index of suspicion for perforation when insertions are performed after delivery
Advice to abandon the insertion attempt if the procedure is unexpectedly difficult or there are other signs or symptoms that might suggest a possible perforation
A list of criteria for urgent referral for in-house ultrasound.
Acknowledgments
The authors thank Jem Ramazanoglu at Central London Community Healthcare NHS Trust for advice on statistical control methods. They also thank the peer reviewers for their valuable comments. Both authors moved to Central North West London NHS Trust in April 2017.
Footnotes
Contributors The concept for the paper POB, review of case notes POB and SP, analysis POB, writing by SP and POB.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue