Article Text

Abstract
Objective This systematic review and meta-analysis assessed whether enhanced peri-abortion contraceptive counselling had an effect on subsequent unplanned pregnancies and the uptake and continuation of contraceptive methods.
Methods and materials A systematic review of English-language articles published prior to May 2014 was conducted, using MEDLINE, EMBASE and the Cochrane Library. Only randomised controlled trials (RCTs) involving enhanced pre- and post-abortion contraceptive counselling were included. The authors independently applied the inclusion and exclusion criteria to the identified records, and extracted data from each included paper using a predefined extraction form. Risk of bias was assessed using the Cochrane Collaboration's tool. Meta-analyses were undertaken where appropriate and based on random effects models.
Results Six RCTs met the inclusion criteria. Three RCTs investigated the effect of enhanced counselling on subsequent unplanned pregnancy. The results of the meta-analysis were non-significant [pooled odds ratio (OR) 0.47; 95% confidence interval (95% CI) 0.12–1.90]. Four RCTs reported results relating to the uptake of long-acting reversible contraception (LARC) and continuation of chosen method of contraception at 3 months. Findings were non-significant (pooled OR 1.07; 95% CI 0.20–5.69 and pooled OR 3.22; 95% CI 0.85–12.22, respectively).
Conclusions This review found no evidence of effect resulting from enhanced peri-abortion contraceptive counselling on subsequent unplanned pregnancy rate or the uptake of LARC. However, these findings are limited by the small number of relevant studies available and the marked heterogeneity between published studies. Further, larger-scale RCTs should be undertaken to ensure that there is sufficient power to detect an effect.
- abortion
- counselling
- long-acting reversible contraception
Statistics from Altmetric.com
Key message points
This review found no evidence of effect of enhanced counselling on uptake of long-acting reversible contraception or subsequent pregnancy.
This may be due to heterogeneity between studies. Therefore we recommend that further research is conducted as some studies reported evidence of effect.
Introduction
Approximately one in three abortions carried out in the UK is performed on a woman who has previously undergone the procedure. A ‘repeat abortion’ is defined as a woman having two or more induced abortions in her reproductive lifetime. In England and Wales, the proportion of repeated abortions has increased from 30% in 2000 to 37% in 2012.1
Importantly, as with every medical procedure, there are risks involved with having an abortion. These risks include those occurring during the procedure itself, such as haemorrhage, cervical damage and damage to the uterus, and those following the procedure, such as infection.2 Although the overall risk of adverse outcomes is limited, particularly in countries where safe abortions are readily available, undergoing further abortions exposes women to these risks more than once. Importantly, it should be noted that undergoing an abortion can be safer than continuing an unwanted pregnancy, in terms of the mother's mental and physical well-being. However, it has been reported that multiple surgical abortions may increase the chance of late miscarriage in any future pregnancy,3 although evidence is conflicting.4 ,5 It has also been reported to increase the risk of very preterm birth,6 although other studies7 ,8 contradict this. However, it is reasonable to assume that reducing the rates of women undergoing multiple surgical abortions would be of benefit.
This is especially crucial in countries where the laws governing the provision of abortions are restrictive, causing women to seek unsafe abortions.9 An unsafe abortion is defined as “a procedure for terminating an unintended pregnancy carried out either by persons lacking the necessary skills or in an environment that does not conform to minimal medical standards, or both”.10 The World Health Organization (WHO) estimates that every year 80 million women worldwide unintentionally fall pregnant, and of those, 42 million choose to undergo an abortion. Nearly half of these procedures are unsafe.10 A WHO systematic analysis studying global causes of maternal death found that 7.9% of these deaths were caused by abortion.9 This review studied the effect of contraceptive counselling given around the time of an abortion in preventing subsequent unwanted pregnancies.
NICE (the UK National Institute for Health and Care Excellence) has suggested that increasing the uptake and use of long-acting reversible contraception (LARC), such as intrauterine devices, intrauterine systems and progestogen-only subdermal implants, could lead to a reduction in unplanned pregnancies.11 These are known to be the most effective forms of contraception for women who do not wish to become pregnant in the short term.12 They are prescribed post-abortion as a more reliable and convenient method of contraception than daily oral contraceptive pills and other methods. However, it is important to recognise women's autonomy in their choice of contraception, and acknowledge that some women may prefer non-LARC methods.
Poor contraceptive usage is one of the mechanisms that can lead to unplanned pregnancy,13 with the possibility of repeat abortions. LARC has been shown to improve contraceptive use.14 Equally, if a woman has made an informed decision to use an alternative method of contraception, evidence suggests that this too will reduce the likelihood of poor contraceptive usage. However, one study showed that only 67% of women who understood the contraceptive choices available to them chose to use any form of contraception following an abortion.14 This may contribute to the relatively high proportion of these women undergoing subsequent abortions. One possible solution is enhanced peri-abortion counselling and contraceptive advice. This may benefit women by reducing the likelihood of undergoing subsequent abortions, and when considered against the cost of each abortion, universal implementation of such practices could lead to significant financial savings.
In this review, we summarise the evidence from randomised controlled trials (RCTs) of provision of contraceptive counselling and advice before or after abortion in comparison to women who received standard care. The primary outcome was the subsequent rate of unplanned pregnancies; the secondary outcomes were the uptake of LARC and the continued use of chosen contraceptive methods.
Methods
The PICO (Patient, problem or population; Intervention; Comparison, control or comparator; Outcomes) framework was used to define a focused review question, namely “How effective is enhanced contraceptive counselling in preventing further unplanned pregnancies in women having an abortion?” From this, a combination of MeSH and Boolean operators were used to create the search strategy. Searches were conducted in MEDLINE, EMBASE and the Cochrane Library database from the inception of each database to May 2014. The search was limited to females, humans, papers written in the English language and RCTs. The abstracts and titles of the studies identified by the electronic search were scanned by three independent authors, allowing selection of potentially relevant studies. The bibliographies of these were used to identify any relevant studies that may have been missed in the database search.
This study was concerned with RCTs that provided specialist contraceptive counselling to women before or after an abortion. The outcomes of interest were subsequent unplanned pregnancy, uptake of LARC and continuation of chosen methods of contraception. Studies involving women of reproductive age who had undergone at least one abortion, or were about to have an abortion were included, if the included women received enhanced counselling and information on contraceptive methods before or after abortion. A priori inclusion criteria specified a control group of women receiving standard care or no contraceptive advice following abortion. Studies involving women outside the reproductive age range or women who had never undergone an abortion were excluded. Those studies investigating postpartum interventions or miscarriages without the need for a first-trimester procedure were excluded.
Two authors independently extracted the data from the included studies. The data extraction included population, setting, intervention and outcomes (subsequent pregnancy, LARC uptake and continuation of any chosen method of contraception). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials15 was used to assess the quality of the papers. The criteria assessed whether the following criteria were met in the selected studies: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete data addresses and selective reporting. The studies were given either a high, low or unclear risk of bias for each criterion (see online Supplementary Table 1). However, studies were not excluded based on their risk of bias score. Two authors independently assessed the studies using a priori inclusion and exclusion criteria based on the review question and extracted the study data; any discrepancies were resolved through discussion. The data were analysed in RevMan V.5.1 software [Review Manager (RevMan) (Computer program) V.5.1. Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011], and meta-analyses were performed where appropriate. The pooled effect was estimated using a random effects model and this was presented as an odds ratio (OR) with 95% confidence interval (95% CI).
Results
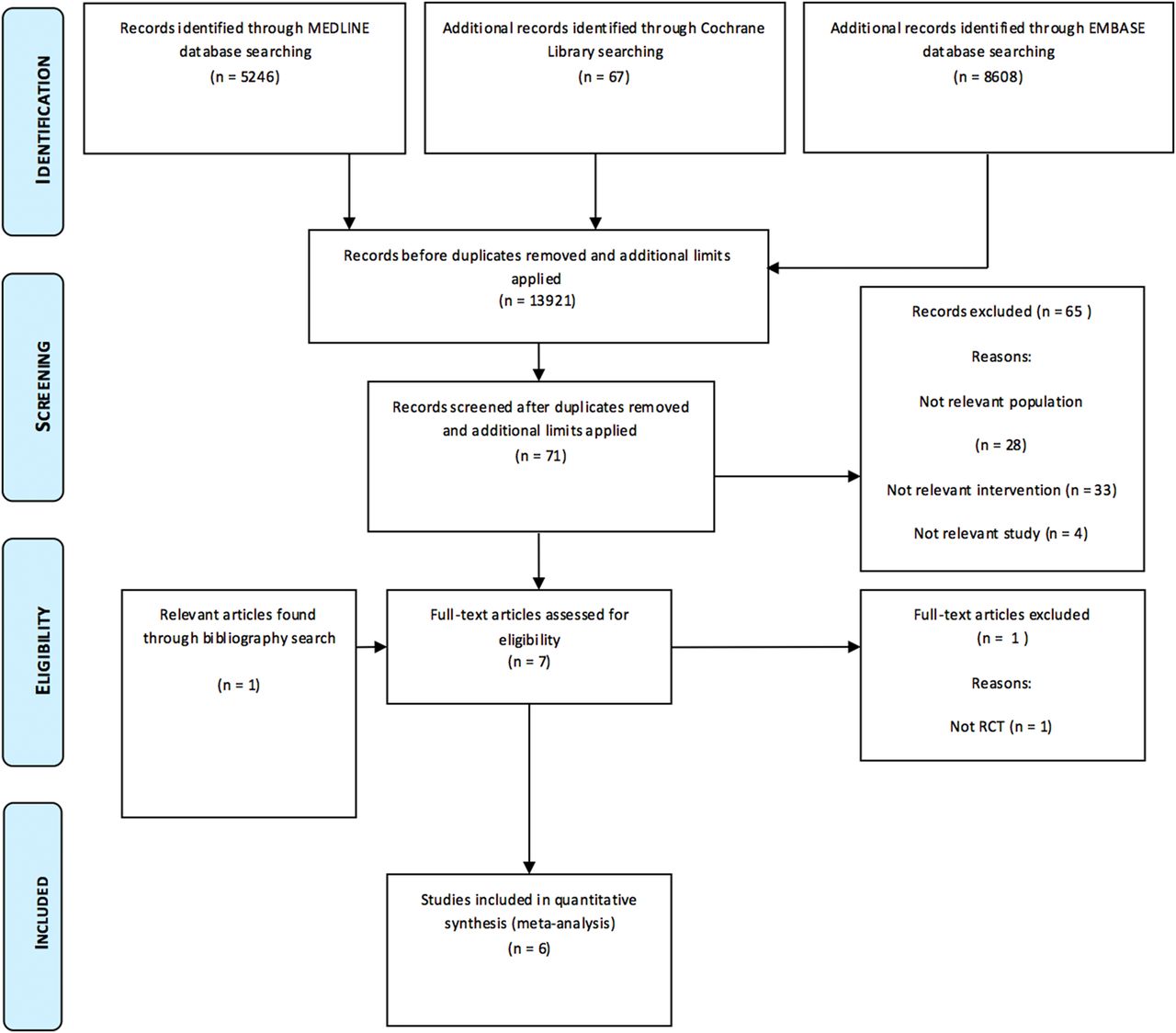
The search strategy identified 13 921 records. A total of 71 abstracts were screened, of which six, including 2502 women, met the inclusion criteria (Figure 1). Five of the studies took place in hospitals,17–21 while one study was conducted in a family planning clinic.22 Four of the studies took place in developed countries: Iceland,20 Italy,17 Scotland19 and the USA.22 The remaining two studies were carried out in newly industrialised countries: China21 and Brazil.18

The PRISMA flow diagram of the study selection process.16
All of the studies included women of reproductive age who had undergone at least one abortion, with two studies reporting that these were first-trimester abortions.20 ,22 Nobili et al.17 and Langston et al.22 both only included participants that were over 18 years of age, whereas Zhu et al.21 reported that all participants were under the age of 25 years. The languages spoken during the data collection varied across the studies; Nobili et al.17 included Italian-speakers only, while Langston et al.22 included participants who were fluent in either Spanish or English.
All the papers reported an intervention involving individual counselling relating to contraceptive methods, although one study also provided group education over a 2-day event involving partners.21 The remaining five studies delivered the counselling in one single session.17–20 ,22 Carneiro Gomes Ferreira et al.,18 Schunmann and Glasier,19 Zhu et al.21 and Langston et al.22 provided the participants’ choice of contraceptive method at no charge, while Bender and Geirsson20 provided participants with a prescription for contraception.
Five of the studies compared their intervention with the standard care available to the participant at the time of the study. The trial by Zhu et al.21 involved two interventions: Package A and Package B. Package A was described as involving only the essentials and its components were broadly similar to those of the standard care controls reported by other studies. However, standard care did vary between studies. A more comprehensive explanation of the standard care available in each study can be found in Table 1.
Characteristics of included studies
Each study reported different outcomes. The majority of the studies investigated the uptake rate of contraception and the rate of continuation of a contraceptive method. These were the studies by Nobili et al.,17 Carneiro Gomes Ferreira et al.,18 Schunmann and Glasier,19 Bender and Geirsson20 and Langston et al.22 Nobili et al.17 also investigated differences in participants’ knowledge about contraception between the two study groups. Finally, Schunmann and Glasier19 and Langston et al.22 investigated the effect of counselling on the rate of subsequent abortions, while Carneiro Gomes Ferreira et al.18 investigated the rate of subsequent pregnancy.
Assessment of bias
Having used the Cochrane Collaboration's tool for assessing risk of bias in RCTs,15 all six studies were deemed to be of a sufficiently high quality to be included in our review (Table 2). However, it was only stated specifically in two studies that participants were blinded.18 ,20 Outcome assessors were blinded in only one study.17 The lack of blinding in these studies is most likely due to the nature of the interventions, as there are inherent difficulties in blinding participants and providers to whether or not they have received or delivered specialised counselling. The risks of selection bias, attrition bias and reporting bias were limited across the studies. Carneiro Gomes Ferreira et al.18 carried out an intention-to-treat analysis in order to reduce attrition bias in their study. When assessing risk of bias, it was noted that some authors described limitations of their studies. One paper stated that they had a significantly small dataset.17 The authors also discuss ‘social desirability’ as a potential cause of bias, as the women in the intervention group may have been tempted to portray a more positive result. Carneiro Gomes Ferreira et al.18 stated that their follow-up time was shorter than ideal; however, some of the other studies also had similar follow-up times. Langston et al.22 mentioned that their participants were predominantly Hispanic, limiting the generalisability of their findings. Bender and Geirsson's20 randomisation procedure resulted in a significantly different intervention group in terms of characteristics such as age, childbearing and previous abortions. Finally, Zhu et al.21 commented that some of the hospitals involved in the trial did not follow the randomisation procedure, but these hospitals were not included in the results.
Assessment of bias
Study results
Subsequent abortion or unintended pregnancy
Two studies found that women in the intervention group were at reduced odds of having a subsequent abortion or unintended pregnancy.18 ,21 Carneiro Gomes Ferreira et al.18 found that the odds were 0.15 (95% CI 0.03–0.70) in the intervention group compared to the control group. Similarly Zhu et al.21 showed the odds of a subsequent abortion in the intervention group in comparison to the control group were 0.32 (95% CI 0.14–0.71). However, one study19 showed that a larger proportion of women in the intervention group went on to have further unplanned pregnancies compared to those in the control group (OR 1.52; 95% CI 0.91–2.54). However, this result was non-significant.
Choice of LARC methods
Two studies found that women in the intervention group were at decreased odds of choosing LARC methods.18 ,20 Bender and Geirsson20 reported that the odds of choosing LARC methods in the intervention group compared to the control were 0.51 (95% CI 0.20–1.26). Similarly, Carneiro Gomes Ferreira et al.18 reported odds of 0.32 (95% CI 0.01–7.93). However, one study19 found that a larger proportion of women in the intervention group chose LARC methods compared to the control group (OR 3.40; 95% CI 2.19–5.28).
Knowledge of contraception
Nobili et al.17 also aimed to increase women's knowledge of contraception. One month after counselling they reported a highly increased knowledge in the intervention group (Z=3.91; p=0.0001), compared to no significant change in the control group (Z=−0.83; p=NS).
Two of the four studies investigating use of contraceptives found that women in the intervention group were significantly more likely to continue their chosen method of contraception for at least 3 months, compared to those in the control group.17 ,18
Continuation of contraceptive methods
Carneiro Gomes Ferreira et al.18 found that odds of continuing to use the chosen method of contraception at 3 months were 26.03 (95% CI 6.11–110.91). Similarly, Nobili et al.17 reported odds of 6.50 (95% CI 1.59–26.51). Langston et al.22 reported odds of 1.24 (95% CI 0.62–2.50); this result favouring the intervention group was non-significant. Schunmann and Glasier19 reported that the odds of continuing the chosen method of contraception were 0.89 (95% CI 0.45–1.74); this result favouring the control group was non-significant.
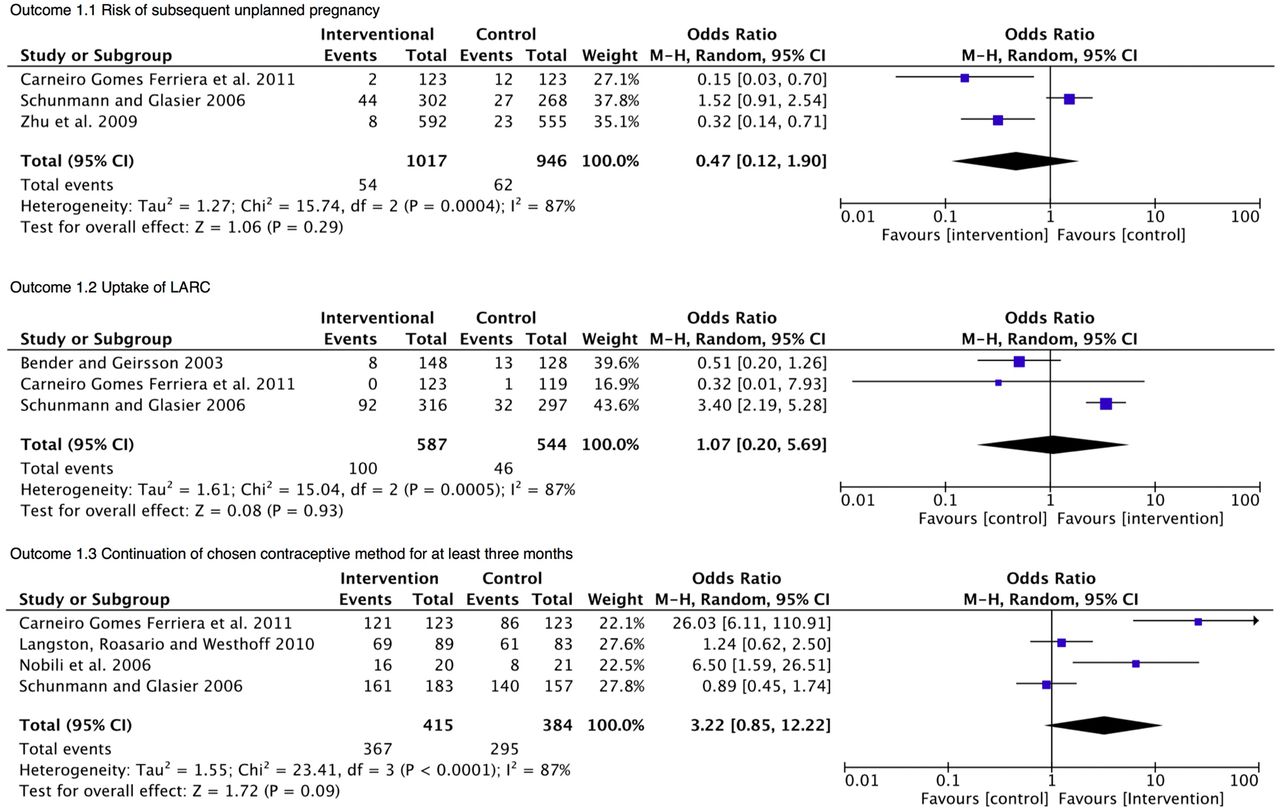
Meta-analysis
Figure 2 shows the meta-analysis for each outcome. No meta-analyses were significant; however, there is some evidence of benefit in Outcome 1.1 and 1.3, while there is no evidence of benefit in Outcome 1.2.
{kind=link}
{kind=link}
Meta-analyses.
Outcome 1.1: Risk of subsequent unplanned pregnancy
There were three studies involving a total of 1963 women, with 1017 in the intervention groups and 946 in the control groups. The results of the meta-analysis showed no significant difference between the control and intervention groups (OR 0.47; 95% CI 0.12–1.90).18–19 ,21
Outcome 1.2: Uptake of LARC
There were three studies with a total sample of 1131 women, including 587 and 544 in the intervention and control groups, respectively. The results of the meta-analysis were not statistically significant (OR 1.07; 95% CI 0.20–5.69).18–20
Outcome 1.3: Continuation of contraceptive method chosen for at least 3 months
There were four studies involving a total of 799 women, with 415 and 384 in the intervention and control groups, respectively. The results of the meta-analysis were non-significant (OR 3.22; 95% CI 0.85–12.22).17–19 ,22
As the statistical heterogeneity was considerable across all included studies (I2=87%; p<0.001), it was deemed appropriate for a random effects model to be used. Using the random effects model provided no statistically significant evidence of effect. For two of the outcomes (Outcome 1.2: Uptake of LARC and Outcome 1.3: Continuation of chosen contraceptive method chosen for at least 3 months), a fixed effect model would have provided a statistically significant result.
Discussion
There are very few RCTs examining the effect of specialist contraceptive counselling for women around the time of abortion. This review takes into account more such trials than any previous review. It also looks at three different outcomes, providing information on the effectiveness of peri-abortion contraceptive counselling on the proportion of subsequent unplanned pregnancies, the uptake of LARC and the continuation of any chosen contraceptive methods. Only three studies were identified that examined the effect of peri-abortion counselling on subsequent abortions or unplanned pregnancy.18–19 ,21 This review demonstrates that there was no significant difference in the number of women who had a subsequent unplanned pregnancy between those who received the specialised counselling and those who received standard care.
Due to the interventions, the women in the trials were more knowledgeable about contraception,17 and this effect was increased further if the male partner was involved,21 but this did not seem to change the outcome of continued contraception use at 3 months post-intervention. There are various factors that can affect a woman's choice of contraception and it is possible that a follow-up time of only 3 months is not long enough to test the impact on the intervention group fully. Carneiro Gomes Ferreira et al.18 had encouraging results of the women being less likely to have a subsequent unintended pregnancy, but a lack of trials and participants included in each group meant that the overall meta-analysis may have lacked the power to detect a significant result; therefore further RCTs are warranted. There was statistical and clinical heterogeneity between the studies, as the studies used different populations and interventions, which may have influenced the outcomes of the study (see Table 1).
Health care systems and policies were likely to vary widely amongst the countries in which the included studies were conducted. Only Carneiro Gomes Ferreira et al.18 and Zhu et al.21 discussed the legal status of abortion and the availability of free contraception in their respective settings. Carneiro Gomes Ferreira et al.18 highlighted that induced abortion is legal in Brazil in only two situations: rape and risk to the mother's life. Furthermore, free contraception is not available and can incur financial hardship. In contrast, Zhu et al.21 discussed China's ‘one-child policy’, which led to the free provision of contraception and induced abortion. These factors may have influenced the results of each study.
Comparison with other reviews
The results from this review corroborate and build upon Carneiro Gomes Ferreira et al.'s23 previous findings. The current review identified more RCTs to test whether specialist contraceptive counselling had an effect on a number of outcomes; however, no significant differences in the proportion of subsequent unplanned pregnancies between the intervention and control groups were found.
When considering the effectiveness of counselling on later use of contraception in women who had undergone an abortion, Carneiro Gomes Ferreira et al.18 also found no significant difference between women in the control group and those in the intervention group. Due to clinical and methodological diversity, and resulting statistical heterogeneity, a random effects model was used when conducting meta-analyses. Despite this, no evidence for effect was found.
However, a high-quality cohort study has shown that women provided with LARC were less likely to undergo a subsequent abortion,24 suggesting that LARC is the most effective post-abortion approach to contraception. Nevertheless, more research should be undertaken to identify how best to encourage continued use of contraceptive methods post-abortion as there are still many women who discontinue their chosen method. Our study shows that specialised counselling before or after the initial abortion does not affect the uptake of LARC or continuation of a chosen contraceptive method. This is either due to the small sample size of the included studies, the short follow-up periods or the fact that the intervention is ineffective. Therefore further high-quality research should be undertaken and other intervention options should be explored.
Strengths and weaknesses
This review builds upon the work of one previous review by including three additional studies and a wider array of results.18 ,21 ,22 The key strengths of this review are robust methodology, exhaustive search strategy and a priori inclusion and exclusion criteria.
However, in our review process, several areas introducing potential bias must be highlighted. For example, due to time constraints, our exhaustive search strategy omitted both studies published in languages other than English and those as yet unpublished.
In addition, the risk of bias in several studies was unclear due to incomplete information regarding randomisation, whilst blinding of participants and personnel was often impractical due to the nature of the intervention. In some cases, the risk of bias was high due to inadequate methods of randomisation and allocation concealment.
Furthermore, clinical heterogeneity was observed between all the studies, with reference to timing of the intervention, duration of the intervention and the specific details of the intervention utilised.
Context of findings
There are several possible reasons as to why this review has found no evidence of effect. The authors of each paper described limitations at the study level, which could have contributed to the overall lack of statistical significance reported in this review. Two trials reported that their results could be vulnerable to the effects of ‘social desirability’,17 ,22 while a third discussed the potential risk of bias introduced through the use of self-reported outcome measures.21
Another issue with the collection of results was noted by Schunmann and Glasier19 with regard to their paper. Information was collected from participants in the intervention group at interview, whereas case notes were reviewed in order to collect data about women in the control group. However, the authors reported that they were unable to review case notes for all participants, therefore control group data were potentially less accurate and complete.19
Several studies discussed issues related to follow-up time.17–19 The feasibility of extended periods of follow-up was limited both by cost and by participant dropout rates, particularly in relation to the outcome of further unwanted pregnancies. Accordingly, follow-up time was described as a limitation by two studies,18 ,19 while another mentioned that the limited follow-up time may have impacted upon the results.17 Furthermore, an individual's intention to avoid pregnancy is not easily measured.18
Some limitations described by individual authors were in reference to the interventions used. For example, the flip-chart aid used for counselling by Langston et al.22 was developed by the WHO to be used for tailored counselling.25 Instead, it was adapted for structured, standardised counselling.22 It is possible that this counselling tool was less effective when used in this way. Zhu et al.21 mentioned that there was some variation in the interventions delivered by their study, as the study was conducted across several different sites in China.
Importantly, participants may have experienced some form of anxiety about the abortion procedure. This anxiety may have resulted in a decrease in concentration, which could limit the effectiveness of the counselling.22 Bender and Geirsson20 highlighted the possibility that participants may experience ‘information overload’. It is likely that these women will have received information regarding the process of an abortion, which may have limited the impact of further counselling.21
Conclusions
The results of this review indicate that there is no evidence for the effect of peri-abortion contraceptive counselling and advice on subsequent unplanned pregnancy rate, uptake of LARC and continued use of chosen contraceptive methods. The included primary studies were limited by small sample sizes and short follow-up periods as well as between-study clinical, methodological and statistical heterogeneity, which may have affected the results of this systematic review and meta-analysis. The results of this review may have been affected by random error due to the small sample sizes of the included studies. This area of research would benefit from larger multicentre clinical trials with longer follow-up periods. Additionally, further research into interventions that encourage the continuation of effective methods of contraception would be of benefit.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue