Article Text

Abstract
Background Engaging community, government and non-governmental organisation (NGO) stakeholders in the design of family planning (FP) programmes is best practice. Stakeholders can provide local insights on barriers to FP. However, it can be difficult to know whether there may be limited programme perceptions if only one method of enquiry is used.
Aim This study aimed to validate the perceptions of stakeholders on barriers to FP in Malawi.
Methods The study was conducted in a rural area in Lilongwe District, Malawi and employed a mixed-methods exploratory design. Five focus groups were run with community, government and NGO stakeholders to identify barriers to using modern FP. The results of the qualitative phase were then compared using a quantitative survey of 960 women who had at least one child aged under 5 years.
Results The qualitative phase identified a range of barriers to FP, including lack of awareness, lack of access, religious beliefs, myths, and opposition by husbands. However, the quantitative survey found that these issues are not a concern for the majority of women. The main reasons given by women for not using FP were that were not currently having sex or had a child recently, and so they felt they did not need to use it.
Conclusions Perceptions of stakeholders from a qualitative approach do not necessarily reflect the perspectives of the population as documented in a quantitative survey. When involving stakeholders it is important to recognise that different approaches may elicit different responses, particularly with regard to sensitive issues or issues that apply to particular subgroups. Consequently, a deeper understanding is likely to be obtained by using a multimethod approach.
- family planning service provision
- ethnic minority and cultural issues
- education and training
- qualitative research
- Malawi
- health knowledge, attitudes, practice
Statistics from Altmetric.com
- family planning service provision
- ethnic minority and cultural issues
- education and training
- qualitative research
- Malawi
- health knowledge, attitudes, practice
Key message points
Community, government and non-governmental organisation stakeholders identified awareness, access, beliefs, myths, and opposition by husbands as the main barriers to modern family planning (FP) in Malawi.
A quantitative survey of women found that the majority were not using modern FP because they were not currently having sex or had a child recently, and felt it was unnecessary.
Perceptions of stakeholders from a qualitative approach do not necessarily reflect the perspectives of the population in a quantitative survey. Stakeholder perceptions identified using quantitative methods need combining with perceptions identified through qualitative methods for more effective programme design.
Introduction
One of the first steps in designing a family planning (FP) programme is usually the involvement of community, government and non-governmental organisation (NGO) stakeholders. Engaging with stakeholders is an important part of any participatory design process.1 This engagement often takes the form of meetings, focus groups or interviews in which stakeholders discuss the barriers to FP in their area. These ideas are then incorporated into the programme design.
FP programmes in Malawi have used similar approaches to engage with stakeholders as part of the design process.2 ,3 Engaging with stakeholders can provide local insights that are critical for appropriate programme design. However, it can be difficult to know whether the qualitatively collected perceptions of stakeholders will be the same as views expressed in quantitative surveys.
This study was conducted during the design of a programme in Malawi. It compares the qualitative perceptions of stakeholders with findings from a quantitative survey to compare the different methods of obtaining stakeholder perceptions.
Methods
The study used a mixed-methods exploratory design. The results of the first qualitative phase were used to design the quantitative instrument for the second phase. The study was conducted in Mitundu Health Area, Lilongwe District, Malawi. Approval for the qualitative and quantitative phases was provided by the Lilongwe District Health Office. As the study was part of ongoing monitoring and evaluation of an existing programme, an ethics review screening process found that it did not require approval from an ethics review board.
Qualitative phase
The qualitative phase consisted of five focus groups with community, government and NGO stakeholders. Three focus groups involved representatives from rural communities, including village chiefs. There were 12 people in each of the three community focus groups. Communities were selected to give a range of distances from the nearest health centre that provided FP services. Individual participants were selected by a community health worker to give an equal number of male and female participants, and a range of ages.
One focus group was for government health workers and included 16 staff from the local health centre, including a nurse, medical assistant, and community health workers. The final focus group was comprised of eight field staff working on a child health programme at an NGO running activities in the area.
During each focus group a problem tree analysis approach was used to elicit discussion about why couples do not use modern FP methods, and the pathways by which these underlying causal factors work.4 Modern FP methods were defined as any method of FP currently offered through government health services, including the pill, female and male sterilisation, intrauterine devices (IUDs), injectables, implants, and male and female condoms. Traditional methods included periodic abstinence, withdrawal or traditional beliefs (e.g. tying a string around the waist and herbal remedies).
The issues raised during each discussion were drawn onto a problem tree. During the final stage the five separate problem trees were synthesised together into a single problem tree. All causal pathways were included, regardless of how many participants mentioned the pathway.
Quantitative phase
The results of the qualitative study were used to develop a survey questionnaire. The purpose of the survey was to verify which of the underlying causes identified by focus group participants were generalisable in the community. The survey instrument was developed and pre-tested by the research team. Some questions were adapted from the 2010 Malawi Demographic Health Survey.5 Analysis was conducted using STATISTICA™ (StatSoft Inc.).
Two-stage cluster sampling was used. In the first stage, 96 villages were randomly selected from a sampling frame provided by the District Health Office. Within each village, 10 households were selected using a random walk quota method. Only households that had a woman with at least one child aged under 5 years old were included. A total of 960 households were surveyed. Within each household one woman of reproductive age was selected to be interviewed.
All participants were required to give informed consent before participating in the survey. This was done with a thumb print on the consent form. The survey was conducted as a structured interview due to low literacy levels among community members.
Results
Qualitative
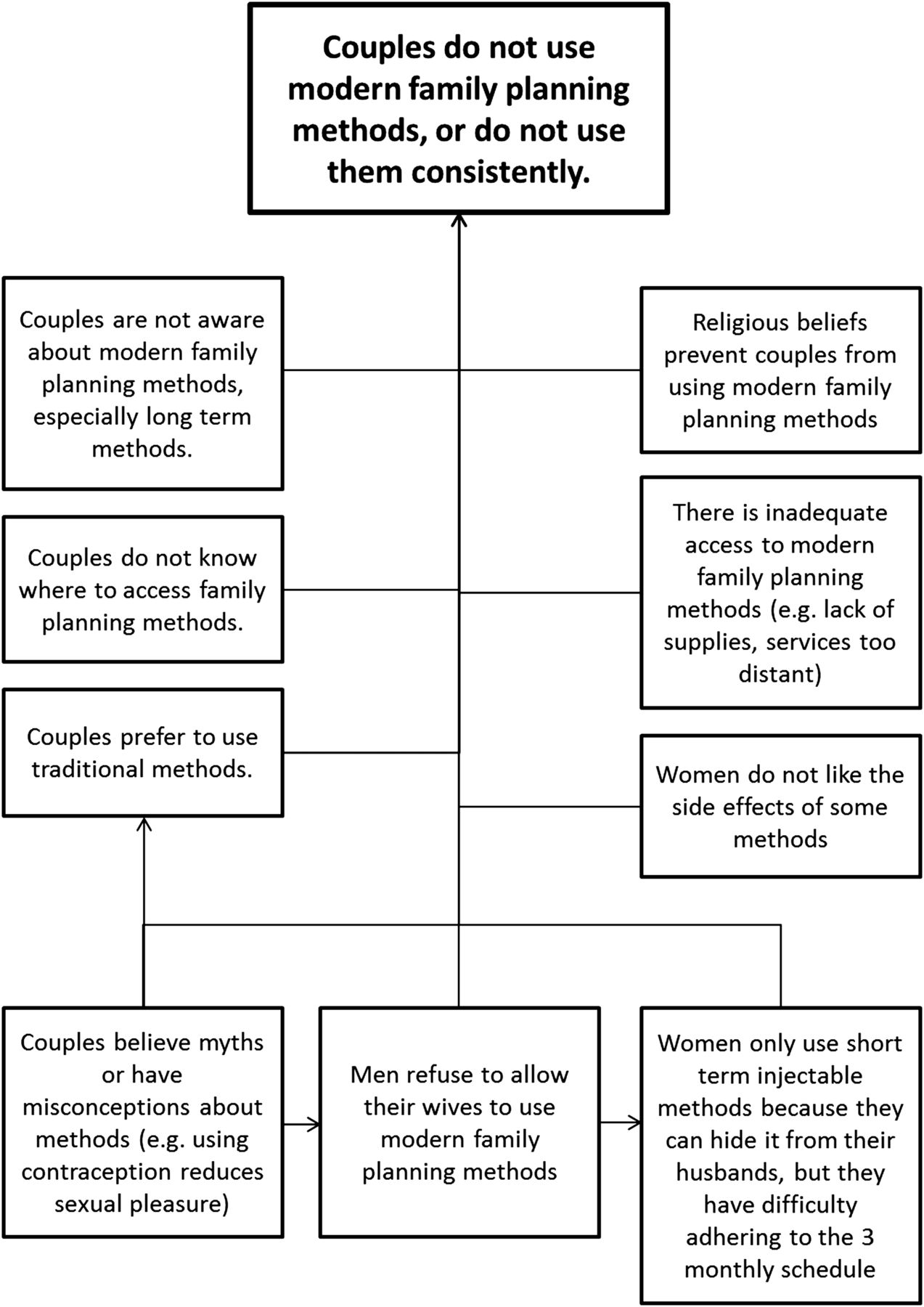
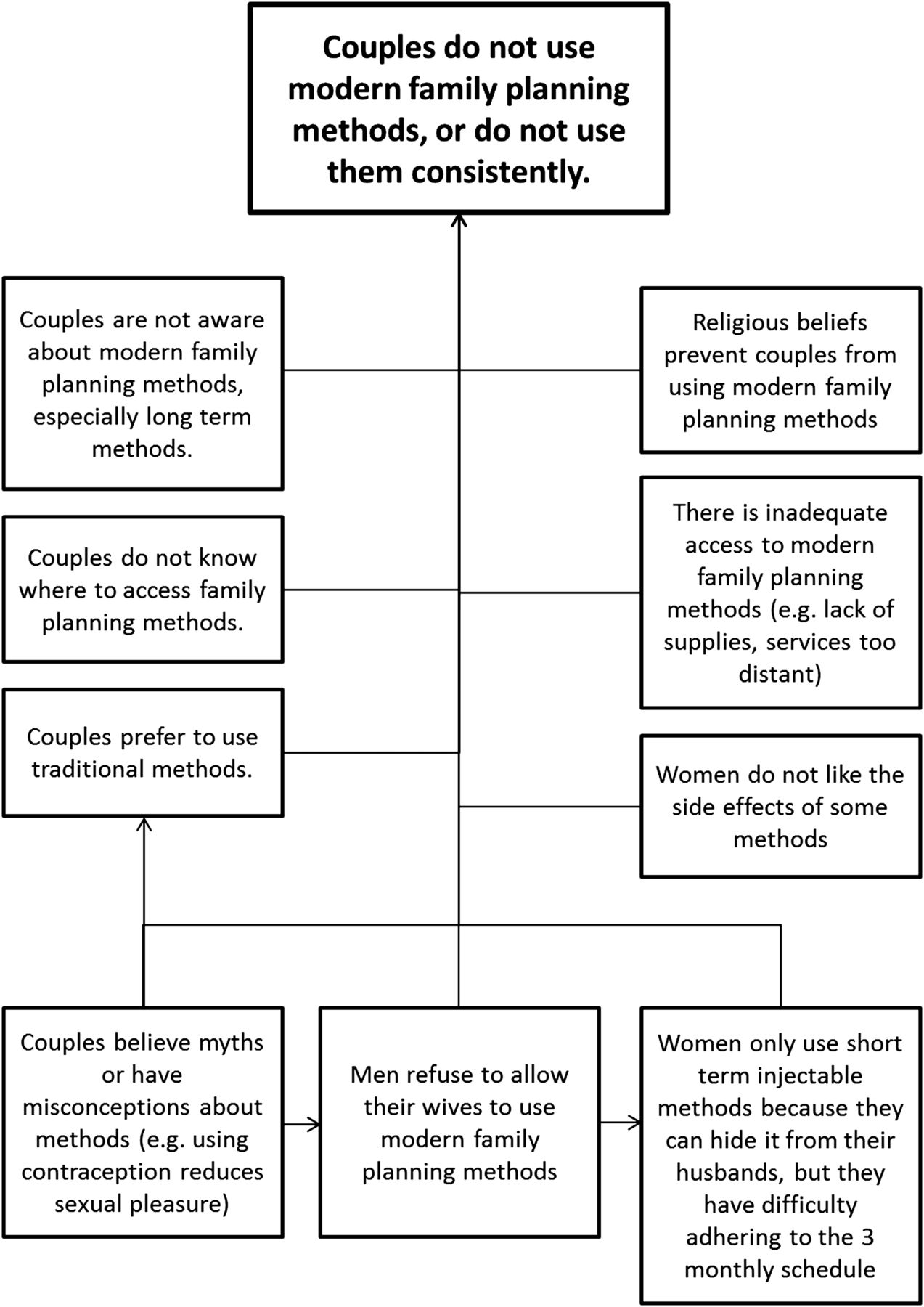
Figure 1 shows the causal pathways that focus group participants identified as leading to couples not using modern FP methods. Many participants thought that couples were not aware about modern methods or do not know where to access them. They also thought that religious beliefs commonly prohibit contraception, that some women do not like the side effects, and that there is a lack of available services.
{kind=link}
Causal pathways leading to non-use of modern family planning methods, as described by community, government and non-governmental organisation focus group participants.
Some participants suggested that couples do not use modern FP methods because they have misconceptions about these methods. Participants mentioned a particular myth that a woman who uses contraception is less sexually attractive to her husband. Focus group participants felt that if a couple believes these types of myths then the husband will not allow the wife to use modern methods, and the couple may prefer to use traditional methods instead.
There is a strong preference in Malawi for the use of injectable methods.5 Focus group participants explained this preference by saying that most women want to use the injectable method because they can hide it from their husband. The preference for injectable methods was seen as contributing to the inconsistent use of FP methods, because it is a short-term method and requires the woman to return to the health centre every 3 months.
Quantitative
Demographics
All 960 women agreed to participate in the survey. The average age of the respondents was 27 (range 17–60) years. Only four participants in the sample claimed to be aged over 50 years with a child under 5 years. They did not have any written record of their birth date, and so may have been younger than 50 years but this could not be verified. Eight (1%) were single, 634 (66%) were married to a monogamous husband, 272 (28%) were married to a polygamous husband, 38 (4%) were divorced and eight (1%) were widowed. Two hundred and ninety-three (31%) women had completed no education, 333 (35%) had attended 1–4 years of school, 282 (29%) had attended 5–8 years of school, and only 52 (5%) had attended 9–12 years of school. The average number of children was 4 (range 1–12) years.
Desire for more children
One hundred and twenty-seven (13%) of the women wanted another child now, 644 (67%) wanted to wait until later, 188 (20%) did not want any more children, and one (0%) woman's data were missing. Among the 381 women not currently using a modern FP method, 112 (29%) wanted another child now, 194 (51%) wanted to wait until later, and 75 (20%) did not want any more children.
Ninety (9%) of the women were pregnant at the time of the survey. Of these pregnancies, 50(56%) were unplanned, namely the woman either did not want the pregnancy at all, or wanted it to be delayed until later.
Use of modern FP methods
Five hundred and seventy-eight (60%) women were using an FP method, 381 (40%) were not using any method, and one (0%) woman's data were missing. Of the women who were currently using a method, 429 (74%) were using injectables, 66 (11%) implants, 42 (7%) female sterilisation, 18 (3%) pill, 8 (1%) IUD, 5 (1%) male condom, 3 (1%) female condom and 7 (1%) other methods.
Of the 578 women using an FP method, 569 (98%) reported that their husband was aware that they were using it. Of the 429 women using injectable contraceptives, 420 (98%) reported that their husband was aware.
Awareness
Table 1 shows that awareness of most modern FP methods (injectables, IUDs, the pill, implants and condoms) was extremely high, even among women who were not using any modern method. Women had higher awareness of modern methods than the rhythm and withdrawal methods.
Awareness of family planning methods among women who use/do not use a modern family planning method
Of the 381 women not currently using a modern method, 365 (96%) knew where they could obtain one.
Reasons for not using FP
Table 2 shows the reasons that the 381 women gave for not using modern FP methods. Excluding the women who want another child or who were pregnant, the majority of women report that they are not using FP because they are not having sex (although almost all of them are married), they had a baby recently, or they are breastfeeding.
Reasons given by women for not using a modern family planning method
Very few women report that they do not use FP methods because their husband is opposed, they have a religious prohibition, they do not know where to access the services, they lack access or they fear the side effects.
Discussion
There is a long tradition of using qualitative studies to identify barriers to FP among different cultural groups.6–10 The qualitative results of this study are consistent with other qualitative studies conducted in Malawi. For example, beliefs about the link between contraception and sexual attractiveness, and the idea that women prefer injectable methods because they are discreet, have both been found in other qualitative studies in Malawi.2 ,3
All the causal pathways identified during the qualitative phase were generally plausible. For example, participants felt that some couples do not use FP methods because their religious beliefs prohibit them from doing so. This is a reasonable idea given that Malawi is a highly religious country, with many Christian denominations having prescriptions on sexual practices.11
Similarly, the idea that men may prohibit women from using modern FP is also plausible given the well-documented power disparity between men and women in Malawi.12 The idea that women may prefer injectable methods of contraception in order to hide their use from their husband also flows logically from this conclusion.
However, the quantitative results provided different causal pathways to the qualitative phase. Few, only 1% of women who do not use modern FP reported that it is because their husband opposes it, and none said it was because of a religious belief. Of the women using injectable methods, nearly all 98% reported that they had told their husband, in contrast to the idea that most women prefer injectable methods in order to hide their use from their husband.
Similar variation between the two methodologies was seen on awareness and access. In the survey almost all the women who were not using a modern FP method were aware of the common methods and where to access them. Very few women reported that they did not use modern methods because they could not access them (either due to monetary, distance or supply constraints). This again was different to the problem trees generated by participants during the qualitative phase.
In the survey the majority of women who were not using FP reported that it was because they were not having sex or because they had recently had a baby and were breastfeeding. This suggests that there may be alternative views among the community that were not raised at all during the qualitative discussion. Specifically, it suggests that women may believe postpartum contraception is unnecessary, particularly if they are still breastfeeding. It also suggests that women who are married but not having sex frequently may feel they do not need to be using contraception. A typical example of this during the survey included women whose husbands travelled for work several months at a time. These women may be having sex every few months, but at the time of the survey were not currently having sex. Further research is needed to confirm this hypothesis.
These results suggest that focus group discussion with community members, health workers and NGO staff may generate different views about why couples do not use modern FP methods compared with a survey. Although these views appear logical and plausible in the focus group, in a survey different views were expressed. A possible reason for the differences between the qualitative and quantitative results could be that qualitative methods, by their very nature, are more likely to uncover motives and reasons, which are difficult to elicit with a closed question. Qualitative methods could also be more likely to provide insights into hard-to-reach groups, which may not be representative of the general population. It is important to acknowledge some of the limitations of this study. First, it was only carried out in one district in Malawi. It is not nationally representative. In addition, the survey sample only included women who had at least one child under the age of 5 years. This would have excluded women who had been using long-term methods of contraception for more than 5 years. The survey included women using and not using modern FP methods, and so the sample size of women not using any method is small. The use of a random walk quota sampling method for choosing households within villages also has limitations. There may be a difference between households who are not at home during the time of the survey compared to those that are at home.
Qualitative approaches have an important role to play in FP research and programme design.13 However, this study suggests that in some settings the qualitative focus group information collected from stakeholders may provide different results to a survey methodology. It is important to gain information using a variety of approaches to obtain a fuller understanding of factors to be taken into account in programme design.
Acknowledgments
The authors wish to acknowledge the assistance of Benson Chidaomba, Burton Saiwala, Christopher Masina, Gertrude Kalirangwe, Ignatius Liphuka, Jenkins Banda, Lesta Phiri and Moses Enoch.
Footnotes
Twitter Follow Piroska Bisits-Bullen at @piroskabb
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue