Article Text

Abstract
Background Increasing access to effective postpartum contraceptive methods can reduce the risk of unintended pregnancy and short inter-birth intervals. The need for an additional postpartum visit can be a barrier to women accessing intrauterine contraception after childbirth. Immediate postpartum intrauterine contraception (PPIUC) provision is known to be safe, but is not routinely available in the UK. Establishing this service requires multidisciplinary support, including from community and maternity stakeholders. The aim of this study was to determine the views of community sexual health providers towards PPIUC implementation.
Methods A questionnaire was distributed to attendees at two UK sexual health conferences. Research questions focused on (1) views on PPIUC (2) perceived role of the sexual health provider in PPIUC service and (3) potential challenges anticipated in providing PPIUC aftercare. Free-text boxes were provided for further comment. Analysis was by a mixed methods approach.
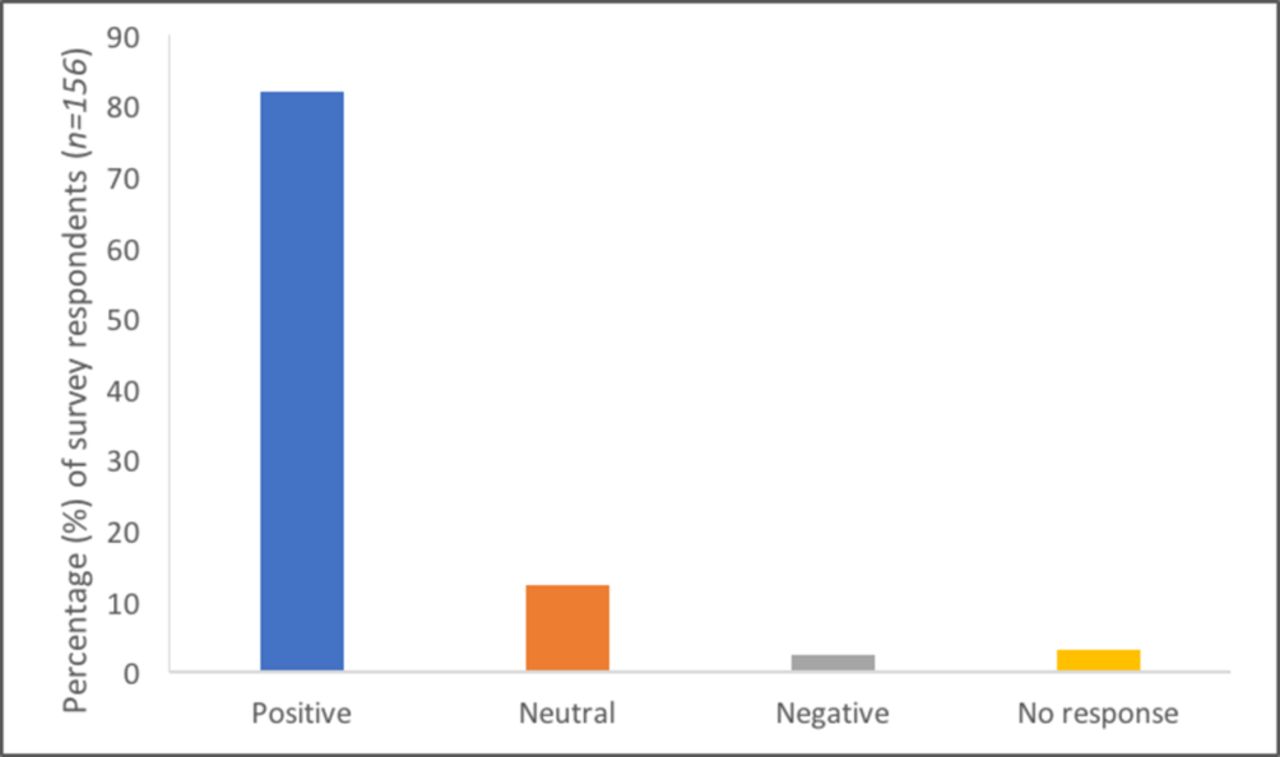
Results A total of 240 questionnaires were distributed with 156 completed (response rate 65%). Some 128 respondents (82%) felt ‘positive’ towards the PPIUC implementation. Most respondents (67.9%) indicated they would be happy to promote PPIUC and provide thread checks. Perceived challenges in providing PPIUC aftercare included staff time, experience in managing clinical issues, and access to ultrasound.
Conclusions Community sexual health providers were positive towards PPIUC implementation, and perceived their role predominantly in the aftercare of women. Several clinical and practical challenges were identified, some of which differ from those previously expressed by other groups. Stakeholder involvement is key to successful implementation of PPIUC, and wider recognition of potential barriers can assist in developing strategies to overcome these.
- intrauterine devices
- long-acting reversible contraception
- postpartum contraception
- family planning service provision
- providers
Statistics from Altmetric.com
- intrauterine devices
- long-acting reversible contraception
- postpartum contraception
- family planning service provision
- providers
Key messages
Multidisciplinary support is essential to achieving successful postpartum intrauterine contraception (PPIUC) implementation in the UK.
Community sexual health providers are positive about the benefits of providing immediate PPIUC.
Challenges exist in the delivery of PPIUC and in the aftercare of women in the community.
Background
There is growing interest in the provision of immediate postpartum intrauterine contraception (PPIUC).1 This service may help reduce the risk of unplanned pregnancy following delivery, and short inter-birth intervals which are associated with increased obstetric and neonatal morbidity.2 3 The clinical safety and feasibility of this technique is well documented, with no observed increase in the risk of complications such as infection or uterine perforation when compared with interval insertion.4 5 Although the risk of expulsion is higher, the long-term continuation rate of PPIUC suggests that this is an excellent option for women.4
At present in the UK women seeking intrauterine contraception (IUC) after childbirth would generally attend either their general practitioner (GP) or local sexual health clinic to arrange insertion in the weeks following delivery. However, the need for a further postpartum visit is recognised as a potential barrier for women.6 7 The movement towards provision of IUC within maternity settings can help overcome these barriers, but may also impact the community contraceptive provider. Following PPIUC insertion, women require a thread check to confirm device location, and referral for ultrasound if IUC threads are not visible. For intra-caesarean insertion, threads may not be visible in 28% to 50% of women.8 9
Currently, PPIUC is not routinely available in the UK. The recent ‘Contraception After Pregnancy’ guideline published by the Faculty of Sexual & Reproductive Healthcare (FSRH) supports the insertion of IUC within the first 48 hours postpartum.10 However, there are limited data around the practical implementation of PPIUC within a public health service. PPIUC is available in many low- and middle-income countries worldwide, and despite the diversity of these settings, common themes emerge as being essential for successful implementation.11 12
Stakeholder involvement and staff engagement are consistently recognised as crucial, along with the identification of clinician ‘champions’.11 13 These are individuals able to actively demonstrate the benefits of providing PPIUC to clinical and managerial colleagues, policymakers and commissioners; and to encourage and support its implementation. This may involve dispelling some of the misconceptions that are known to exist among healthcare providers around the provision of IUC at this time.14 15
Previous studies have focused on the views and practices of maternity providers (obstetricians, midwives) around PPIUC.14 15 However, to our knowledge, there have been no studies focused specifically on community sexual healthcare providers. GPs and sexual health clinicians represent two major stakeholder groups for successful implementation in the UK. They are most likely to be involved in the aftercare of women following PPIUC (eg, thread checks and management of late complications) and it is likely that their opinions and concerns may differ from those involved in the delivery of the hospital-based service component. Having successfully established a PPIUC service within our region (NHS Lothian),8 it is our experience that the responsibilities, referral pathways and funding for PPIUC aftercare can present a significant challenge.
The aim of our study was to determine the views of UK community-based sexual health providers about the implementation of PPIUC, and to identify possible facilitators and barriers to successfully achieving this.
Methods
A paper-based questionnaire for self-completion was distributed to all attendees at two UK sexual health conferences: the FSRH Annual Scientific Meeting (April 2017) and Lothian Sexual Health Update (May 2017). This recruitment method was chosen as it provided a convenience sample of our target population. It was known from previous experience that attendees of both conferences were largely community sexual health providers. Participation in the study was voluntary and anonymous, with general information outlining the background and aims of the study provided in advance.
Research questions focused on three key areas: (1) overall feeling towards implementation of PPIUC in the UK; (2) respondents' perceived role in a future PPIUC service; (3) and potential challenges they anticipated. As a validated tool was not available, questions were designed based on researchers’ clinical expertise in this area, and were pilot tested on the target population. The survey consisted of a combination of fixed-response, rating scale and open-ended questions. Respondents were also invited to add additional comments, either to expand on a previous response or to raise issues that had not otherwise been discussed.
Results from both sites were combined and a mixed methods approach was used for analysis. The fixed responses from the surveys were coded and entered into an Excel database, and descriptive statistics performed. Thematic analysis was used to examine the free-text comments provided in relation to PPIUC and its implementation. Responses were analysed by the second author using an inductive approach and grouped according to themes derived from the data.16 The first author reviewed the coding framework, and contributed to interpretation of the data.
Ethical approval was not required to conduct this study as it was considered as health service evaluation. The NHS Health Research Authority17 provides clear guidance on this and was consulted in advance. Permission was sought from the conference organisers to distribute the survey.
Results
A total of 240 questionnaires were distributed to attendees across both conferences. Of those returned, 156 were completed either fully or in part, representing a response rate of 65%. Data were combined for analysis and the overall demographics of respondents are shown in table 1.
Demographics of survey respondents
Overall feeling towards PPIUC
Respondents were asked to rate their overall feeling towards the implementation of PPIUC in the UK using fixed responses (positive, neutral, negative). Results are summarised in figure 1.
{kind=link}
Respondents’ overall feeling towards postpartum intrauterine contraception implementation in the UK.
Perceived clinical challenges
Respondents were asked to rate perceived importance of certain challenges in PPIUC aftercare service delivery from a pre-defined list (staff time, available equipment/resources, funding and reimbursement, experience of managing clinical issues, access to ultrasound for confirming presence of IUC if threads are not visible). The list was generated based on expert opinion and feedback from stakeholders within an established PPIUC service.8 Survey respondents most frequently indicated that challenges would include staff time, inexperience of managing clinical issues with postpartum insertion (for example, long or non-visible threads), and referral pathways for access to ultrasound in the presence of non-visible threads.
Future role in PPIUC service
Respondents were asked to indicate what their perceived role in a future PPIUC service might be. The possible answers and reported frequencies are shown in table 2. This also includes subgroup analysis for the most highly represented staff groups (ie, GPs and sexual and reproductive healthcare (SRH) clinicians). Of all respondents, 67.9% (n=106) indicated that they would be happy to promote PPIUC and to conduct postpartum thread checks.
Anticipated roles in a future postpartum intrauterine contraception service
Respondents less frequently indicated an intention to train in PPIUC insertion themselves (28.2%), to train other healthcare professionals (32.1%) or to provide a ‘champion’ or specialist role in a future PPIUC service (24.4%).
Free-text responses
There were two areas of the survey where respondents were invited to provide additional free-text responses: in discussing the reasons for their overall feeling towards PPIUC implementation, and to provide any additional general comments. A summary of responses is provided below with further detail available in an online supplementary table 1.
Supplementary file 1
Reasons given for ‘positive’ views
Of the 128 respondents who reported feeling positive towards implementation of PPIUC, 81 supplied additional comments. Three keys issues emerged: PPIUC as improving access to long-acting reversible contraception (LARC) and addressing unmet contraceptive needs; the role of PPIUC in maximising contraceptive options for women; and potential challenges in PPIUC service implementation.
PPIUC was framed as a means to increase access and uptake of LARC. Respondents emphasised key benefits of PPIUC including: effectiveness; reduced risk of unplanned and repeat (‘back-to-back’) pregnancies; high acceptability; and high continuation rates with the method. Respondents noted the potential of PPIUC to reduce the need for multiple appointments. As such, PPIUC was described as an intervention that could ‘save time’ for both patients and services.
PPIUC was framed as an intervention to maximise contraceptive options. Respondents highlighted the importance of increasing contraceptive options for women, providing them with choices around when and where to access services. PPIUC was described as especially important for women who were sure of IUC as their intended contraceptive method.
Reasons given for ‘negative’ or ‘neutral’ views
Of the 23 respondents who reported feeling either negative or neutral towards PPIUC implementation, 16 supplied additional comments. Four key issues emerged: concerns around clinical risks of PPIUC; lack of knowledge and awareness of PPIUC as an option among healthcare professionals; lack of alignment with women’s priorities in the postpartum period; and practical barriers to PPIUC service implementation.
Clinical concerns included the increased risk of IUC expulsion (including unnoticed expulsion), the (false) perception that there may be an increased risk of uterine perforation, and issues around the clinical management of non-visible threads.
Practical barriers to PPIUC service implementation included: maternity staff shortages; lack of trained staff to insert IUC in the maternity setting; time pressures within maternity services resulting in delays to providing PPIUC; concerns around funding for PPIUC provision and subsequent thread check/review services. In addition, poor staff engagement was framed as a potential challenge to service implementation, with the need for local PPIUC ‘champions’ to encourage ‘buy-in’ highlighted. Many of these potential challenges were also echoed by those with an overall ‘positive’ view towards implementation.
Additional issues
Access to education and training in PPIUC emerged as a key issue. Training was perceived as critical to increasing awareness of PPIUC and equipping staff with the necessary skills for insertion at caesarean and vaginal delivery. Nevertheless, concern about shortage of maternity staff and an inability to release available maternity staff for training in PPIUC techniques was seen as a significant challenge. Some respondents suggested that PPIUC training should be integrated into the Royal College of Obstetricians and Gynaecologists (RCOG) curriculum, and/or as part of the FSRH Letter of Competence in Intrauterine Techniques (LoC IUT).18
Discussion
Most community sexual health providers were enthusiastic about the implementation of PPIUC in the UK. There was recognition of the potential benefits of PPIUC in relation to increasing access to effective contraception and in reducing subsequent unintended pregnancy. As expected, community providers viewed their role predominantly in the aftercare of women following PPIUC, with a majority indicating that they would be happy to provide this. Many also indicated that they would be happy to promote PPIUC, highlighting their important role in raising awareness of the service among women during the antenatal period.
However, as well as recognising many of the benefits of a PPIUC service, they also acknowledged several possible barriers and areas of concern. Many of these are consistent with the implementation challenges noted in previous studies.11 In relation to potential clinical issues, respondents felt that access to ultrasound and lack of experience in managing complications after PPIUC were of greatest importance. For PPIUC establishment, multidisciplinary staff training, funding and stakeholder co-operation were highlighted as key areas.
Training
Further education for both maternity and sexual health staff was reported as essential, both in PPIUC insertion techniques and more generally around risks and management of clinical issues. The RCOG have developed PPIUC training materials as part of their work to improve access to postpartum contraception in South Africa and Tanzania, through the Leading Safe Choices Initiative.19 With their permission, we have adapted these locally for training maternity staff in our region. Incorporating information about PPIUC into the national training curricula for midwives and junior obstetricians may assist in achieving widespread adoption and sustainability of this service. For training community-based providers, PPIUC ‘champions’ within sexual health services are likely to play a key role. Widespread staff education for community and hospital-based staff involved in the antenatal and postpartum care of women may assist in dispelling some of misconceptions that currently exist, and would support providers in both the delivery and follow-up care of patients requesting PPIUC. Services that have successfully implemented PPIUC will prove invaluable in disseminating their experience and knowledge.
Funding/commissioning
There is evidence from the USA to support the cost-effectiveness of providing PPIUC20 and its availability aligns with many of the current sexual health strategies in the UK.21–23 Demonstrating local service need and identifying key clinician ‘champions’ to present local data on the benefits of a PPIUC service may assist in prioritising the agenda and securing appropriate funding support. There will be more specific challenges for some regions of the UK in relation to core commissioning groups, particularly as a PPIUC service will naturally cross the hospital and community care boundaries.
Stakeholder involvement
As identified in survey responses, collaborative working between multiple key areas is integral to the establishment of PPIUC. In the UK, stakeholders may include hospital and service managers, maternity staff (midwives, obstetricians), theatre staff, sexual health services, primary care, radiology, pharmacists, IT specialists and patient group representatives. In our experience, a core steering group can help facilitate communication and aid the development of antenatal and postpartum care pathways to manage the patient journey effectively between hospital and community services.
While the demographics of respondents in this survey closely matched those of the conference delegates, it is possible that the views of conference attendees may not reflect those of the wider group of community sexual health providers. It would be beneficial to conduct similar surveys with other key groups to canvas a wider pool of opinion and identify other unique challenges. As part of our ongoing research around PPIUC, we are conducting qualitative interviews and focus groups with maternity providers. This will further assist in identifying facilitators and barriers towards successful implementation.
Although the survey response rate was acceptable, the reasons for non-completion are unknown. Therefore, it is possible that an element of bias exists in the results. However, the mixed methods approach to analysis allowed us to achieve the study aims of identifying perceived advantages and challenges, as both were commented on in the free-text responses. It is also interesting to note that individuals who reported either positive or negative views towards PPIUC provided both positive and negative comments in the free text. Therefore, the feedback may be more balanced than initially expected. It also indicates that while the practical and health benefits of PPIUC are recognised, this does not necessarily translate into widespread adoption as there are many other factors to consider. This may explain in part why countries such as the UK have been slow to establish PPIUC.
In this regard, the development of a shared-learning culture will prove essential to achieving implementation. The experience of healthcare professionals already involved in PPIUC service delivery will be invaluable. There is no doubt that successful PPIUC establishment requires cross-specialty support, particularly from within the maternity sector who will be at the forefront of service delivery . However, it is helpful to assemble the perceptions and opinions of the wider stakeholder group in advance so that potential barriers can be anticipated and addressed. This study represents important stakeholders previously unreported in the literature. In conjunction with data from other studies, we hope to increase knowledge around the practical aspects of PPIUC implementation, and move closer to achieving widespread availability of this service in the UK.
Footnotes
Contributors All authors conceived the idea and contributed to the study design. NB and MC analysed the collected data. MC and NB prepared the initial manuscript. All authors reviewed the final draft.
Funding The implementation of PPIUC in Lothian has been funded by a joint research grant from Wellbeing of Women and the Chief Scientist Office (RG1903).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All of the individual participant data collected during the study is available. Requests can be made via the corresponding author.
Linked Articles
- Highlights from this issue