Article Text

Abstract
Objectives Intrauterine contraception (IUC) is highly effective, safe and long-lasting, but is not a popular method of contraception among British women. This study examined barriers to the uptake of IUC in general practice in England.
Method A sequential mixed-method approach to explore the views of practitioners regarding the provision of IUC. We e-surveyed 208 practitioners from 69 practices in a region of England and subsequently interviewed 14 practitioners from eight practices.
Results Just under half of general practitioners (GPs) (46.8%; 58/124), and only 8.2% (4/49) of nurses reported being trained to fit IUC. Lack of knowledge of IUC was a barrier to fitting, and also to recommending IUC, especially by practitioners who were not trained to fit. There was discordance between reported knowledge of eligibility for IUC and the likelihood of recommending IUC. Respondents were less likely to recommend IUC to young, nulliparous women, women who had experienced a previous ectopic pregnancy, a recent sexually transmitted infection (STI), or an abnormal cervical smear. The qualitative data indicate that risk aversion and limited training, together with practitioners’ assessments that women are uninterested, may lead to IUC being precluded as a suitable method.
Conclusions Increased practitioner education, for those not trained to fit IUC, may remove a barrier to the uptake of IUC in general practice. More research is required on the discordance between the practitioners’ views on the characteristics of women considered suitable for IUC, and the criteria set out in the UK Medical Eligibility Criteria (UKMEC) guidelines.
- intrauterine devices
- intrauterine systems
- general practice
- long-acting reversible contraception
- contraceptive barriers
Statistics from Altmetric.com
- intrauterine devices
- intrauterine systems
- general practice
- long-acting reversible contraception
- contraceptive barriers
Key messages
There is discordance between practitioner knowledge of eligibility for intrauterine contraception (IUC) and the likelihood of recommending IUC to the full range of possible patients.
Practitioners' lack of knowledge about IUC acts as a barrier to recommending IUC in contraceptive consultations.
Increased training in IUC counselling for practitioners who do not fit IUC could address barriers to recommending IUC and referring on to other services.
Introduction
Intrauterine contraception (IUC) is a form of long-acting reversible contraception (LARC) that can provide several years of protection against unintended pregnancy. On a par with sterilisation, this method is over 99% effective in preventing pregnancy, and is suitable for all women, including young and nulliparous women.While IUC is safe, efficient and convenient in the long term, researchers largely concur that long-acting contraceptive methods are not popular1–3 particularly among young women in the developed world, and that many women display a lack of awareness or understanding of IUC.4
In 2005 in the UK, the National Institute for Health and Care Excellence (NICE), the national body which makes recommendations based on effectiveness and cost effectiveness of treatments, recommended increased use of LARC for all women seeking contraceptive advice.5 According to the Medical Eligibility Criteria (MEC) of the WHO, the advantages generally outweigh theoretical or proven risks for women from puberty to age 20 years, both for initiation and continuation of copper and hormonal IUC.1 The recent increase in LARC use is mainly due to an increase in the uptake of contraceptive implants, and not intrauterine contraception.6 IUC remains an unpopular method in England in particular. Our data from the patient survey arm of this research project showed that IUC was used by only 13.1% of women attending the surgeries included in our study and completing the survey, as compared with 21.8% using oral contraception (combined oral contraceptive pill (COCP)/progestogen-only pill (POP)).7 Data available from the NHS England Sexual and Reproductive Health Activity Dataset (SRHAD) for 2016 shows that IUC is used by 14% of women, as compared with 45% using the COCP/POP and 14% condoms.6
Internationally, research suggests that gaps in medical training and healthcare services result in some professionals lacking appropriate knowledge or even harbouring misperceptions of their own.8–10 Of particular note is the reluctance of some healthcare professionals to consider adolescents and nulliparous women as suitable candidates for IUC, reinforcing perceptions that IUC suits a narrower range of women than international and national clinical guidelines advise.11 12 Internationally, cost to the patient can also be an issue, but this is not the case in the UK, where contraception is provided free of charge.
Recent evidence about the attitudes, experience and practice of UK practitioners regarding IUC is limited. It would have been expected that NICE Guidance (2005) and the introduction of a Quality Outcomes Framework (QoF) payment encouraging GPs to advise women on all forms of LARC in 2004 would have changed the situation. However, two subsequent studies found that practitioners were less likely to recommend IUC to younger women,13 14 and a 2014 survey of 150 UK-based GPs and family planning practitioners (as part of a larger study) found that the most frequently reported barriers to the use of IUC were nulliparity, concerns about pelvic inflammatory disease (PID), concerns about difficult insertion, and the belief that women do not like the method.15 This research called for improved training to overcome the persistence of beliefs that are not supported by evidence. The United Kingdom Medical Eligibility Criteria (UKMEC) guidelines for IUC place no restrictions on its use (UKMEC 1) in nulliparous women, women with a history of PID or previous ectopic pregnancy16 and state that the advantages outweigh the risks of its use (UKMEC 2) in teenagers, those at risk of STIs, and with HIV.16
The aim of our research was to understand barriers to uptake of IUC in general practice, and to provide evidence that could help explain the persistence of low uptake. The research was conducted with practitioners and patients. This paper focuses only on the results from the practitioner arm of the study. The results from the patient arm of the study have been published separately.7 17
Methods
The study was registered on the NIHR CRN Portfolio, study ID 15912 ‘Acceptability of intrauterine contraception: a mixed methods study’. Our full methods are reported in detail elsewhere.7 17 The practitioner arm reported in this paper adopted a ’QUANT-qual' approach, in which a quantitative online survey (e-survey) was followed by qualitative interviews in order to generate explanations for findings. Ethical approval was obtained from NRES Committee London South East (14/LO/0004).
Our research was conducted in one region in South East England, and the local Primary Care Research Network (PCRN) supported study recruitment. A total of 69 (12%) practices out of 577 in the region took part in our e-survey (via SurveyMonkey) and from those we received 208 individual responses. The e-survey was followed up by qualitative interviews with seven GPs and seven practice nurses (PNs) from across eight practices. One nurse withdrew informally from the study (by not returning a consent form following a telephone interview). The qualitative data for interviewee PN06 were therefore excluded from analysis. Our quantitative sample was pragmatic and non-random, and as a consequence we have reported only descriptive statistics and cross-tabulations. The non-random sampling method was chosen to allow us to maximise responses to the survey, as it was felt that any attempt to generate a random sample, within the budgeting and time constraints of the project, would result in a very small response rate. Practices were remunerated for the time of staff participating. We present the quantitative findings of a cross-section of practitioners as an indicator of likely barriers. We do not claim that our findings can be generalised with respect to frequency.
The demographic and practice characteristics of those who responded to the e-survey are presented in table 1.
Demographic and practice characteristics of respondents to the practitioner survey
The e-survey questions were developed from existing literature, in particular drawing on a US study,11 and from the clinical experience of one of the authors (SW). The e-survey was refined by the research team and an advisory group, and piloted. The topic guide for the semi-structured qualitative interviews was developed from the preliminary findings from the e-survey.
Descriptive quantitative analysis was carried out using SPSS (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp), and ‘R’ (R: A language and environment for statistical computing, In: R Foundation for Statistical Computing, Vienna, Austria: R Development Core Team; 2015.) The qualitative data were originally analysed independently by two researchers, who checked each other’s selection of themes and employed a descriptive thematic analysis.18 The transcripts were then coded independently by two researchers using the data management software NVivo (QSR International Pty Ltd, Version 10, 2012).
The final analysis was checked against the original transcripts for accuracy and context. The qualitative data allowed us to generate answers to questions that emerged from our quantitative findings.
Results
Quantitative findings
Two strong themes in the quantitative data were around fitting and training, and around knowledge and opinions.
Fitting and training
Of the 208 practitioners who responded to the e-survey, 70 (33.6%) reported being trained to fit IUC. In contrast, 133/208 (63.9%) reported having a post-registration qualification in contraceptive care. Some 13.2% of those trained reported that they did not fit IUC in their present role, and 8.2% of respondents reported that no-one in their practice was trained to fit. In the UK, general practices can receive a locally enhanced service payment (ESP) to fit, monitor, check and remove IUC. There was a statistically significant difference in terms of numbers of practitioners trained to fit IUC between practices receiving ESP and those not, with 57.7% (15/26) of non-ESP practices reporting having no-one trained to fit, compared with 1.3% (2/154) of ESP practices (P<0.001, Fisher’s exact test).
Practitioners were asked about potential barriers to providing or recommending IUC within general practice. They responded by ticking boxes against a list of statements and were also provided with an opportunity to give a free-text ‘Other’ response. Respondents could tick multiple boxes and so findings are reported as numbers of respondents endorsing each potential barrier. Ninety respondents endorsed at least one statement (n=90). Responses were analysed according to whether or not the practitioner reported being trained to insert IUC. Non-trained practitioners endorsed many more proposed barriers than trained practitioners. Unsurprisingly, the most endorsed barrier was lack of training to insert IUC (n=54) or not knowing enough about IUC (n=23). These statements were endorsed only by non-trained practitioners.
Knowledge/opinion gap
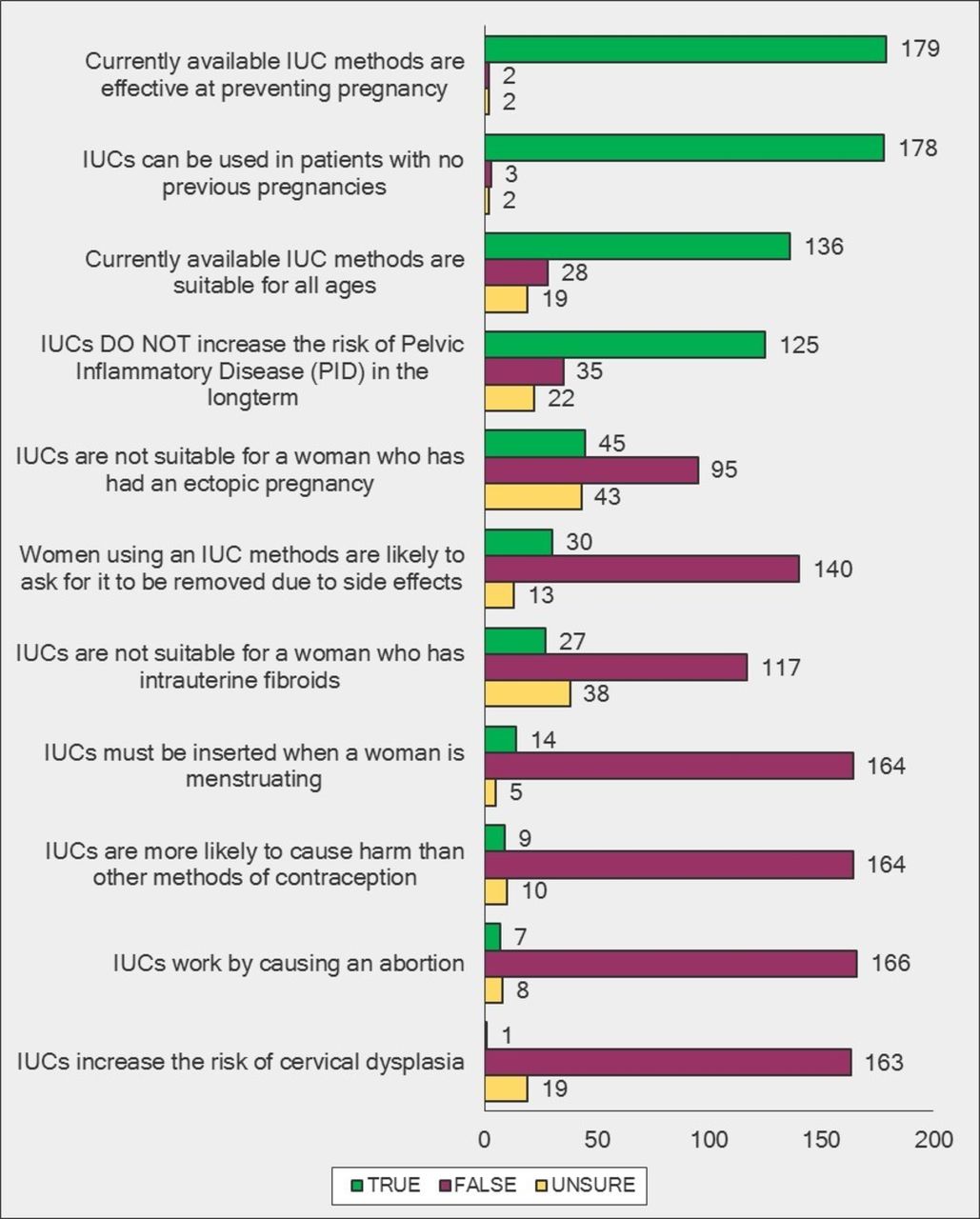
Respondents were asked to state whether they thought a range of statements about IUC were ’True' or ’False' or they were ’Unsure'. Figure 1 lists these in order of those statements most marked as ‘True’.

Practitioners' knowledge regarding intrauterine contraception (IUC).
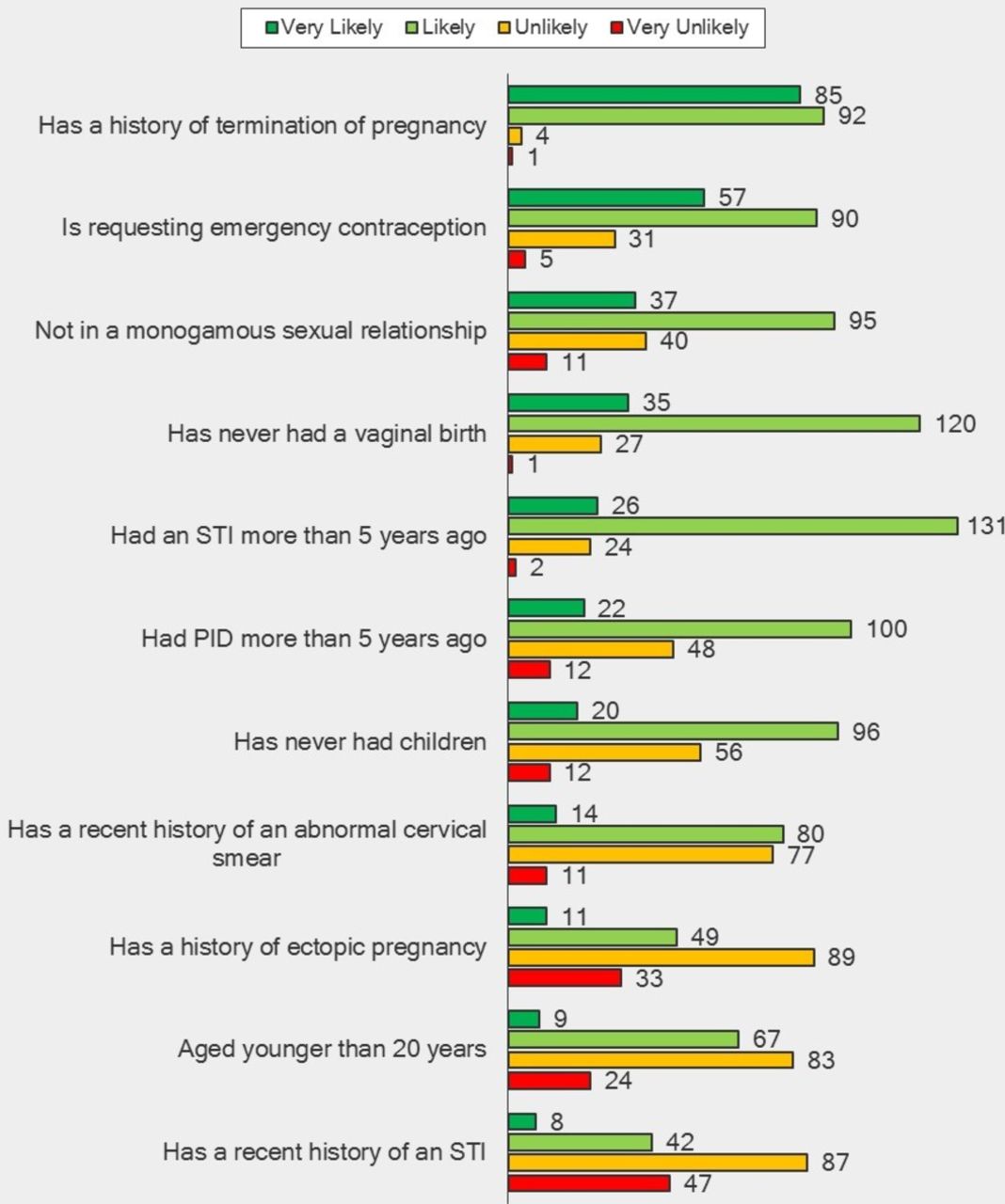
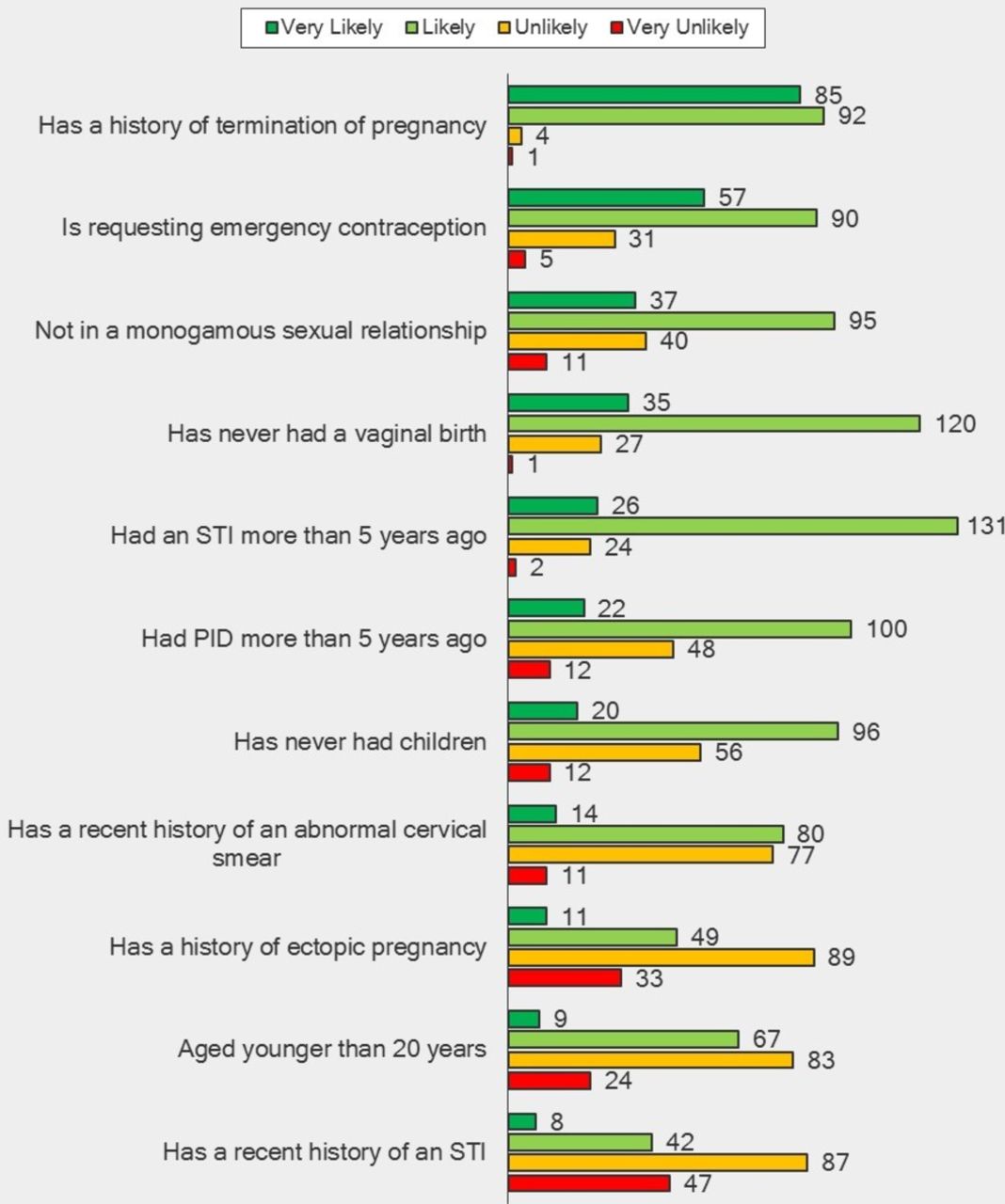
Respondents were also asked how likely they were to recommend IUC to women with a range of characteristics. Figure 2 is ordered from most to least likely to recommend.
{kind=link}
{kind=link}
Likelihood of practitioners recommending intrauterine contraception. PID, pelvic inflammatory disease; STI, sexually transmitted infection.
Opinions
We noticed a difference between responses with respect to knowledge regarding eligibility and likelihood of recommending IUC. This may indicate a gap between cognitive knowledge and actual practice. For example, 178 (97%) respondents answered ‘true’ to the statement ‘IUCs can be used in patients with no previous pregnancies’, whereas only 116 (63%) would recommend IUC to women who had never had children; and 136 (74%) answered ‘true’ to the statement ‘currently available IUC methods are suitable for all ages’, but only 76 (42%) were likely or very likely to recommend IUC to women aged under 20 years.
Two main issues identified and selected for exploration in the qualitative interviews were therefore: (1) the dissonance between knowledge about suitability of IUC and the categories of women to whom the practitioners would be likely to recommend IUC (a gap which has been recognised in other fields such as diabetes care and osteoporosis treatment)19 and (2) training barriers and why a lack of training to fit IUC might affect confidence in recommending IUC.
Qualitative findings
Our thematic analysis on practitioner-based barriers to IUC identified four strong themes:
proactive selection of women for whom IUC is considered suitable
risk aversion
perceived and received knowledge of ‘what women want’
competencies, training deficits and confidence.
Proactive selection
Most of the practitioners, both GPs and practice nurses, felt that IUC was suitable for more women than were currently using it, and that it could be used more by young women. Some practitioners, however, said they were less likely to recommend IUC to young or nulliparous women, and these data are therefore important. One respondent indicated proactive selection of women:
After the first child I try to steer them towards the coil insertion and I prefer not to do it in the nulliparous unless they specifically request. [GP05, trained]
Others mentioned the very limited circumstances in which they might recommend IUC. One respondent described how other methods had to fail before IUC was considered:
for the youngsters… if they’re not good [at taking the pill] then the implant I think is what we tend to try and go for next, then Depo and then say the coil for when all else fails. [GP03, trained]
The view that IUC was an ideal form of contraception to target at women who had required emergency hormonal contraception was also expressed:
If they’d had one lot of emergency contraception, that was fine. If they came a second time then they got sent to me and we’d try and talk them round and have coils fitted. [PN04, trained]
Risk aversion
If respondents expressed a reluctance to recommend IUC to some groups of women, the reasons they gave were primarily based on technical difficulties and the perceived heightened risks associated with the procedure for nulliparous women:
The ladies that haven’t had children the cervix tends to be closed making it technically a bit more difficult to physically get the coil in […] also ladies that have had children and are more familiar with gynaecological examination tend to tolerate the procedure better. [GP03, trained]
One respondent noted that "the cervix is so sensitive in the nulliparous, that’s my only concern" [GP05, trained], and worried about cervical shock in those circumstances.
Selection against younger women was also explained by a perception of heightened age-based risks:
The infection risk with the chlamydia and things like that is […] much higher in those under 25. And I think that age group as well […] we want to be certain ladies aren’t pregnant when we put coils in, they have to abstain from intercourse and have alternative contraception beforehand, I find that group tend to be more difficult when it comes to that. [GP03, trained]
The perception of IUC insertion as a risky procedure was a strong theme:
You always run a risk with any gynaecological procedure of increased sort of complaints…you can perforate uteruses, cause really nasty infections, drop blood pressures…it’s not without risk. [GP03, trained]
This was a risk that was highlighted by practice nurses who explained that perforation was a major risk that distinguished IUC fitting from implant insertion:
Part of me is still slightly nervous, you think ‘ooh what if I do, what if I perforate or do something wrong’. [PN07, not trained]
Perceptions of risk also informed ideas about the different roles of doctors and nurses. The risk of litigation was seen as a burden which doctors, rather than nurses, are more likely to accept in their everyday practice.
The practice nurses don’t want to do it because it’s quite…an invasive procedure and a lot of nurses are a bit scared about litigation. [PN04, trained]
What women want
Practitioners explained their own hesitation at recommending IUC more generally by referring to what women want. Most practitioners stressed that contraceptive consultations were patient-led and there was a perception that the most difficult barriers to address lay with the women themselves who know which method they would like:
I don’t think we do so much contraceptive choice consultations in general practice, a lot of younger ladies will come and say, ‘I want the Pill, I want the injection, I want an implant’; they’ve often made their mind up before they come. [GP04, trained]
Additionally, practitioners felt that women themselves were averse to IUC:
I definitely feel that a lot of women, when you just say ‘coil’ recoil. [GP07, trained]
Practitioners were asked why they thought women might be averse to IUC. Their explanations centred on the role of women’s informal information sources on their contraceptive choice:
Often women will pay more attention to each other and the media than they will health professionals. [PN02, trained]
Other practitioners thought that discomfort around fitting could cause general negativity, and that hearing about other women’s bad experiences led to reluctance to try the method:
I think there’s a lot of bad experiences out there, and those that haven’t had children they hear horror stories about the fitting of the coil so therefore choose not to have it. [PN03, not trained]
Training
The qualitative interviews provided some plausible explanations for the training-based barriers. A shortage of trainers was identified as an issue:
There aren’t that many people that train and so I was probably waiting for at least a year. [GP07, trained]
Funding for training was also cited as a barrier:
I think part of it is funding, part of it is the availability of training and mentorship. [PN05, not trained]
However, practitioners also thought that lack of demand was a limitation on training:
If for example there were lots of patients within a practice who it was obvious they needed coils fitting, lots of people were trying to book appointments and they were getting frustrated they couldn’t get any, then it would generate a need and perhaps that would be a way to try and get nurses to do it. [PN02, trained]
These limitations fed into issues around revalidation and who should have precedence with respect to fitting sufficient numbers of IUC to retain competency. Maintaining competency was also seen as a potential problem in practices where there is a lower demand and/or more practitioners are trained:
You need to be fitting a certain number of coils per year or per month and that the general feeling is that you won’t be able to see that many, if many of us are doing the fitting. [GP06, not trained]
There was an awareness that practice nurses are not often trained in IUC fitting (although they assist with fittings, and some are trained in other LARC methods), and it was acknowledged by both GPs and nurses that additional nurse training in IUC may help strengthen their contraceptive service. However, a number of barriers were identified. It was noted that nurses have a lot of clinical skills to maintain, and training in IUC could mean losing a different skill, or being too stretched to continue to deliver all of their other services effectively:
We have lots of different roles, lots of different hats, so we’d have to be taken away from something else to actually do that. [PN05, not trained]
Other barriers included ideas about job roles and who should fit IUC:
Not all family planning GPs wanted to actually train any nurses to do it because the way they see it, is that we’re taking their jobs. [PN04, trained]
As discussed earlier, there was also evidence of risk aversion, and this affected practice nurses’ willingness to consider training.
Discussion
The strength of this study lies in the use of qualitative interviews to amplify the findings of the quantitative e-survey. New insights obtained from the qualitative data add to understandings of barriers, and suggest how they might be ameliorated in a general practice setting.
We acknowledge that there are some limitations to our study. We used a non-random sample of practitioners for the e-survey resulting in the possibility of bias in the findings, since the attitudes, knowledge and experiences of non-responders cannot be ascertained and may have differed from those who did respond. Additionally, with both samples it is important to bear in mind that these practitioners opted-in to the study and thus may be more likely to be supportive of IUC than a representative sample. As such, we are likely to be understating the barriers we have identified.
Changes in the past 5 years in the way contraceptive and sexual healthcare services are commissioned and funded in the UK have led to increased complexity and fragmentation of the services. GP practices may undertake insertion of IUC as part of a locally enhanced services (LES) contract (or similar local arrangement), which varies from region to region, and is commissioned by the Local Authority20 These usually take the form of a fixed payment per device inserted, monitored and removed. Training of nurses or doctors is not generally included in such arrangements, and the costs in terms of time, and any fee for training, are borne by the practice (as employer) or the individual practitioner. Insurance for medico-legal claims for nurses employed by a general practice is funded by the nurses themselves or by the employing practice. Undertaking more advanced procedures such as insertion and monitoring of IUC may lead to increased indemnity fees, which are another expense associated with providing IUC services at a practice level. This reimbursement structure helps account for the difficulties expressed by practitioners with regard to training staff, and funding training and staff time to provide an IUC service. Our study did indicate that enhanced service payments for fitting and removing IUC appear to have a beneficial effect on numbers trained to supply IUC within a practice. Commissioning should ensure that all women have access to local practices where IUC is provided, and include recompensing practices for all the time and cost involved in supplying IUC.
In our quantitative sample only a very small number of practice nurses were trained to fit IUC, or even had a specialist qualification in contraception. Given the expanded role of practice nurses in the provision of contraception, it is especially concerning not only that few nurses were trained, but that significant barriers to such training were identified in the qualitative interviews. We also found that lack of knowledge about IUC acts as a barrier to initiating discussion about IUC, let alone recommending it. This suggests that increased training in IUC counselling for practitioners who do not fit IUC could address barriers either to recommending IUC or to referring on to other services if necessary. A requirement for a basic level of training on IUC as a method of contraception for all practice nurses who provide contraceptive advice might help ensure that contraceptive counselling includes knowledgeable discussion on all methods, which is particularly important when women express a preference for LARC methods.
There is a gap between practitioner assessments of which women are suitable for IUC and those who are eligible for the method according to UKMEC guidelines. While this is not a new finding, it is a persistent one. The difference between responses with respect to eligibility and suitability is of interest and indicates a gap between cognitive knowledge and actual practice. The qualitative research helps clarify why practitioners may make non-evidence-based judgments about the characteristics of women for whom IUC is suitable. The effect of this is likely to be unnecessary restriction in recommending IUC for women for whom it is a valid and safe contraceptive option. Our study of the views of never-users of IUC, reported in another article that appears in this journal , suggests a double barrier effect: IUC is not offered to women because they do not request it, but women do not have good knowledge of IUC, and opportunities to discuss the method are being missed.17 This impasse is reinforced by the barriers identified around training, which is not seen as a priority when low demand does not justify its time and expense.
Measures need to be taken to dissipate both practitioner assumptions about women’s suitability and demand for the method, and women’s misperceptions about IUC, to ensure that as far as possible all women are able to make informed choices based on the full range of contraceptive methods that may be suitable for them. Our study indicates that in order to overcome practitioner assumptions, women may need to be proactive and request IUC. Women who visit their GPs without adequate information, or even with disinformation, would benefit from clear information to assist in their decision-making. Research has shown that additional practitioner training may help: a 2013 survey of 106 US medical students found that poor knowledge of IUC was improved by an obstetrics and gynaecology attachment.9 Research has also suggested the need for specific targeted strategies to encourage implementation of research-based recommendations to ensure change in practice, since passive dissemination of information is generally ineffective.21 22 As a result of this study, we have developed an ‘aide memoire’ that could be used by all practitioners who provide contraceptive consultations in general practice, not just those who have specialist training (see online supplementary materials). This would help address the knowledge-practice gap around IUC provision that has been highlighted by this study.
Supplemental material
Acknowledgments
The authors would like to acknowledge the research assistance of Elektra Lapavitsas and Catherine Bannister and the invaluable input of the research advisory group.
References
Footnotes
Funding This study was funded by Bayer PLC, manufacturers of several types of intrauterine devices and systems. The funder played no part in the design or implementation of the research, other than requesting that the authors explored, in the qualitative interviews, the participants’ opinion of a new product, Jaydess. The funder has had no influence over the article as written and submitted for publication.
Competing interests None declared.
Patient consent Not required.
Ethics approval NRES Committee London South East (14/LO/0004).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue
- Research