Article Text

Abstract
Background and methodology Treatment of individuals with chlamydial infection and their sexual partners is an important aspect of reproductive health care. Partners of infected individuals are currently offered ‘epidemiological treatment’, which means that they are offered antibiotic treatment at their first visit without waiting for the result of their chlamydia test. We carried out a study to identify the risk factors for chlamydial infection in partners of infected individuals. Individuals attending a genitourinary clinic as chlamydia contacts were identified and asked to complete a questionnaire about their relationship with the index case and their prior sexual history. The result of their chlamydia test was then analysed against those variables.
Results A total of 115 chlamydia contacts were analysed in this study; 60 (52%) were found to be positive for chlamydial infection. In a multivariate analysis, young age, more than one episode of sexual intercourse with the infected partner and a greater total number of sexual partners were associated with a positive chlamydia result. A prediction model for chlamydial infection using these risk factors had a discriminatory ability quantified by an area under the curve (AUC) of 0.76 (95% CI 0.66–0.85).
Discussion and conclusions The risk factors identified can be used when discussing epidemiological treatment with individuals who attend sexual health services as chlamydia contacts, or to target clinic resources to a higher-risk group. Larger studies will be necessary to assess the benefits and risks of changing to a policy of offering epidemiologic treatment to ‘high-risk’ contacts only, identified using a predictive model such as the one described here.
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis is the most common treatable bacterial sexually transmitted infection (STI) in the UK. A total of 200 959 new cases of chlamydia were diagnosed in 2008, mainly from individuals aged between 15 and 24 years.1 Within this age group, 9.7% of screens done on women and 8.7% of screens done on men through the National Chlamydia Screening Programme (NCSP) are positive for chlamydia.2 If left untreated, chlamydia can cause urethritis, epididymitis, cervicitis, pelvic inflammatory disease, ophthalmic and neonatal complications. The high prevalence of chlamydia, together with its potential to cause serious complications, makes management of chlamydial infection an important aspect of reproductive health care.
Key message points
▶ The infection rate for chlamydia among partners of index cases was 52%.
▶ Factors associated with a positive chlamydia test in chlamydia contacts were young age, more than one episode of sexual intercourse with the infected partner and a greater total number of sexual partners.
▶ Larger studies are necessary to assess the benefits and risks of changing to a policy of offering epidemiologic treatment to ‘high-risk’ contacts only, identified using a predictive model such as the one described here.
In addition to treating the index case, the UK national guideline for the management of genital tract infection with C. trachomatis recommends ‘epidemiological treatment’ of all sexual partners of infected individuals. This means offering antibiotic treatment to all chlamydia contacts during their first visit, provided that their last exposure to chlamydia was within 6 months of diagnosis if the index case was asymptomatic or within 4 weeks if the index case was symptomatic.3 Not all these chlamydia contacts will test positive for chlamydia. Results from previous studies looking at concordant infection rates for chlamydia between sexual partners have been variable, ranging from 24% to 76%.4 5
The NCSP protocol also recommends epidemiological treatment of sexual contacts of infected individuals.6 In Leicestershire, UK the NCSP target for 2011 is to test 51 000 young people each year.7 This means that up to 5000 new cases of chlamydia could be diagnosed each year (based upon the NCSP positivity rate of 8.7–9.7%). If one chlamydia contact is seen for every case found, a large number of individuals could be prescribed antibiotics unnecessarily each year. This represents a considerable waste of resources and a risk of producing resistance among other, non-chlamydial, organisms.
The aim of this study was to establish the concordant infection rate for chlamydia between sexual partners, defined as the percentage of chlamydia diagnoses among partners of index chlamydia cases, and to identify the risk factors for chlamydial infection in chlamydia contacts. Although the epidemiology of C. trachomatis has been extensively investigated, there is very limited contemporary literature with reference to chlamydia contacts.
Methods
This was a questionnaire-based cross-sectional study. Participants were recruited from the clinic population attending the genitourinary department at the Leicester Royal Infirmary, Leicester, UK for a period of 6 months starting on 1 August 2007. Individuals were recruited if their presenting complaint was sexual contact with an individual diagnosed with chlamydia during the last 6 months. Individuals were excluded if they declined to undergo a chlamydia test at the time of review, if the positive chlamydia status of the index case could not be confirmed or if they were younger than 16 years. The positive chlamydia status of the index case was confirmed by accessing their test results, or if the presumed contact presented with a contact slip for chlamydia from another clinic. Testing for chlamydia was done using the BD ProbeTec™ ET amplified DNA assay (Becton, Dickinson UK Ltd, Oxford, UK). A first-pass urine specimen in men and an endocervical swab in women were submitted for analysis. The BD ProbeTec ET amplified DNA assay has a sensitivity of 94.5% and specificity of 91.4% for chlamydia from a first-pass urine specimen in men and a sensitivity of 92.8% and specificity of 98.1% from an endocervical swab.8
Patient recruitment was undertaken by the health advisers who are routinely referred such patients after they are assessed, examined and tested for chlamydia and other STIs by the medical practitioner. All patients who agreed to participate in this study provided written informed consent, and were then allowed a few minutes to complete a questionnaire. During this time a health advisor was available to answer any questions and provide quality assurance checking for accuracy and completeness. For each patient recruited, the chlamydia test result was traced and recorded.
The questionnaire was developed based on prior research on risk factors for chlamydial infection and other STIs. Sociodemographic factors examined were age, sex, ethnicity and sexual orientation. The time period elapsed since the patient last had sex with the infected partner was recorded.
Sexual behaviours assessed included the number of episodes of sexual intercourse with the infected partner (defined as oral, vaginal or anal sex), the total number of sexual partners, the age at first intercourse and use of contraception. Other variables assessed were past history of chlamydia or other STIs, presence of genital symptoms, use of antibiotics within the last 3 months and history of serious illness.
History of serious illness was defined as any illness requiring hospitalisation or extended periods off work. Symptoms included abnormal urethral or vaginal discharge, dysuria, postcoital bleeding or dyspareunia. Whenever patients were unable to give an exact figure (e.g. for total number of sexual partners) they were instructed to give the closest approximation. The method of contraception used was indicated by encircling the appropriate method or methods from the different contraceptive options. Condom use was divided into ‘always’ (i.e. consistent use) or ‘sometimes’.
Statistical analysis
Statistical analysis was done using SPSS Version 15.0 (SPSS Inc., Chicago, IL, USA). Frequency tables were generated for all the variables. Univariate associations of questionnaire variables with diagnosis of chlamydia were assessed by means of Chi-square (χ2) (categorical variables) and Mann–Whitney tests (quantity variables). Univariate predictors significant at a level of less than 0.2 for chlamydial infection were selected for logistic regression analysis. Potential confounders which showed no univariate association but which were significant in other studies (i.e. barrier contraception, total number of sexual partners and presence of symptoms) were also included. The variables not selected for multivariate analysis were gender, ethnicity, sexual orientation, previous antibiotic use and a history of other STIs or serious illness.
Backward stepwise regression was performed using the Wald test to select variables for removal. The calibration of the model was evaluated using the Hosmer and Lemenshow goodness-of-fit test. The sensitivity and specificity of this multivariate model was assessed using a receiver operated characteristic (ROC) curve. The ROC curve is a plot of the true-positive rate against the false-positive rate (1–specificity) for the different possible cut points of a diagnostic test, with the area under the curve (AUC) giving an indication of the ability of the multivariate model to discriminate between individuals with or without chlamydia. An AUC of 1 indicates a perfect predictive model.
Results
A total of 123 chlamydia contacts were recruited into this study. This included one patient with an indeterminate chlamydia result, three patients who were not tested for chlamydia and four patients who were recruited despite having been exposed to chlamydia more than 6 months previously. A total of 115 cases were therefore suitable for analysis.
The age range was 16–64 years with a mean age of 25 years for men and 21 years for women. 48% of individuals were aged between 19 and 24 years. 83% of individuals presented to clinic within 6 weeks of last exposure to chlamydia. 81% of individuals attended within 1 week of having been told that they could have chlamydia. Twenty-eight (25%) patients had a previous history of chlamydia. Five individuals who reported STIs other than chlamydia in the past had gonorrhoea, warts, scabies, genital herpes and non-specific urethritis, respectively. Although most individuals recruited were White Caucasian (86%), there were four Black Africans, three Asians, four individuals of mixed ethnicity and three individuals from the Caribbean in the cohort. Five (5%) individuals were men who have sex with men (MSM). Sample descriptive, together with the results of a univariate analysis of the chlamydia risk determinants, are presented in Tables 1 and 2. There were insufficient numbers to analyse the individual ethnic groups or the individual methods of contraception apart from condom use.
Description of the study sample in terms of categorical data, and assessments of association of chlamydia diagnosis with the other variables presented
Description of the study sample in terms of age and other quantity variables, and assessments of association with chlamydia diagnosis
Of the 115 individuals who were exposed to chlamydia within the last 6 months, 60 (52%) tested positive for chlamydia. Univariate analysis of the data established that young age, more recent exposure, more than one episode of sexual intercourse with the infected partner and no previous history of chlamydia were statistically significant risk factors for infection with chlamydia. In a multivariate analysis (Table 3), factors associated with a positive chlamydia test in chlamydia contacts were young age, more than one episode of sexual intercourse with an infected partner and a greater total number of sexual partners. A prediction model for chlamydial infection using these risk factors had a discriminatory ability quantified by an AUC of 0.76 (95% CI 0.66–0.85). Increased time since last exposure to chlamydia was associated with a decreased risk of testing positive for chlamydia [odds ratio (OR) 0.93 per week, 95% CI 0.84–1.03] but this was not statistically significant in the multivariate analysis (p=0.18).
Multivariate analysis of the chlamydia risk determinants showing the significant variables
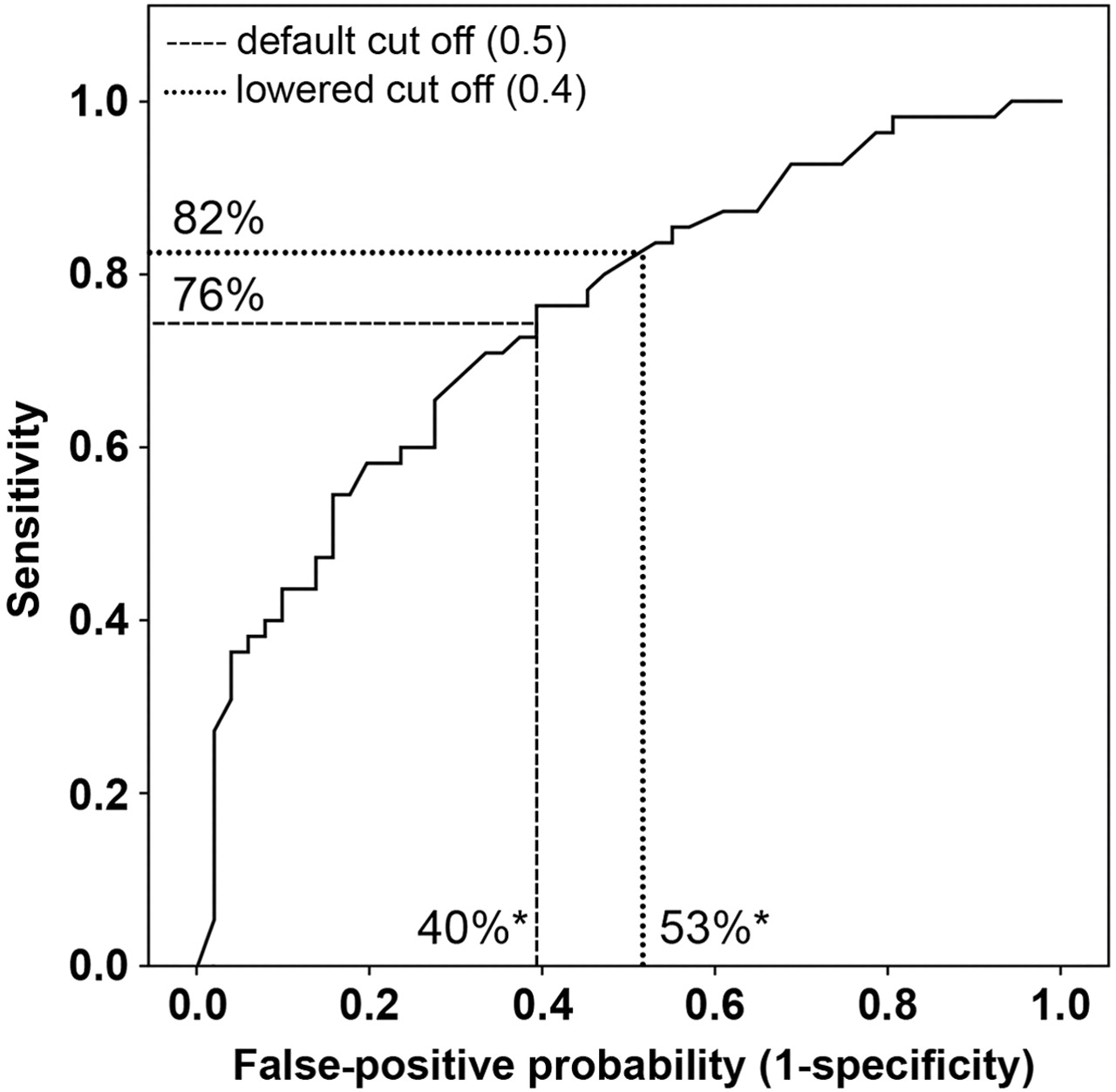
The adequacy of the multivariate model fit was assessed using the Hosmer and Lemeshow goodness-of-fit test, which resulted in a χ2 of 5.47 and a p value of 0.71, indicating adequate goodness-of-fit. Using the default cut-off of 0.5 for identification of positive cases by the multivariate model, the sensitivity was 76% and the specificity was 60% (Figure 1). Reducing the cut off to 0.4 increased the sensitivity of the model to 82% but decreased the specificity to 47%.
{kind=link}
Receiver–operating characteristics (ROC) curve of true-positive rate against the false-positive rate (1–specificity) for the different possible cut points of the multivariate model. Illustrated are the sensitivities and corresponding specificities at the default cut off (0.5) and at a cut off of 0.4. The area under the curve (AUC) is 0.76 (95% CI 0.66–0.85). *Corresponding to specificities of 60% and 47% for the 0.5 and 0.4 cut offs, respectively.
Discussion
Previous studies have varied in the concordant infection rates found. When culture methods were used to diagnose chlamydia, the concordant infection rate was 24% for female index cases and 46% for male index cases; this difference was statistically significant.5 A retrospective case note review in a clinic using nucleic acid amplification tests (NAATs) to diagnose chlamydia quoted a concordant infection rate of 76%, with no significant difference between the proportion of positive male and female contacts.4 Quinn et al. detected chlamydia in 68% of sexual partners of infected individuals, with no significant difference between male-to-female and female-to-male transmission frequencies.9 We also found no difference in the probability of infection between male and female contacts. However, our concordant infection rate of 52% was lower than those quoted in other studies using NAATs. This difference can be attributed to the different inclusion criteria; in the study by Quinn et al., for example, only heterosexual couples who reported having had sex within the last 30 days were recruited. A high concordant infection rate strengthens the case for epidemiological treatment of all sexual contacts. However, a concordant infection rate of 52% suggests that there could be advantage in identifying ‘high-risk’ contacts for appropriate intervention using a predictive model.
The risk factors for acquiring chlamydia in the community have been well documented. Fenton et al. using data from the National Survey of Sexual Attitudes and Lifestyles (NATSAL 2000) identified non-married status, age and partner concurrency or two or more sexual partners in the past year as independent risk factors for infection with C. trachomatis.10 Other studies also identified young age and multiple partners as significant risk factors for chlamydial infection.11,–,13 Unprotected sex and presence of genital symptoms were significant in some studies but not in others.14 15 We also identified young age and a higher number of sexual partners as risk factors for chlamydia in our cohort. Chlamydia contacts who reported genital symptoms or who had unprotected sex with the infected partner were at a greater risk of testing positive for chlamydia (ORs of 2.41 and 2.08, respectively) but these factors were not statistically significant in our study (p=0.18 and 0.31, respectively).
The current dilemma facing the clinician is weighing the interests of the individual patient (avoiding unnecessary antibiotics and building natural immunity to chlamydia16,–,19) against ‘public health’ interests (spread of untreated infection) and the possibility of developing complications from untreated infection. Using such a predictive model would have to be weighed against the lost opportunity of offering treatment to infected patients during their first visit. The clinician, therefore, needs reassurance that the predictive model used in clinical practice consistently performs well. Large-scale studies would be required in order to develop the most accurate model. The number of predictor variables included into the model also needs consideration. A highly sensitive and specific model that requires many predictor variables may be expensive in terms of time taken to gather the information required and in interpreting the data collected. A more parsimonious predictive model, including only a few highly significant variables, may not perform as well but may eliminate the need for a formal medical consultation. Finally, it is known that predictive models perform better in the datasets used to develop them. The chosen model must therefore be validated in a variety of clinical settings before suggesting any changes to the current treatment guidelines.
The results from this study can also be used when discussing epidemiological treatment with patients who present to sexual health services as chlamydia contacts. Such individuals would be able to make a better informed decision, based on their individual risk factors, on whether to accept the health care professional's offer of antibiotics for chlamydia without definitive proof of infection. These data can also help direct scarce clinic and health adviser resources towards a higher-risk group; more time can be spent giving these individuals information regarding the infection and treatment, advice about how to avoid onward transmission and re-infection, partner notification and discussion of future strategies for risk reduction.
We recognise that this study has a number of limitations that may have influenced the findings. The patients were asked to complete the questionnaire after the interview with the medical practitioner, which may have had an effect on patient recall. In addition, the number of individuals recruited was small, decreasing the power of the study. This is because we only recruited ‘proven’ chlamydia contacts (i.e. when the chlamydia status of the index case could be verified), which depended on the patient's ability to provide their partner's details, such as their partner's date of birth. Furthermore, we have no data on the individuals who declined to participate or who we did not identify as contacts. Consequently, we could not determine whether there were any statistical differences between enrolees and other chlamydia contacts who attended the clinic, or other chlamydia contacts identified from different settings. There are no similar studies on chlamydia contacts from the UK for direct comparison of patient demographics. The demographic details of infected individuals from the UK national audit on chlamydial infection were not significantly different from those of our cohort (age: 19–24 years: 50% vs 48%; White Caucasian: 78% vs 86%; MSM: 6% vs 5%; p=0.83, 0.45 and 0.67, respectively).20 We, however, recruited a significantly lower proportion of females compared to the national chlamydia audit cohort (17% vs 49%; p<0.01). This was expected, since most of the female contacts would be treated at the stage when a non-specific urethritis is diagnosed in the partner, and would therefore only be chlamydia contacts ‘in retrospect’. Since male-to-female and female-to-male transmission rates for chlamydia were identical in this study, this gender bias is unlikely to have affected the overall results. There were, however, insufficient numbers for gender-specific analysis; of particular interest would have been the effect of hormonal contraception on the chlamydia status of female contacts. Finally, we failed to ask about new sexual contacts since the last exposure to chlamydia, a potentially significant variable.
In conclusion, the concordant infection rate for chlamydia between sexual contacts was 52%. Young age, more than one episode of sexual intercourse with the infected partner and a greater total number of sexual partners were associated with a positive chlamydia result. These risk factors can be used when discussing epidemiological treatment for chlamydia with individuals who present as chlamydia contacts. Larger studies are necessary to assess the benefits and risks of changing to a policy of offering epidemiologic treatment to ‘high-risk’ contacts only, identified using a predictive model such as the one described here.
Acknowledgments
The authors would like to thank Mr A Gokul, Ms J Mabbs, Ms C Leggat, Ms J Chernova and Ms C Weston for their help with recruitment of patients and data analysis.
References
Footnotes
-
Funding This study was funded by the University Hospitals of Leicester NHS Trust.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.