Article Text

Abstract
Objectives The aim of this Phase III, multicentre, open-label, randomised study was to compare the efficacy and safety of ethinylestradiol (EE)/drospirenone (DRSP) in a new flexible extended regimen that allowed the management of intracyclic (breakthrough) bleeding (MIB) with that of EE/DRSP in a conventional 28-day regimen in women with moderate-to-severe primary dysmenorrhoea.
Methods Women (aged 18–40 years) with moderate-to-severe primary dysmenorrhoea-related pain received a flexible extended regimen with MIB (flexibleMIB; minimum 24, maximum 120 days of continuous tablet intake for a flexible number of cycles to reach a treatment duration of at least 140 days with 4-day breaks between cycles) or a conventional 28-day regimen (24 active and four placebo tablets for five cycles) of EE/DRSP. The primary outcome was the number of days with dysmenorrhoeic pain over 140 days. Secondary outcomes included other dysmenorrhoea-related pain outcomes, bleeding profile, satisfaction and safety.
Results Overall, 223 patients received study medication. There were significantly fewer days with dysmenorrhoeic pain with the flexibleMIB regimen than the conventional regimen (difference −4.2 days, 95% CI −6.5 to −2.0; p=0.0003), as well as considerably fewer days with at least moderate dysmenorrhoeic pain (difference −2.5 days, 95% CI −3.7 to −1.3), dysmenorrhoeic pain that interfered with daily activities (difference −2.2 days, 95% CI −4.2 to −0.1) and pelvic pain (difference −3.4 days, 95% CI −5.9 to −0.9). Adverse events were similar with both regimens.
Conclusions Compared with the conventional regimen, the flexible extended regimen of EE/DRSP with MIB was associated with a significantly greater reduction in days with dysmenorrhoeic pain in women with moderate-to-severe primary dysmenorrhoea. The flexibleMIB regimen was also associated with greater improvements in dysmenorrhea according to the Clinical Global Impression rating scale and was generally well tolerated.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://jfp.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Primary dysmenorrhoea is characterised by cramping pain in the lower abdomen and/or pelvis just before or during menstruation, without any identifiable pelvic disease. Dysmenorrhoea usually presents with or shortly after menarche, is most prevalent in adolescent women and becomes less prevalent with increasing age.1,–,3 Estimates of the prevalence of dysmenorrhoea vary depending on the method of assessment, but range from around 20–90% in adolescents.4 Dysmenorrhoea can have a significant impact on quality of life and school/work absenteeism.3 Despite the high prevalence of dysmenorrhoea and the considerable effect that it may have on daily life, few women consult their physicians about their condition;2 additionally, low physician awareness means that dysmenorrhoea is often inadequately recognised and treated.1
Key message points
▶ Ethinylestradiol 20 μg/drospirenone 3 mg in a flexible extended regimen versus a conventional regimen resulted in significantly fewer days with dysmenorrhoeic pain in women with primary dysmenorrhoea.
▶ In the investigators' assessment, more women in the flexible extended regimen group were ‘very much’ or ‘much’ improved, compared with the conventional regimen group.
▶ Women were generally satisfied with their regimen, and satisfaction scores were similar between the two groups.
A range of treatments exist for dysmenorrhoea, and the majority of women self-medicate with over-the-counter (OTC) non-steroidal anti-inflammatory drugs (NSAIDs), resulting in reduced pain.2 3 However, NSAIDs are associated with gastrointestinal adverse events (AEs)/complications that can cause high levels of morbidity and cost.5
Although the results from a systematic review did not find a conclusive effect for the use of combined oral contraceptives (COCs) with a conventional 28-day regimen in women with dysmenorrhoea,6 it is thought they may have a positive effect in this setting. There is evidence that fixed extended COC regimens may be effective in such women.7 It is postulated that extending active hormonal intake of COCs beyond 28 days might have use in reducing the frequency and intensity of menses. This may consequently lead to a reduction in the symptoms of dysmenorrhoea and the factors that influence dysmenorrhoea (such as pituitary gonadotropin production and ovarian activity).
This study was designed to compare the efficacy and safety of a flexible extended regimen of ethinylestradiol (EE)/drospirenone (DRSP) that allows the management of intracyclic (breakthrough) bleeding (flexibleMIB) with a conventional 28-day regimen of EE/DRSP in women with moderate-to-severe primary dysmenorrhoea.
Methods
Study design
This was a Phase III, multicentre, open-label, randomised, active-controlled, parallel-group study conducted in 26 centres in Germany and three centres in the UK between December 2007 and December 2009.
The study (ClinicalTrials.gov identifier, NCT00569244) was conducted in accordance with the International Conference on Harmonisation–Good Clinical Practice guidelines and Declaration of Helsinki. All participants had to have voluntarily signed an informed consent form before entering the study.
Study population
Women aged 18–40 years (≤30 years for smokers with a daily cigarette consumption of ≤10) with moderate-to-severe primary dysmenorrhoea (moderate-to-severe menstruation-related pelvic pain in at least four of six of the preceding cycles) were enrolled. Moderate dysmenorrhoea was defined as requiring OTC analgesics during menstruation with significant pain relief upon intake, as well as the presence of symptoms that interfere with usual activities. Severe dysmenorrhoea was defined as requiring analgesics during menstruation, with inconsistent relief from OTC analgesics, prescription analgesics required in at least some cycles, as well as discomfort that resulted in an inability to work or to carry out usual activities. Additionally, to meet the inclusion criteria, patients were required to have a self-rated sum pain total score of at least eight on the Andersch and Milsom dysmenorrhoea grading scale8 over the two baseline menstrual cycles.
At the screening phase, eligible women were grouped as COC switchers (who were required to have a washout phase comprising three menstrual cycles, the second and third of which constituted baseline cycles one and two) or COC starters (who did not require a washout phase and simply had two baseline cycles).
Study regimens
Eligible women were randomly allocated to one of two regimens of EE/DRSP: a flexibleMIB and a conventional 28-day regimen. For the flexibleMIB group, women took EE 20 µg/DRSP 3 mg at around the same time each day, continuously for at least 24 days (mandatory phase). After 24 days, EE/DRSP tablets could be continued for up to a maximum of 120 consecutive days (flexible intake phase). During the flexible intake phase (Days 25–120) women were, however, instructed to finish the intake cycle by observing a 4-day tablet-free interval if they experienced three consecutive days of bleeding or spotting. The 4-day tablet-free interval had to be taken no later than after a maximum 120 days of continuous tablet intake. After each 4-day tablet-free interval, women started a new cycle with a minimum of 24 days and a maximum of 120 days. Treatment was intended to last at least 140 days and, therefore, a flexible number of cycles were required to reach this duration, with the 140 days including at least one 4-day tablet-free interval.
For the conventional group, women took EE 20 µg/DRSP 3 mg for five 28-day cycles (total 140 days); each cycle consisted of 24 days of active hormonal intake followed by a 4-day hormone-free interval (during which women received hormone-free tablets).
Patients were permitted to take ibuprofen as rescue medication (which was documented).
Study variables
The primary efficacy variable was the number of days with dysmenorrhoeic pain over 140 days. Dysmenorrhoeic pain was defined as any spasmodic pelvic, lower abdominal pain with possible radiation towards the back or thighs recorded in a daily diary in correspondence with a withdrawal and/or menstrual bleeding episode. Pain severity was self-assessed on a daily basis using a verbal rating scale with the following four categories: 0, no pain; 1, mild dysmenorrhoeic pain with no need for an analgesic; 2, moderate dysmenorrhoeic pain with need for an analgesic; and 3, severe dysmenorrhoeic pain with the need for an analgesic.
Secondary efficacy variables included: days with at least moderate dysmenorrhoeic pain; days with dysmenorrhoeic pain associated with withdrawal or unscheduled bleeding; days with pelvic pain; days with dysmenorrhoeic pain that interfered with daily activities; bleeding profile (including the number of days and episodes of bleeding/spotting by 90-day reference periods, bleeding intensity (none, spotting, light, normal or heavy) and the proportion of subjects with withdrawal and intracyclic bleeding during individual cycles); investigator-assessed global improvement in dysmenorrhoea (seven-point scale ranging from 1=very much improved to 7=very much worse); and user satisfaction (seven-point scale ranging from 1=very much satisfied, to 7=very much dissatisfied).
Safety evaluations included AEs, metabolic parameters, carbohydrate metabolism, vital signs, clinical laboratory tests, and physical and gynaecological examinations.
Statistical analysis
The study sample size was determined on the assumption that for the primary efficacy variable there would be a mean difference between the flexibleMIB and conventional groups of 5 days, with a standard deviation (SD) of 10 days. Based on a standardised effect size of 0.5, a dropout rate of 20%, α of 0.05 (two-sided) and 90% power, a sample size of 108 women per regimen was required to have 86 evaluable women per group. At screening, eligible subjects were sequentially assigned a unique three-digit patient identification number. Subjects were then randomised 1:1 using a computer-generated randomisation list using randomisation blocks of four. These blocks were assigned to study centres. Within each centre the allocation of a randomisation number was linked in a chronologically ascending manner to the sequence of arrival of the patients at the study centre.
All data were evaluated according to the type of data, that is, descriptive statistics (including at least arithmetic mean, SD, minimum, median and maximum) for continuous variables and frequency tables for categorical data. All women who took at least one unit of study medication and for whom at least one observation after dosing was available were included in the full analysis set (FAS). A two-sample t-test was used to analyse the primary efficacy variable. For the difference between the two treatment groups, two-sided 95% CI were calculated for the primary efficacy variable and for the secondary efficacy variables related to dysmenorrhoeic pain. All other variables were analysed descriptively.
Results
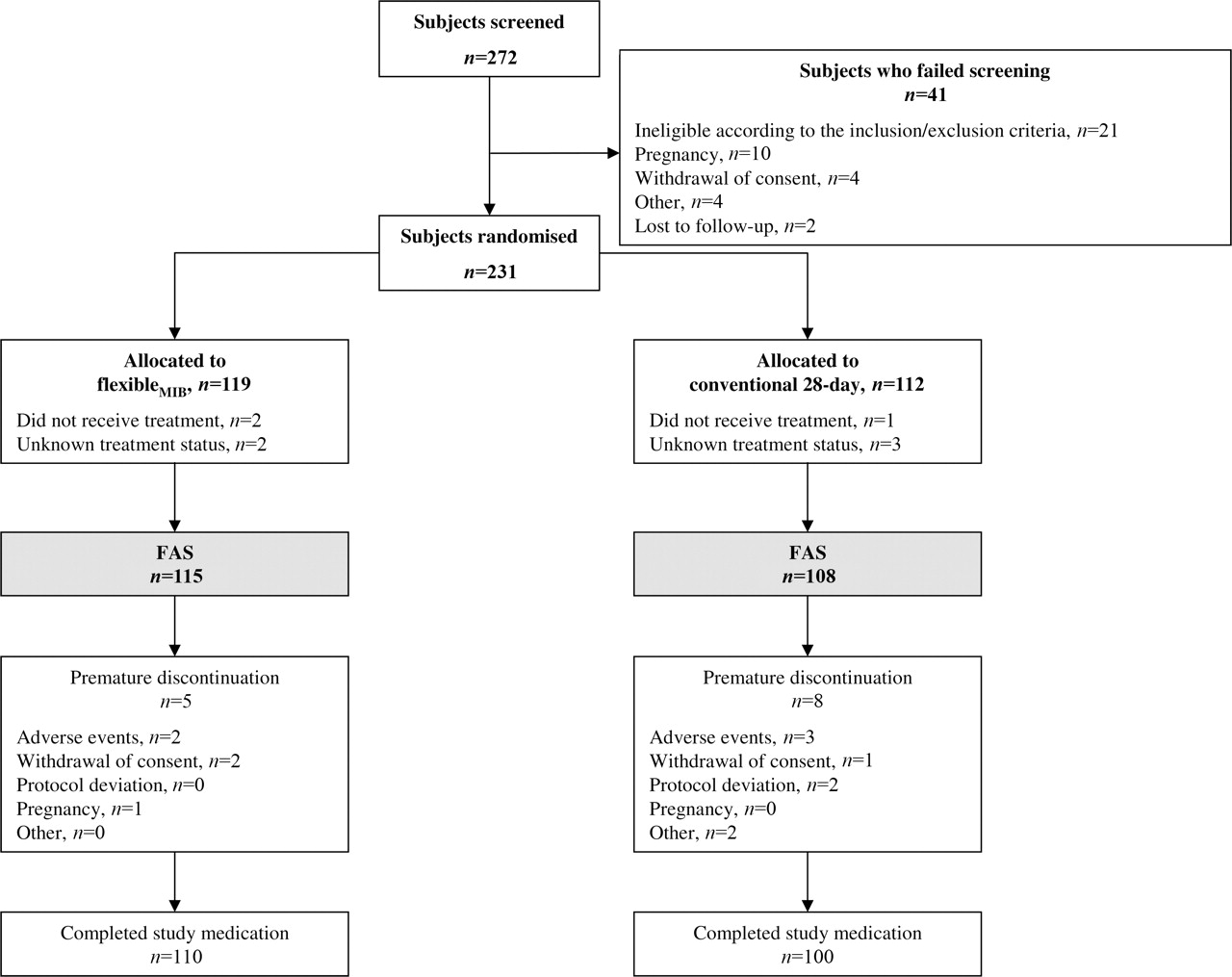
A total of 223 patients who received study medication were included in the FAS (flexibleMIB regimen, n=115; conventional regimen, n=108) and 210 patients (110 and 100, respectively) completed the study as planned (Figure 1). Baseline characteristics were similar for the two regimens and are outlined in Table 1.

Disposition of women through the study. FAS, full analysis set. MIB, management of intracyclic (breakthrough) bleeding.
Baseline demographics and clinical characteristics (full analysis set)
Overall, compliance was good for both regimens: the mean (SD) number of tablets taken in the flexibleMIB group was 151.8 (31.8) with a median of 146.0; corresponding tablet numbers in the conventional regimen group were 135.6 (26.0) and 140.0, respectively.
Primary efficacy variable
Dysmenorrhoeic pain
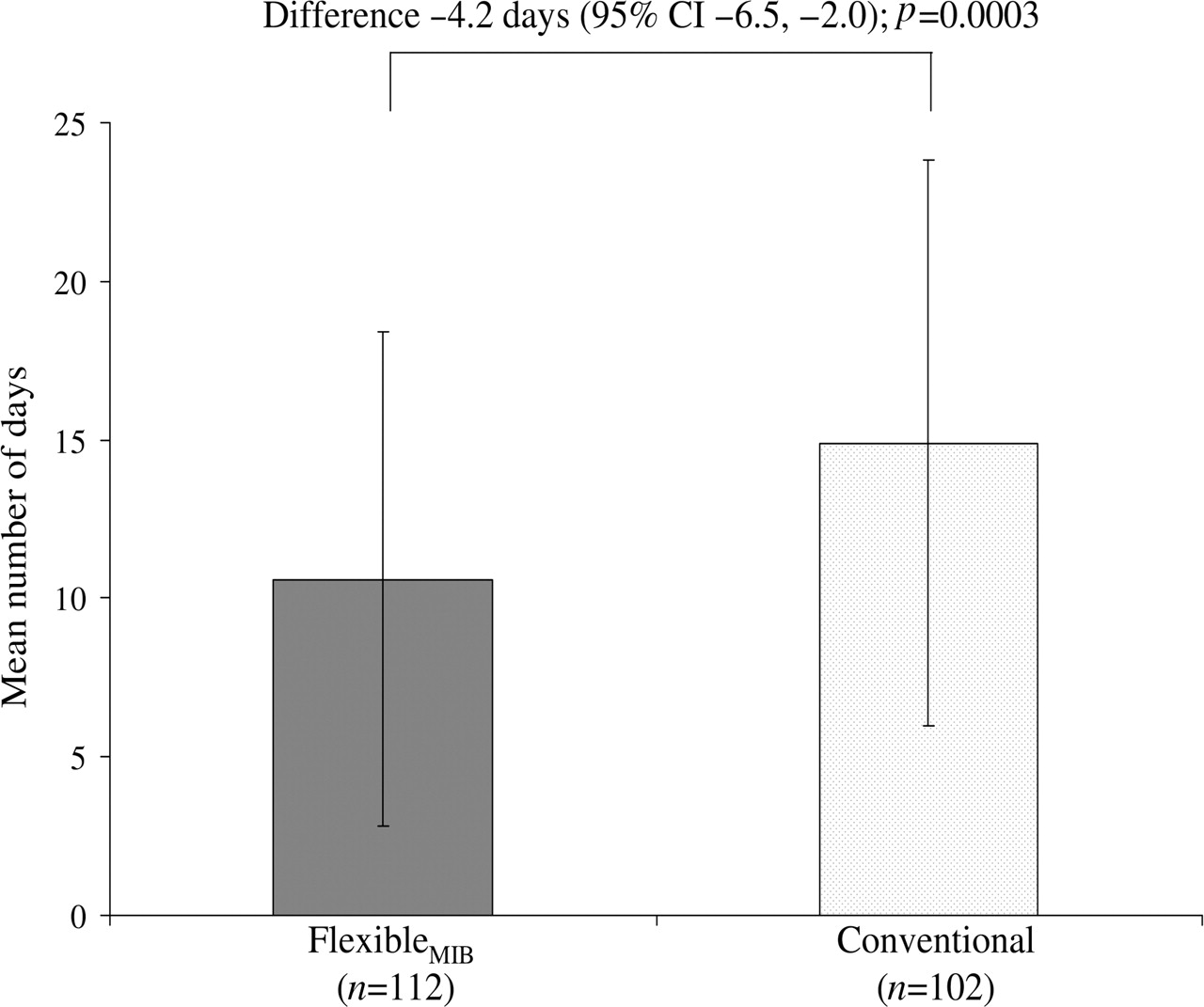
Over 140 days, the flexibleMIB regimen was associated with significantly fewer days with dysmenorrhoeic pain compared with the conventional regimen [mean (SD) 10.6 (6.7) vs 14.9 (8.9) days, respectively] (Figure 2). The difference between the two regimens was −4.2 days (95% CI −6.5 to −2.0, p=0.0003).
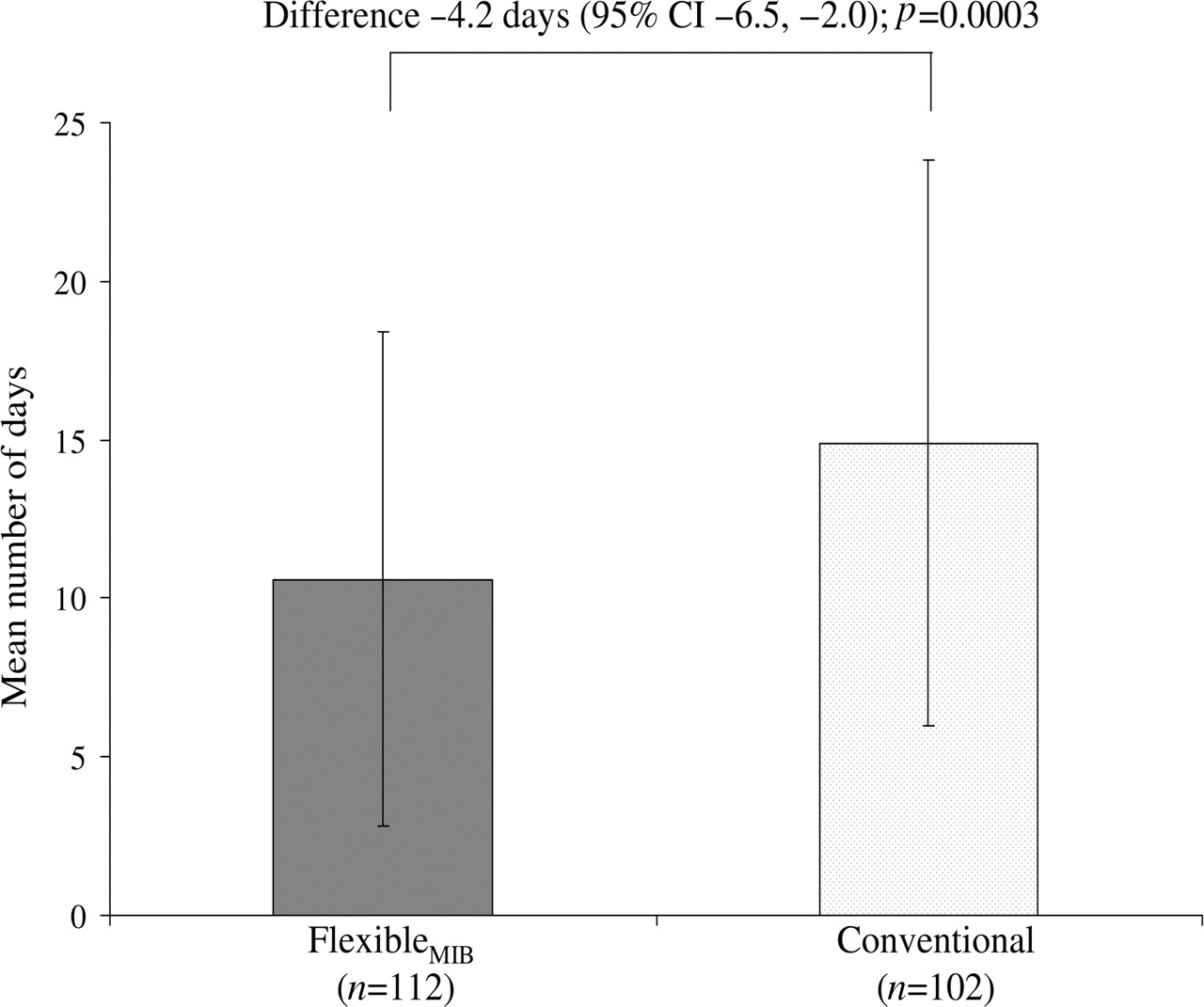
Mean number of days with dysmenorrhoeic pain over 140 days (full analysis set). CI, confidence interval; MIB, management of intracyclic (breakthrough) bleeding.
Secondary efficacy variable
Other dysmenorrhoeic pain outcomes
Consistent with the results of the primary efficacy variable, over 140 days, the flexibleMIB regimen also provided considerably fewer days with at least moderate dysmenorrhoeic pain (treatment difference −2.5 days, 95% CI −3.7 to −1.3), days with dysmenorrhoeic pain associated with withdrawal bleeding (−4.1 days, 95% CI −5.8 to −2.4), days in which dysmenorrhoeic pain interfered with daily activities (−2.2 days, 95% CI −4.2 to −0.1), and days with pelvic pain (independent of vaginal bleeding; −3.4 days, 95% CI −5.9 to −0.9) than the conventional regimen (Figure 3). The mean number of days with dysmenorrhoeic pain associated with unscheduled bleeding (−0.1 days, 95% CI −1.3 to 1.0) and the use of rescue medication (−1.0 days, 95% CI −2.5 to 0.5) was similar for both regimens (Figure 3).

{kind=link}
{kind=link}
{kind=link}
Mean number of days with various pain outcomes and use of rescue medication over 140 days (full analysis set). MIB, management of intracyclic (breakthrough) bleeding.
Other efficacy variables
Baseline comparison
Patients in this study had to undergo a screening period in which the number of days with pain from dysmenorrhea was recorded. Because patients were not receiving COCs for up to three menstrual cycles during this period, it was possible to compare the number of days with pain during screening with the number of days with pain during treatment. For this purpose, pre-treatment days with dysmenorrhoeic pain were projected to a 140-day period. The mean (SD) number of days with dysmenorrhoeic pain pre-treatment in patients who received the flexibleMIB regimen and the conventional regimen was 21.0 (7.3) and 22.0 (8.4), respectively (Table 1). When looking at the results of the primary efficacy variable (see above), the overall benefit of treatment in terms of a reduction in the total number of days with dysmenorrhoeic pain was approximately one-third for patients who received the conventional regimen and approximately one-half for patients who received the flexibleMIB regimen.
Number of days with dysmenorrhoeic pain in relation to cycle length
In an exploratory post hoc analysis, the number of days of pain in patients who received the flexibleMIB regimen were analysed according to the length of the flexible intake cycle. In patients with cycle lengths of less than 42 days, the mean (SD) number of days with dysmenorrhoeic pain was 13.0 (8.8); this was approximately two fewer days with dysmenorrhoeic pain, compared with patients who received the conventional regimen. In contrast, in patients with a cycle length of 42 days or more, the mean (SD) number of days with dysmenorrhoeic pain was 8.6 (6.3); this represented more than seven fewer days with dysmenorrhoeic pain, compared with patients who received the conventional regimen. This suggests that the advantage of the flexibleMIB regimen is a result of an extension of the menstrual cycle.
Bleeding profile
During the two 90-day reference periods in which the bleeding profile was analysed there were a lower mean and median number of bleeding/spotting days observed in the flexibleMIB group compared with the conventional group (Table 2). Likewise, the mean number of bleeding/spotting episodes was lower in the flexibleMIB group than in the conventional group. However, the mean length, maximum length and range of length of bleeding/spotting episodes were all slightly higher in the flexibleMIB group than the conventional group (Table 2).
Bleeding/spotting outcomes by 90-day reference period (full analysis set)
During the individual cycles, the proportion of women with withdrawal bleeding was similar in both regimens [range of the percentages over time for all cycles: 86–97% (n=9–110) in the flexibleMIB group and 87–98% (n=79–99) in the conventional group]. The mean length of withdrawal bleeding episodes tended to be longer with the flexibleMIB regimen and the onset of the withdrawal bleeding episode in the flexibleMIB group was 3 days early in relation to the hormone-free interval. A similar proportion of women had withdrawal bleeding of light or moderate intensity in the two groups, but there was a lower frequency of heavy intensity withdrawal bleeding in the flexibleMIB group versus the conventional group during the individual cycles [range 15.9–22.7% (n=2–24) in the flexibleMIB group and 24.5–29.8% (n=22–28) in the conventional regimen group].
The occurrence of intracyclic bleeding, the number of intracyclic bleeding days and episodes was noticeably higher in the flexibleMIB group in the first cycle, but decreased in the subsequent cycles. Despite these differences, the maximum length and the maximum intensity of intracyclic bleeding episodes were similar in the two groups.
Clinical Global Impression scale
Based on the investigator's assessment of the degree of improvement of primary dysmenorrhoea, 40 (34.8%) and 60 (52.2%) women receiving the flexibleMIB regimen were considered to be ‘very much’ or ‘much’ improved, respectively. The corresponding values in the conventional regimen group were 43 (39.8%) and 40 (37.0%). The number of women considered to be ‘minimally improved’ or ‘unchanged’ was 12 (10.4%) and 20 (18.5%) in the two groups, respectively, while the number of women with dysmenorrhoea that worsened (‘minimally’, ‘much’ and ‘very much’ worse) was 3 (2.6%) and 5 (4.7%), respectively.
User satisfaction
Women were generally satisfied with their regimen. Overall, 25 (21.7%) and 63 (54.8%) women receiving the flexibleMIB regimen were ‘very much satisfied’ or ‘much satisfied’ with it. The corresponding values in the conventional regimen group were 26 (24.1%) and 54 (50.0%). The number and proportion of women who were ‘minimally satisfied’ or ‘neither satisfied or dissatisfied’ was similar [20 (17.4%) in flexibleMIB group and 16 (14.8%) in the conventional regimen group]. In the flexibleMIB group, 7 (6.1%) women were ‘minimally’, ‘much’ or ‘very much’ dissatisfied compared with 12 (11.1%) women in the conventional regimen group.
Safety
In total, 82 (36.8%) women reported experiencing at least one AE, with a similar incidence between the flexibleMIB (n=44; 38.3%) and the conventional (n=38; 35.2%) regimens. AEs that occurred in >2% of the total sample are detailed in Table 3. No deaths or serious AEs were reported in the study.
Most frequent adverse events occurring in >2% of women in either regimen (full analysis set)
The levels of various metabolic parameters (including total cholesterol, triglycerides, low-density lipoprotein cholesterol and high-density lipoprotein cholesterol) and potassium remained normal and generally stable in both treatment groups. Similarly, levels of glycosylated haemoglobin remained normal and generally stable in both treatment groups over the course of the study. Neither the flexibleMIB regimen nor the conventional regimen adversely affected blood pressure, with mean values within normal limits. Mean body weight remained stable in both treatment groups. There were also no clinically meaningful changes in haematology and serum chemistry profiles with either regimen. No abnormal cervical smear test findings were observed at the final examination in any of the subjects. The results of the gynaecological examination revealed findings that were similar to those that would be expected in similar populations to the one recruited.
Discussion
In this 140-day study in women with moderate-to-severe primary dysmenorrhoea, a flexible extended regimen of EE/DRSP with management of intracyclic (breakthrough) bleeding was found to reduce dysmenorrhoeic symptoms and was associated with better outcomes than the conventional 28-day regimen of EE/DRSP. Compared with a conventional regimen of 24 days of active treatment followed by a 4-day tablet-free interval, the flexibleMIB regimen was associated with significantly fewer days with dysmenorrhoeic pain over 140 days, as well as considerably fewer days with at least moderate dysmenorrhoeic pain, dysmenorrhoeic pain associated with withdrawal bleeding, days in which dysmenorrhoeic pain interfered with daily activities, and days with pelvic pain. This effect may have been even more pronounced if the flexibleMIB regimen had been compared with a conventional 28-day regimen COC that uses a 7-day hormone-free interval and 21 days of active treatment. Additionally, investigator-assessed global improvement and user satisfaction scores were more favourable in the flexibleMIB group compared with the conventional group. The small difference between the groups in favour of the flexibleMIB regimen may be explained by its bleeding pattern with fewer menstrual periods compared with the well-known standard application of COCs that mimic a normal menstrual cycle. Furthermore, the flexible extended regimen may lead to better patient compliance.
In addition to reducing the frequency of withdrawal bleeding episodes by extending the menstrual cycle, the benefit of the flexibleMIB regimen was that it provided a method to manage any intracyclic (breakthrough) bleeding that occurred during the flexible intake phase (Days 25–120). By observing a 4-day tablet-free interval after experiencing three consecutive days of bleeding/spotting, breakthrough bleeding was turned into withdrawal bleeding. This facilitated better management of intracyclic (breakthrough) bleeding, enabling women to experience fewer overall days of bleeding over 140 days and fewer bleeding episodes, compared with the conventional regimen.
The MIB strategy meant that the bleeding profile was somewhat different between the flexibleMIB regimen and the conventional regimen; the mean length, maximum length and range of length of bleeding/spotting episodes and the mean length of withdrawal bleeding episodes were all slightly higher in the flexibleMIB group than in the conventional group. This probably relates to the fact that, by definition, the withdrawal bleeding episode under treatment with the flexibleMIB regimen often included the 3-day ‘wait and see’ period of bleeding/spotting that was instructed before women managed their intracyclic (breakthrough) bleeding by taking a 4-day tablet-free interval. The onset of the withdrawal bleeding episode occurred 3 days earlier in relation to the hormone-free interval in the flexibleMIB group compared with the conventional regimen. Again, this was likely a result of the 3-day ‘wait-and-see’ period.
The occurrence of intracyclic bleeding, the number of intracyclic bleeding days and episodes and the maximum length of intracyclic bleeding episodes varied markedly between the two groups. Such differences can be explained, at least in part, by between-treatment differences in the way in which data were analysed and differences in the two regimens themselves (as described above). In addition, the flexibleMIB regimen was designed to achieve prolonged bleeding-free intervals. While bleeding/spotting episodes of three consecutive days were to be managed by introducing a 4-day tablet-free interval (thus converting them into withdrawal bleeding episodes), episodes of bleeding/spotting of less than 3 days were to be ignored. Not managing shorter bleeding/spotting episodes was considered a suitable strategy to avoid too frequent withdrawal bleeding episodes; however, this ultimately increased the incidence of intracyclic bleeding in women who received the flexibleMIB regimen (data not shown).
There have been relatively few randomised studies that have specifically assessed the effect of continuous use or fixed extended regimens of COCs on dysmenorrhoea. Several studies have, however, assessed the effect of such regimens on menstrual-related symptoms in general, including dysmenorrhoea. In a study among women with menstrual-related symptoms (n=50), extending the number of consecutive days of active pills (up to a maximum of 12 weeks) was shown to reduce dysmenorrhoea, menorrhagia and premenstrual symptoms.9 Two studies have shown that the COC EE 30 µg/DRSP 3 mg, when used continuously for either 84 or 168 days, improved menstrual-related symptoms, including dysmenorrhoea.10 11 In a study of 32 women, continuous use of EE 20 μg/levonorgestrel (LNG) 100 μg for 168 days was associated with significantly fewer bleeding days that required sanitary protection, significantly fewer days with bloating and significantly fewer days with menstrual pain (all p<0.05) compared with a conventional 28-day regimen of EE 20 μg/LNG 100 μg.12 A COC containing EE 30 µg/chlormadinone acetate 2 mg in an extended regimen has also been shown to be effective in women with dysmenorrhoea. In a pooled analysis of three large-scale observational studies assessing the benefits and risks of this COC in an extended regimen (mean treatment duration 5.8 months), a reduction in dysmenorrhoea symptoms was observed, as measured by a reduction in analgesic use, absence from school/university/work and restrictions in leisure and sporting activities.13 Overall, the results from the current study and those previously published support the extended use of COCs to reduce menstrual-related symptoms such as dysmenorrhoea.
In this study, both regimens were generally well tolerated and the overall incidence of AEs was similar between the two groups.
Conclusions
Compared with a conventional regimen of EE/DRSP, a flexible extended regimen of EE/DRSP with management of intracyclic (breakthrough) bleeding was associated with better relief of dysmenorrhoeic complaints, including significantly fewer days with dysmenorrhoeic pain, in women with moderate-to-severe primary dysmenorrhoea. The flexible extended regimen has the advantage of being able to delay menstruation for up to 124 days. The flexible phase of the intake cycle allows women to react to the occurrence of breakthrough bleeding/spotting by initiating a 4-day break that concludes the cycle. The strategy of managing breakthrough bleeding/spotting by initiating a withdrawal bleeding has been shown to reduce the overall number of bleeding days, bleeding episodes and menses, and the number of days with pain in women suffering from primary dysmenorrhoea.
Acknowledgments
Medical writing support was provided by Matt Weitz and Clare Wheatcroft (of inScience Communications) during the preparation of this manuscript. This support was funded by Bayer HealthCare Pharmaceuticals. The authors would like to thank Dr Daniela Rouskova of Bayer HealthCare Pharmaceuticals for preparation of the clinical study report.
References
Footnotes
-
Funding This study was funded by Bayer HealthCare Pharmaceuticals, Berlin, Germany, the manufacturer of ethinylestradiol 20 µg/drospirenone 3 mg.
-
Competing interests Thomas Strowitzki has acted as a speaker for Bayer HealthCare Pharmaceuticals at various symposia and congresses. Bodo Kirsch and Jörg Elliesen are employees of Bayer HealthCare Pharmaceuticals.
-
Provenance and peer review Not commissioned; externally peer reviewed.