Article Text

Abstract
Background Uptake of the English National Chlamydia Screening Programme is lower than predicted necessary to result in a rapid fall in chlamydia prevalence. Peer-led approaches may increase screening uptake but their feasibility and acceptability to young people is not known.
Methods Focus groups and interviews with young women and men. Following interview, chlamydia postal kits were introduced to participants and their opinions on giving these out to their peers sought. Participants were asked for their views and experiences of discussing chlamydia screening and distributing kits to their friends 4–8 weeks after the focus group/interview. All kits returned to the laboratory over a 9-month period were recorded.
Results Six men (mean age 19 years) and six women (mean age 20 years) were recruited. In total 45 kits were distributed, 33 (73%) to female participants. 22 (67%) and 3 (25%) of kits given to females and males, respectively, were given to peers. Ten kits (22%; seven female, three male) all of which had been given out by females, were returned for testing. Participants generally felt positive about the idea of peer-led screening (PLS) using postal kits. However, embarrassment was a key theme, particularly among men. Generally women but not men were able to discuss PLS among their close friends. Both sexes felt PLS would be easier if kits were readily available in multiple sites, and chlamydia screening was more widely promoted.
Conclusion Female PLS but not male PLS was successful in recruiting peers to participate in chlamydia screening. An evaluation of the acceptability and cost-effectiveness of PLS is now indicated.
Statistics from Altmetric.com
Key message points
-
Female peer-led screening (PLS) is likely to be successful in recruiting peers to participate in chlamydia screening.
-
Males had positive reactions to PLS but found it difficult to discuss chlamydia screening and offer kits to peers.
-
Both men and women felt PLS would be easier to undertake if testing kits were readily available and chlamydia screening was more widely promoted.
Introduction
Chlamydia trachomatis is one of the most common bacterial sexually transmitted infections (STIs) in Europe. The prevalence is highest in sexually active young people under 25 years old with between 5% and 10% testing positive.1 ,2 The number of diagnosed cases is increasing in many European countries, in part due to increased testing and the use of more sensitive tests.1 People with genital chlamydia may experience symptoms of genital tract inflammation including urethritis and cervicitis, but the majority remain asymptomatic.1 ,2 Chlamydia is a significant public health problem because untreated chlamydia may lead to pelvic inflammatory disease, subfertility and poor reproductive outcomes in some women.1 ,2 In men it can cause urethritis and epididymo-orchitis and there is some evidence of a link between chlamydia and male infertility, although this is probably only true during acute infection.1,–,3 In both sexes infection can also cause reactive arthritis, conjunctivitis and proctitis.1 ,2
In England, the opportunistic National Chlamydia Screening Programme (NCSP), was set up as a control and prevention programme targeted at sexually active young people under 25 years of age.2 The NCSP facilitates screening in core sexual health services, through outreach activities and directly through provision via websites and/or by post.2 Nevertheless, current uptake of screening remains below model estimates of the levels probably needed to reduce chlamydia prevalence substantially and costs of delivering the programme vary widely.2 ,4,–,6 In 2010/11, the national target of 35% uptake among only 15–24-year-olds was missed with only 25% young people being screened, which rises to 32% if men and women attending departments of genitourinary medicine are included.7 However, the picture is more complex than this with the uptake of testing being approximately twice as much among women as men, with 42.7% of women and 22.7% of men being tested.
The House of Commons Committee of Public Account recently emphasised the priority of achieving cost-effective delivery of screening in a devolved health care system.5 The future direction of the English NCSP is to integrate chlamydia screening into sexual health and primary care services and to stop outreach work with low-risk groups that only identifies small numbers of positives, with a continued focus on partner notification.8 Increasing uptake in men has been difficult to achieve and Turner et al. recently demonstrated that partner notification and treatment of male contacts was a cost-effective method of increasing the number of chlamydia-positive men identified and treated.9 The challenge is likely to be in maintaining high levels of uptake among women who are not at low risk of infection and increasing identification and treatment of chlamydia-positive men while ensuring costs per test are below the current average of £45.5 ,6
Peer-led interventions and chain referral or respondent-driven sampling have been demonstrated to be successful in delivering public health benefits in a variety of settings and populations. These include reducing smoking among adolescents10; communicating safer sexual and injecting risk health education among vulnerable populations11 ,12; and efficiently recruiting populations that may be difficult to reach.13 We conducted a proof of principle study of a peer-led screening intervention to enhance chlamydia screening, by asking a small group of young people (men and women) whether they would be willing to give chlamydia testing kits to friends/members of their social networks and subsequently monitoring the number of tests returned to the laboratory.
Methods
One-to-one interviews with young men (n=6, age range 16–21 years, three in further education and three in higher education) and a single focus group with young women (n=6, age range 17–20 years, three in further education, two in higher education and one in full-time employment) were conducted prior to screening kits being given out. Follow-up telephone interviews (n=11, failed to contact one male participant) took place 4–8 weeks following first contact. Ethical approval was granted from the Somerset Research Ethics committee.
The Focus Group Topic Guide (copy available from the authors) was adapted to fit the questioning needs of the one-to-one interviews. The focus group lasted 2 hours, the interviews up to 1 hour and the telephone follow-up was of 15–20 minutes' duration. Females were recruited through a local Brook Centre (a nationwide sexual health support and advice service for under-25s). Males were difficult to recruit via this strategy, therefore they were sampled from local colleges and universities through a sexual health stand at fresher's week events. All participants had expressed an interest in undergoing chlamydia screening or had already been screened. The focus group took place at the local Brook Centre; the interviews took place at the Brook Centre or the University of Bristol. Following a description of the study and details of participation, written informed consent was gained from each participant.
The focus group and interviews followed a broadly similar set of questions around the following:
-
Thoughts and feelings about the chlamydia test and chlamydia in general
-
Awareness of the NCSP
-
Views on levels of awareness of chlamydia among friends and sexual partners
-
Exploration of how much they talk to friends and sexual partners about sexual health issues and how comfortable they feel having such conversations
-
Thoughts on how friends and sexual partners would respond to an invitation to be tested for chlamydia as part of a national screening programme.
The focus group and interviews were audio-taped and transcribed verbatim for analysis. One researcher (JL) conducted thematic analysis of the data to identify, compare and report patterns in the data.14 Two further researchers (PH and MH) reviewed the transcripts for agreement on themes. As this was an exploratory pilot study, saturation techniques were not applied to the data. In this study thematic analysis was used as a realist method14 aiming to report the experiences, meanings and reality of participant's feelings towards chlamydia screening. During analysis each transcript was studied repeatedly to create and develop themes that were reviewed and defined. These themes were inductive in nature, meaning that they were strongly attached to the data rather than existing theory. During the analysis process, continuous consideration was given to whether the analysis provided a convincing and well-organised representation of the data and the topic.
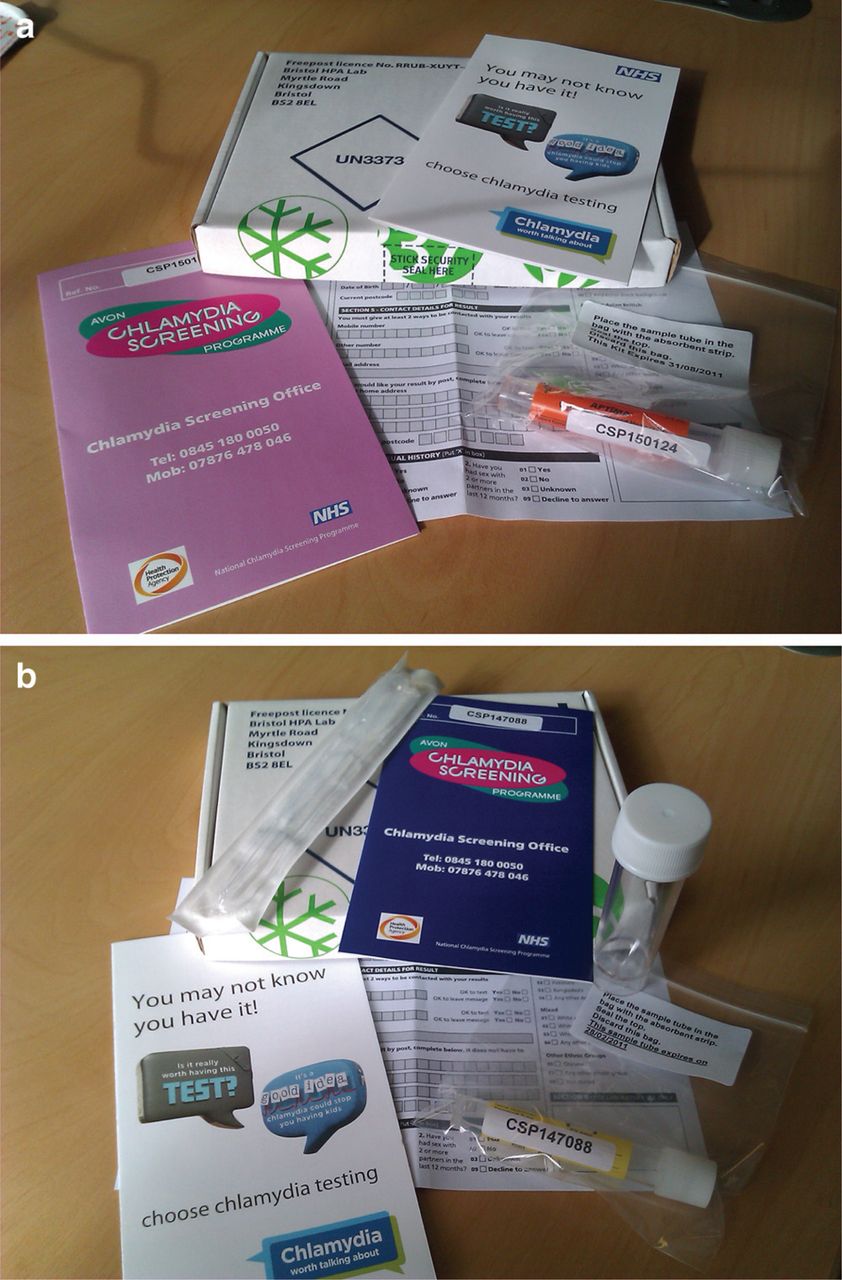
Chlamydia postal kits were shown to the young people during the second part of the focus group or individual interview. Each kit contained: a client details form; an NCSP leaflet; instruction leaflet for taking a vaginal swab (female) or urine (male); vaginal swab or urine collection tube and pipette; Aptima Combo 2® (Gen-Probe, San Diego, CA, USA) specimen tube; and a prepaid, pre-addressed, return postal box (Figure 1A,B). Participants were asked for their views on the kits and how they thought their friends and partners would view the testing kit. They were also asked whether they would be willing to take some of the kits and give them to partners, friends or family members of a similar age to themselves. We have termed this peer-led screening (PLS).
{kind=link}
(a) Showing a female chlamydia postal kit which contains: a client details form; National Chlamydia Screening Programme leaflet; instruction leaflet for taking a vaginal swab; vaginal swab collection tube and pipette; Aptima® specimen tube; and a pre-paid, pre-addressed, return box. (b) Showing a male chlamydia postal which contains: a client details form; National Chlamydia Screening Programme leaflet; instruction leaflet for collecting and processing a urine specimen; urine collection tube and pipette; Aptima specimen tube; and a pre-paid, preaddressed, return box.
Serial numbers of the kits were recorded. Participants were followed-up by telephone 4–8 weeks after the focus group or interviews using the Follow-up Interview Topic Guide (copy available from the authors) and asked whether they distributed any kits and for their views and experiences of discussing chlamydia screening. Kits returned were tracked using serial numbers in the local laboratory over a 9-month period.
Results
Chlamydia testing kits
Twelve young people took part in the focus group and interviews: six females in the focus group and six males in the interviews. A total of 45 kits were distributed following focus groups and interviews, 23 female kits and 22 male kits. The majority of kits were taken by women participants (n=33, 73%) all of whom reported giving out at least one kit to a member of their social network, with a total of 26/33 (79%) kits given out. By contrast only two men gave out a total of three kits. Details of the screening kits taken at initial data collection and those subsequently returned for testing are presented in Table 1.
Details of number of chlamydia testing kits taken by women and men and numbers given out and returned
At least one kit was returned from 5/6 of the social networks contacted by the participating women. In total 10 kits were returned for testing. All kits returned originated from female participants; none of the three kits given out by men were returned. The return rate indicates an average of 1.7 packs returned per woman participating, 38% (10/26) of the kits women gave to peers.
Results from qualitative data analysis
Awareness of STIs
Participants knew the names of common STIs but were unsure of what they actually entailed and potential presenting symptoms. Therefore knowledge and confidence in talking about symptoms was mixed. The majority of participants became aware of STIs and chlamydia between the ages of 13 and 17 years through school-based sexual health education:
“I found out in Year 10 in school when I had sex education. Late school years anyway, to be honest people were having sex by then anyway. So I guess the sex education was too late and should have been done earlier.” (Participant 11, male).
“I don't really know what it is. Doesn't it make it painful when you piss, is that actually what it is though? It doesn't scare me as much as AIDS and the rest of them.” (Participant 12, male).
Most males and females were aware that chlamydia could be present without symptoms but some were unsure and appeared more fearful of other STIs, arguably those with a higher media profile like HIV/AIDS. However, there was some doubt as to the understanding of chlamydia, suggesting that not all participants, particularly the males, had a clear understanding of STIs, the symptoms and the future implications of having had an STI such as chlamydia.
Discussing STIs with others and chlamydia screening
Both males and females said they would confide in their close friends about chlamydia screening. Men tended to feel less self-assured than women about discussing STIs and a few said that they might not discuss the issue seriously with their friends, due to embarrassment and fear of being judged or made fun of. It was felt by some males that STIs were a humorous subject among peers, perhaps to minimise the embarrassment when discussing sensitive topics.
“I think in my girl group of friends if one of us has had unprotected sex and hasn't done anything about it the other says ‘look no seriously you need to go down to Brook and get it sorted out’ basically.” (Participant 4, female).
“Yeah I’ve got some really close friends I’d tell pretty much anything, plus I’ve got really close to my mum lately and I can tell her things which is nice … [pauses] … well maybe not everything [laughs].” (Participant 2, female).
“Yes I would talk to friends; I would talk to close friends. There are people I wouldn't tell because I know they would tell others.” (Participant 10, male).
“It's usually joked about, for example programmes like South Park always make jokes about STIs and stuff like having AIDS. Boys tend to find it really funny. If I thought I had an STI I would talk to one of my close friends seriously and get advice from them.” (Participant 12, male).
It appeared that some males felt anxious and embarrassed about being screened for STIs in general practices or National Health Service (NHS) sexual health clinics even if they had previously been screened.
“It wasn't very nice. I was worried I would see someone I knew and at the time I wished I hadn't come.” (Participant 11, male).
“Very worrying. I really didn't like it. They try to make you feel at ease but for me it just didn't work. I wanted to cancel at the last min and then when I got there I felt like turning round and walking out.” (Participant 9, male).
However, most females described a less anxious view of chlamydia screening and sexual health. This was evident when they described their experiences prior to testing and also experiences of attending a screening appointment or using an NHS walk-in centre for testing purposes.
“When I had it done I had it in the walk in centre … and that was really nice, and it was like, there was one female nurse and one male nurse and they were just like really friendly and just talked me through it and I just went to the toilet and I came back and that was just it really, really straightforward.” (Participant 2, female).
“Then I did it once when you just have these boxes where you just take a women's one and go into the toilet and then just … I just thought that was quite good because like you know, its quick … painless.” (Participant 4, female).
This suggests that the females in this sample were more comfortable than the males with attending routine service providers such as clinics for sexual-health related issues.
Chlamydia screening postal kits
When chlamydia screening postal kits were introduced during initial data collection the discussion centred on how acceptable participants felt the kits and the testing process were. It was generally felt that the kits were a good idea and reduced barriers to access to screening by not having to attend a clinic, whether general NHS clinics or specialist sexual health clinics.
“It would save us coming here and sitting here trying not to look anyone in the eye, it would save lots of embarrassment.” (Participant 3, female).
“Having it text or e-mailed rather than a letter is really good. That is the biggest advantage. It sounds like a really good idea because it's easier and user friendly. I think they should be available everywhere and for everyone. And most importantly they should be free.” (Participant 11, male).
Some participants thought that females would be more likely to discuss and use the kits, and suggested that females are more open and conscientious about health issues. Some thought that men were more likely to joke about the postal kits than discuss them seriously.
“Overall I think girls are more inclined to talk about STIs and spread the word about the kits among their friends than boys. Although I hope this will change in the future if the topic becomes more open.” (Participant 11, male).
“Girls usually take these things more seriously. For boys it's more of a joke. Girls are also more alert and aware about STIs than boys.” (Participant 12, male).
This tendency for males to use humour when interacting with their peers may lead them to either consciously or unconsciously minimise the seriousness of STIs and perhaps to shrug off sexual health concerns.
Results from follow-up interviews
All participants were followed up between 4 and 8 weeks after initial participation. It appeared that males felt uncomfortable with discussing the screening kits and some preferred not to talk about it at all.
“I was too embarrassed to give them to people. At first I thought I would but when it came down to it I didn't feel comfortable doing it.” (Participant 9, male).
“I just don't feel happy giving a test to a friend. It's too much of a personal thing.” (Participant 11, male).
Although males found it hard to offer peers a kit, two participants were able to give kits to their friends, with mixed responses. One male underestimated how uncomfortable he would feel discussing the topic, and just left the kit outside his friend's bedroom door.
“… they were both pleased and we had a discussion about how good it was to not have to go to the clinic. They were really pleased and thought the whole process was such a great idea. Neither of them previously knew about it so it was quite a surprise.” (Participant 10, male).
“I gave it to my housemate and he thought it was really funny. We didn't really talk about it, he just took it and it wasn't mentioned again. I think he was pleased but didn't really want to show it.” (Participant 12, male).
Females felt more confident than males about discussing chlamydia screening and offering kits to their friends. They tended to approach the topic in a different way and appeared to be more comfortable with discussing it without the use of humour. They began telling peers about the research group as a way of introducing the topic of chlamydia screening.
“I just came out with it, because we were saying what we had been up to. I started by saying that I’d been to a research group and explained what it was about, chlamydia screening, and asked them if they wanted a kit to take away and use.” (Participant 5, female).
“I was doing my Florence Nightingale bit and saying how I’d done some research.” (Participant 3, female).
Women therefore took a more fact-based approach to discussing the kits with their friends and felt they were providing a valuable service. When asked what could be done to make kits more acceptable to young people, both males and females suggested similar ideas. Availability of kits was considered along with other items that could be included in the screening kits.
“I think that if this takes off it won't be so weird giving them to your friends because people will get to know that you can get them that way … [(put] condoms, and goodies in the pack, [and] raise awareness.” (Participant 4, female).
“I think just having them available in loads of places, schools, unis, union buildings and activities and doctors. Also, there should be a website you can order them from.” (Participant 12, male).
“I think if more people used them and got used to them being around it would be easier. I guess that just takes a lot of time.” (Participant 8, male).
It was felt that if kits were readily available in multiple sites and chlamydia screening was more widely promoted it might make it easier to give kits out.
Discussion
We undertook a proof of principle study of PLS by asking a small group of young people whether they would be willing to give chlamydia testing kits to friends/members of their social networks and then monitoring the number of tests returned. We found that women under 25 years old are potentially willing to give chlamydia testing kits to their social network. Of those tests distributed to peers there is a high return rate 38% (10/26) and, on average, 1.7 kits were returned for each participant. Conversely, men were reluctant to distribute kits to their peers and none were returned. Women were more willing than men to talk to their friends, with both genders expressing greater confidence about talking to their close friends about chlamydia screening. Embarrassment was a key theme among both sexes but much more so among men.
For men, the embarrassment of approaching peers and discussing sexual health-related issues in a personalised context and the difficulties some men have in general about seeing chlamydia as relevant to them, appear to be significant barriers to PLS.15 ,16 Embarrassment is likely to be a combination of young men feeling embarrassed about the stigma due to the association of chlamydia with promiscuity, being ‘dirty’ and non-desirable stereotypes, as it is an STI, and acknowledging taking responsibility for their own sexual health rather than their ‘fitness for sex’.15,–,20 It is possible that, for men, introducing the topic of chlamydia to peers conflicts with their cultural beliefs of masculinity, which include that men should be independent and self-reliant, be physically tough, not show emotion, be dominant and sure of themselves, and be ready for sex.15 ,21 It was felt by some males that STIs were a humorous subject among peers, perhaps to minimise the embarrassment when discussing sensitive topics or to hide their lack of knowledge. While women found the subject embarrassing they were confident they could discuss it with close friends. This may reflect in part a greater confidence in their knowledge about chlamydia.22 All participants, irrespective of gender, knew about chlamydia but women were more sure than men about the symptoms it may cause and the future implications of being infected which is consistent with previous studies.17 ,23,–,25 Women felt more comfortable than men in talking about sexual health issues and chlamydia, particularly when talking to close friends and were able to distribute to peers 67% (20/33) test kits taken. However, they did use the pretext of “participation in research” with female peers and humour with men when discussing the subject, which may have served to externalise and minimise the embarrassment. As part of this study we did not provide any formal teaching on chlamydia, or communication skills training, although their pack did contain an information leaflet and we did explore how they might go about broaching the subject with people so that they could reflect on this during the interviews/focus groups. Successful peer interventions have educated those providing such strategies regarding the risk of the behaviour in question (e.g. smoking) and provided communication skills training.10 This might result in increased uptake of chlamydia PLS among men and possibly also women.
Both male and female participants thought females tend to be more open and conscientious about health concerns and some thought they would be more likely to use the postal kits. This, combined with the fact that the females were more successful in distributing the screening kits, suggests that women are more ready to address health issues around STIs than men. Perhaps, this is not surprising as women but not men are considered at risk of infertility following infection2 ,26 and are also at risk of other potentially adverse sexual health outcomes such as pregnancy. Alternatively, it may be because young women are given more opportunity to discuss sexual health issues with their health care providers than males because of contraception and cervical screening. Nevertheless, both genders felt that if kits were readily available in multiple sites and chlamydia screening was more widely promoted it might make it easier to give kits out. This is consistent with the observations that men are willing to be tested if tests were readily available outside of routine health care settings including the use of postal testing kits.16 ,20 ,24 ,27,–,29
In this study, qualitative data collection exploring attitudes to participation in PLS was undertaken with men and women, prior to and after distribution of packs. This allowed us to evaluate how stated intentions and concerns at the time of distribution compared to the reality of distributing packs to peers and also to gain information on what approaches might promote uptake of PLS. However, this was a small proof of principle study involving only 12 participants so caution is needed when applying our findings to young people in general. We had intended to use focus groups for both sexes but it did not prove possible to recruit men to participate in one, so men were interviewed individually. We feel that it is unlikely that the apparent sex differences were actually due to methods of interviewing prior to administration of screening kits as this would be unlikely to influence the observed distribution of kits and feelings about doing this. The follow-up interviews were undertaken in a similar manner for both sexes. However, it is possible that the interactions between women in the focus group may have facilitated a greater understanding of the importance of chlamydia testing and resulted in increased confidence in subsequently discussing sexual health with peers and an increased willingness to do so.
This is the first published study combining qualitative and quantitative techniques to explore PLS as a potential tool for increasing coverage and uptake of chlamydia screening in men and women. Qualitative studies of chlamydia screening have tended to focus on women19 ,30 ,31 but, laterally, the opinions of men have also been sought.16 ,18 ,20 ,27 ,32 A particular strength of our study is that we obtained qualitative data before and after the intervention was undertaken, which has enabled us to relate participants' attitudes prior to the intervention to their uptake and distribution of kits.
In general there is a greater uptake of chlamydia screening among women compared with men.33 Our data are consistent with this and suggests that PLS is likely to be more successful at increasing coverage and uptake in women compared to men.
It is likely that female PLS could increase coverage and uptake of screening both among women and men. Concurrent publicity and widespread availability of testing may prove to be important in facilitating this as may the use of incentives.31 PLS has the potential to generate successive waves that could become self-sustaining. Two authors of this paper (JM and PH) recently published a cost-effectiveness model demonstrating that increasing the effectiveness of partner notification for women is a cost-effective way to identify infected men,9 although there are gender equity arguments for targeting both sexes in screening interventions.34 Thus PLS with high rates of partner notification is likely to be a cost-effective way of identifying infected women and men, and may prove particularly useful among high-risk groups that have been traditionally hard to reach.2 ,6 ,13 ,35 Further qualitative studies on men investigating the barriers to discussing STIs and sexual health in general among their peers are also needed. It is possible that a better understanding in men could lead to successful introduction of male PLS.
The recent House of Commons Committee of Public Accounts report on the NCSP highlighted that the Department of Health should identify the most cost-effective local delivery strategies while increasing testing numbers.5 PLS is likely to be one approach which could increase the efficiency of the NCSP. Evaluation of the value for money of PLS, as well as its effectiveness in detecting undiagnosed infections and the acceptability of the experience for those screened, is now indicated.
Acknowledgments
The authors are grateful to Brook Bristol for their support with this study.
References
Footnotes
-
Funding This work was supported by a grant from the Health Protection Agency R&D Pump-Priming & Small Initiatives Fund.
-
Competing interests Dr Patrick Horner has been involved in a multi-centre evaluation of a new molecular diagnostic test for Chlamydia trachomatis and Neisseria gonorrhoeae by Siemens Healthcare Diagnostics, for which his department received funding. Professor Rona Campbell is Director of DECIPHer Impact, a not-for-profit company set up by the Universities of Bristol and Cardiff to bring to the market evidence-based health promotion programmes. Jessica Loaring, Matthew Hickman, Isabel Oliver, Caroline Trotter, John Macleod, Karl Pye and Joanna Crichton did not declare any competing interests.
-
Ethics approval This study was approved by Somerset Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue