Article Text

Statistics from Altmetric.com
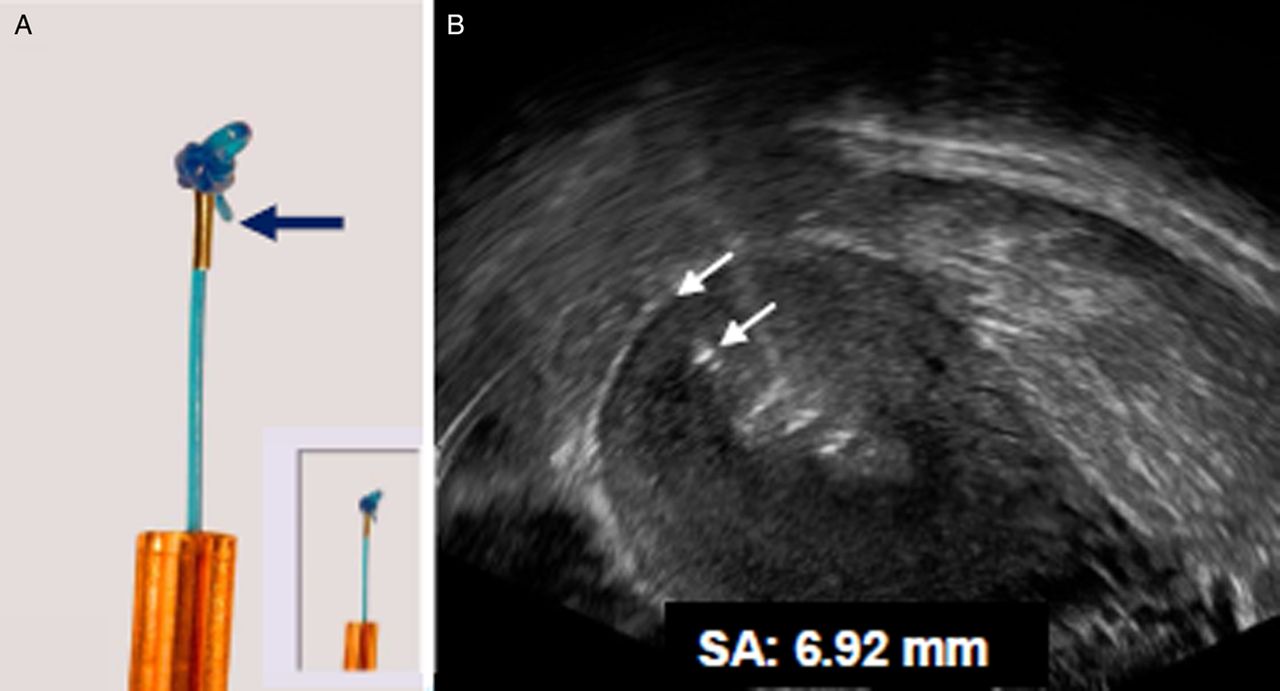
Readers of this journal will wish to be aware of an important improvement in the anchoring technology of the frameless copper intrauterine device (IUD), GyneFix® (Contrel Research, Ghent, Belgium). Long-term experience with this IUD is reviewed in a recent publication.1 As it has no supporting frame, anchoring of the IUD in the uterine wall is essential. During the learning period, or if the provider is unsure if anchoring was correctly achieved, it is recommended that the correct position of the IUD in the uterine cavity should be confirmed. This can easily be achieved using ultrasound, by measuring the distance between the uppermost copper cylinder/sleeve and the uterine serosa (SS-distance). However, the ‘anchor’ itself (a knot at the upper end of the polypropylene thread) is difficult to visualise although this may be necessary in some cases. The new ‘visualised anchor’, a stainless steel element attached to the thread immediately below the knot, was developed 3 years ago to help the provider to check its correct position. Currently available GyneFix devices have the visualised anchor and the packaging is marked with this information. The anchor is illustrated in Figure 1.
{kind=link}
(A) A tiny stainless steel element, 2 mm long and 0.5 mm wide, is added on the anchoring thread immediately below the anchoring knot (magnification ×2.5). Inset: actual size. (B) On ultrasound, the metal part of the anchor is clearly visible and its distance from the serosa (SA; white arrows) can be measured easily in virtually all cases.
A multicentre study was conducted to evaluate the position of the visualised anchor in relation to the uterine serosa as assessed by ultrasound examination at insertion and at follow-up.
Three hundred and nine women (194 nulliparous and 115 parous) requesting GyneFix for contraception participated in this evaluation at five centres in Europe. All insertions were done in consecutive patients in each centre. Following insertion, the stainless steel element was identified on ultrasound and its position in relation to the serosa of the uterus was measured (SA-distance). In 306 of the women the SA-distance could be measured. Two hundred and eighty-one of the 309 women were followed up 1–2 months after insertion and the SA measurement was repeated. The remaining 28 women were not followed up at the study centres as they had come from abroad for insertion only. The SA-distance was again measured in 77 women between 1 year and over 3 years later. The mean SA-distance in the 306 women was 6.0 (range 2.0–24.0) mm at insertion in the parous group and 5.4 (range 1.3–11.0) mm in the nulliparous group. At the first follow-up in 281 women the SA-distance was 6.0 (range 2.0–12.0) mm in the parous group and 5.5 (range 1.1–11.0) mm in the nulliparous group. The SA-distances were not significantly different. The exceptionally large SA-distance of 24 mm in one patient was probably due to insertion in the anterior uterine wall. No follow-up could be done in this patient. In the 77 women who were followed up for 12–42 months, the mean SA-distance at insertion in the parous group was 5.2 (range 3.0–8.5) mm and in the nulliparous group 4.8 (range 1.3–7.0) mm. For those who were followed up for 36 months or longer, the final SA-distance was 5.1 (range 3.0–8.5) mm in the parous group and 4.9 (range 1.3–7.0) mm in the nulliparous group. The visualised anchor was highly visible on ultrasound in all cases as illustrated in Figure 1.
This study with the new visualised anchor suggests that the position of the anchor in the uterine fundus can be checked with precision. The anchor is properly positioned in the fundus if it is inserted into the myometrium. To minimise the risk of incorrect placement, we recommend that the thickness of the uterine fundus should be measured by ultrasound if the provider has any doubt about GyneFix placement. Measuring the SA-distance will confirm if the anchor is correctly placed.
Footnotes
-
Competing interests Dr Wildemeersch is the developer of the GyneFix IUD. He acts as a trainer in GyneFix insertion for companies distributing the product. He has also been involved in the development and optimisation of new drug delivery systems for use in the uterus and he is currently an advisor on the development of new delivery methods for contraception and gynaecological treatment. He receives financial compensation for these activities.