Article Text

Abstract
Objectives To explore the attitudes, views and understanding of women attending a Hindu temple in London, UK towards cervical screening, human papillomavirus (HPV) testing and two HPV self-sample collection devices: the Dacron swab and Evalyn® brush.
Methods A mixed methods design comprising a survey and four focus groups was adopted. Focus group discussions were recorded and transcribed verbatim and explored using thematic framework analysis.
Results A total of 185 Hindu women completed surveys and 23 attended focus groups. Of the respondents 75% aged 25–64 years reported having cervical screening within the last 5 years; 85% had attended college or university. Familiar barriers to attendance for screening were identified: fear of pain and the test result, embarrassment, screener's attitude, inconvenient appointment times and difficulty with child care. Additional barriers cited included age and country of birth, with older and Indian-born women thought to be less likely to attend for screening. Self-collected sampling had a mixed reception. Women were not confident that their sample would be as good as a clinician sample and expressed concern about the impact that a positive HPV result might have on their relationships.
Conclusions Screening attendance in this highly educated group of Hindu women was slightly lower than in the general population (75% of women aged 25–64 years had been screened in the last 5 years compared with 79% in England as a whole). Familiar barriers to screening were identified. Women felt able to collect their own sample for HPV testing with a Dacron swab but lacked confidence that it would be as good as that obtained by a clinician.
- Cervical Screening
- Ethnic Minority and Cultural Issues
- Human Papillomavirus
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key message points
Screening attendance in these highly educated Hindu women is less than in the general population.
This population would currently prefer cervical smear tests as a positive human papillomavirus (HPV) test may cause relationship problems and HPV infection is untreatable.
These women had more confidence in a doctor's sample than their own, but believe younger women would have more confidence.
Introduction
The National Health Service Cervical Screening Programme (NHSCSP) in England invites all women registered with a general practitioner (GP) aged 25–49 years and 50–64 years to attend for free cervical screening, every 3 or 5 years, respectively. The stated target, to ensure that 80% of women are screened,1 has not been achieved in recent years.2 In 2011–2012 only 78.6% of women were screened at least once within the last 5 years.3 Women aged under 50 years were less likely to attend within 3.5 years when invited (73.5%) but more likely to have attended by 5 years (79%).1–5
Inequalities in the uptake of cancer screening by ethnic minority populations have been well documented,6–12 as has the association between poor uptake and social deprivation.1 ,13 ,14 Education and ethnicity have been shown to be predictors of attendance for cervical screening, with increased likelihood of attendance among more highly educated women and white British women.7 ,15 ,16
Populations are diverse and so exploring subgroups within them may provide further information regarding uptake of cervical screening. In the 2011 census, 1.5% of the population of England and Wales were recorded as Hindu (816 633).17 In addition, 58% of Hindus in 2001 were women aged 25–64 years and likely to be eligible for cervical screening.18 Of the Hindus in England 52% live in London, with Harrow and Brent in North West London containing the highest proportions of any of the London boroughs (20% and 17%, respectively).19
Reasons frequently given for not attending for cervical screening include the nature of the examination resulting in embarrassment and fear of pain20 ,21; practical issues with child care or absence from work, and concerns around the gender of the sample taker. Given the choice between a male or female GP, non-white women have been shown to be more likely than white women to say that they would prefer a female GP (42% vs 29%).22
Human papillomavirus (HPV) is a common sexually transmitted virus. Persistent infection with oncogenic HPV types is associated with an increased risk of cervical cancer.23–25 HPV testing therefore has a place in the field of cervical cancer prevention and, unlike cervical cytology, is proving to have great potential as a test using samples that women collect themselves and potentially in the privacy of their own home.26–28 Self-collected sample testing has been shown to have similar specificity and sensitivity to clinician sampling and is more sensitive than cytology.29–31 A test that removes some of the barriers to the uptake of cervical screening could be of benefit32 but it is important to recognise that the detection of this sexually transmitted virus may have adverse implications, particularly within some religious groups.33
It has been reported that women find self-collected sampling acceptable.26 ,30 ,34 ,35 There is some evidence that women from ethnic minority groups may be willing to collect their own samples, but Indian and Pakistani women were less certain about this than white British women.36 There is scant published research regarding cervical screening uptake and women's religion. Of the Indian population in the UK approximately 45% is Hindu.18 This research group has previously explored the attitudes and understanding of Muslim women towards cervical screening, HPV testing and self-collected samples.37 Religious networks are a useful route by which health messages can be disseminated to populations where screening uptake may be low.
Objectives
To explore the attitudes and understanding of Hindu women towards cervical screening, HPV testing and self-collected HPV samples and to ascertain their views on two different self-collection devices: the Dacron swab and the Evalyn® brush.
Methods
Participants and recruitment
Hindu women were recruited at an Open House Weekend Event in September 2011 and a Health and Vitality Day for ‘Yuvati’ (women aged under 40 years) in January 2012 organised by members of BAPS Shri Swaminarayan Mandir. Popularly known as the ‘Neasden Temple’, it is a place of worship for Hindus living in and around London and is located in the London Borough of Brent
Ethical approval
The study was approved by the UCL Research Ethics Committee.
Procedure
A mixed methods design was adopted using a survey (see online Supplementary Figure 1) and four focus group discussions (Figure 1).38 Women were approached at the above-mentioned events and were asked if they would complete a survey with the aim of gathering baseline data on screening attendance and demography. They were asked to provide contact details if they were interested in participating in focus group discussions. Of those returning the survey, 114 women consented to being contacted. A further seven were discounted as they did not indicate that they were Hindu, 31 were either too young or did not provide their age and seven provided illegible details. Those interested were subsequently contacted and invited to attend one of four focus group discussions held at the Mandir. The intention was to purposively sample if sufficient women agreed to participate. ‘Snowball sampling’ (i.e. using participants to recruit others) was incorporated into the recruitment process.
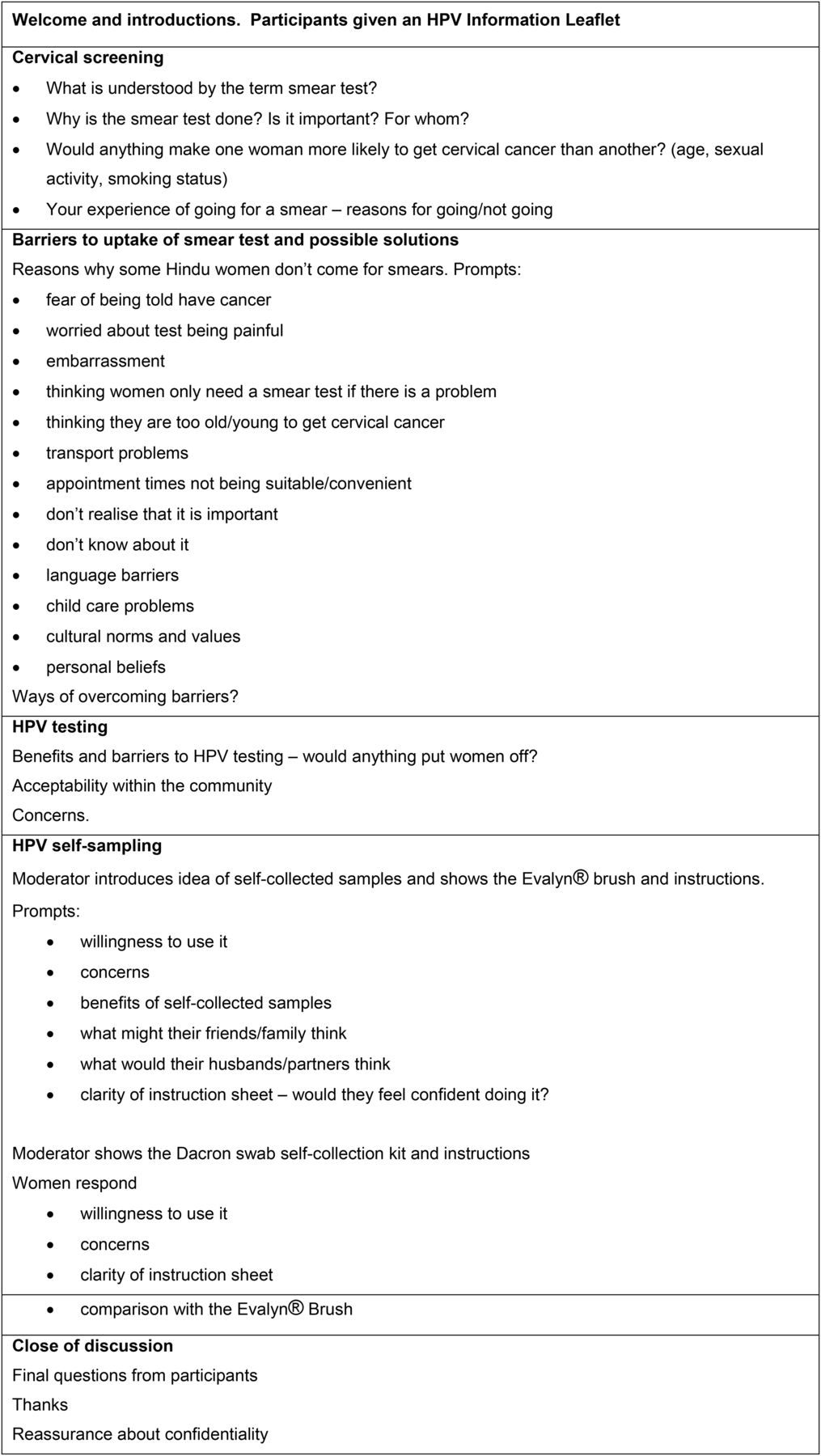
Topic guide for focus group discussions.
Women participating in the focus groups were asked to sign an informed consent form and were given £20 towards their time and travel costs. A donation was given to the BAPS Shri Swaminarayan Mandir in acknowledgement of their assistance and the facilities provided. Two researchers (JW and LC) moderated one and three focus groups, respectively. Representatives from the Mandir recommended that the groups be held in English with any translation being done within the group, as an outside translator could inhibit participants. Focus group discussions (lasting 45–60 minutes) were audio recorded and notes taken by LAB. During the discussions participants were given an information leaflet about HPV and Evalyn brush collection kits followed by Dacron swab collection kits, both with instructions. The Dacron swab resembles a cotton bud, approximately 15 cm long, which is inserted into the vagina and rotated for approximately 20 seconds. It is then broken off into a small tube with approximately 0.5 ml liquid specimen transport medium. The Evalyn brush consists of a pink stick with a brush at one end and a plunger at the other and is approximately 20 cm long. The cap is removed, the stick is inserted into the vagina, the plunger pushed to reveal the brush, which is rotated five times and removed. It is then retracted into its plastic tube and the cap replaced.
Analysis
The survey data were entered onto a Microsoft Office Access 2007 database. STATA/IC 12.1 was used for statistical analysis. Initial results were tabulated and formal statistical comparisons were made using the Chi-square (χ2) test and multivariate analyses using logistic regression. The focus group discussions were transcribed verbatim (LAB) and were analysed together with field notes. Recurrent themes were identified and organised into a matrix for framework analysis.38 Five main themes and twenty subthemes were identified (see online Supplementary Figure 2). Framework analysis was performed by both LC and LAB and any discordance was resolved by discussion.
Results
Sample
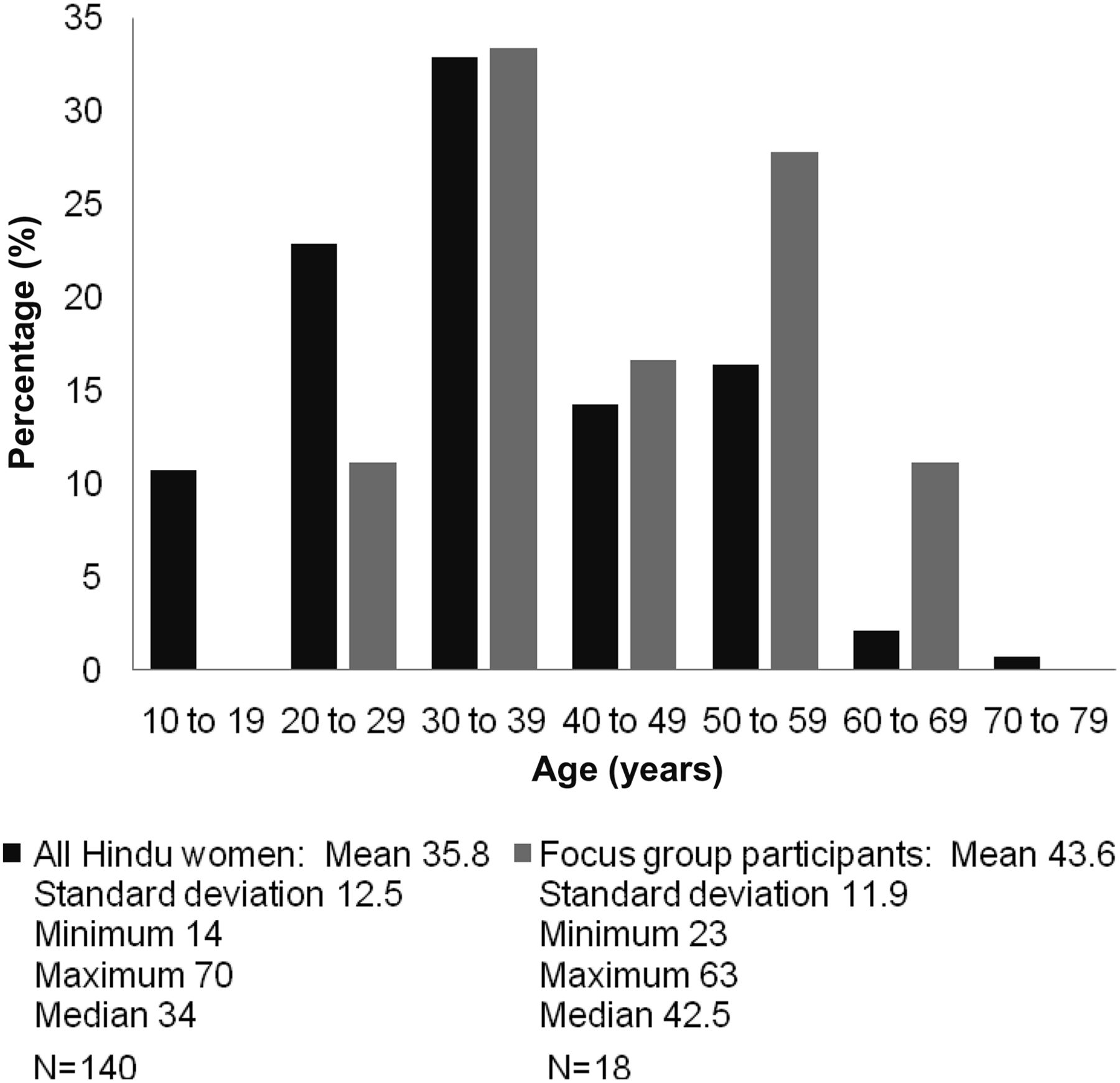
Surveys were returned by 204 women (see online Supplementary Table 1) with 19 being excluded as they did not state that they were Hindu. Of the remaining 185 surveys, 45 women omitted their age, five of whom were among the 23 women who participated in focus group discussions (Figure 2) (see online Supplementary Table 1). Of those returning a survey, 114 women consented to being contacted to participate in focus group discussions, of whom 49 were discounted as they did not indicate that they were Hindu, were either too young or did not provide their age or provided illegible details. Of the remaining 65, 18 could not be contacted or declined, leaving 31 women. This meant that purposive sampling was not realistic.

{kind=link}
{kind=link}
Age comparisons of the survey and focus groups.
Ethnic background was described as Indian by 92% of respondents. Of those aged 25–49 years who answered the question, 64% had had cervical screening within 3 years, but this figure rose to 75% for screening within 5 years. In women aged 25–64 years, 76% reported attendance within 5 years (Table 1). The women did, however, seem to be relatively regular attenders, with 40% of women aged 50–64 years having had more than three lifetime screens (Table 2).
Years since last screening by age (where given)
Number of lifetime screening tests by age group
Only 4% (n=5) of women aged 25–64 years indicated that they did not know about cervical screening, four of whom had been in the UK for less than 6 years.
Excluding women outside the recommended screening age, when exploring attendance for screening within the recommended interval (within 3 years for women aged 25–49 years and within 5 years for women aged 50–64 years), women who were single were significantly less likely than women who were married, living with a partner, divorced, separated or widowed to have attended [OR 0.19, 95% confidence interval (CI) 0.05–0.70]. This result remained significant after adjusting for age (OR 0.21, 95% CI 0.06–0.83). Additional adjustment for educational level did not affect these results.
Screening attendance within the recommended screening interval decreased with increasing level of education, with 77% (n=13/17) of women not going onto further education attending compared to 56% (n=57/101) of those who did. This, however, was not statistically significant (p=0.12).
Notably, 85% of respondents to the question indicated that they had attended college, university or undertaken postgraduate study (Table 3). Country of birth was statistically significant as a predictor of attendance for screening (p=0.024), with women being born other than in England or India more likely to attend within the recommended screening intervals. Parity was also significant as a predictor of attendance (p=0.037). Never having had sexual intercourse, not knowing about cervical screening and not considering it important, although statistically significant as predictors of attendance, were too few to be considered reliable.
Survey response by screening attendance
Some 21% of Hindu women returning surveys indicated they were afraid of pain, 17% were embarrassed and 8% were fearful that they would be told they had cancer.
Qualitative results
Understanding of cervical smear test
Although there was some confusion about whether cervical screening was also to “check the womb; and ovaries” [Participant 90 (P90)], overall women in the focus groups showed a good understanding of the purpose of the test. Some of the participants were clear that it was “to see if there's any abnormal cells” (P106) to detect whether one had a chance of getting cancer and to increase the chances of being able to treat this in the earlier stages. Some described the screening programme as for women “maybe married, unmarried if they are having a relationship” (P202). There was an acknowledgement of the association with sexual activity and that sex outside marriage may occur.
Barriers to attendance for cervical screening
Familiar barriers to attendance were confirmed by the focus group discussions: inconvenient appointment times, difficulty with child care, fear of pain, embarrassment, the sample taker may be male, the sample taker's attitude “they get angry and then you become more tense” (P90) and “some people don't go because of the frightening news they might get” (P105).
Further barriers to attendance identified within the focus group discussions were age and country of birth: “a lot of the older generation, the ones that are not well educated, don't bother” (P134). Participants said that in the case of their mothers: “They're brought up in India, they hardly take orthodox medicines or hospitals and clinics … no awareness about their health, I'm sure they were not even educated they didn't go to schools … so nobody told them about all this” (P90). Also “that generation felt that … if they die it is just destiny” (P103).
HPV awareness
Some women knew of HPV because of the vaccine and associated news stories: “there was a girl who had that kind of vaccine and she was in a coma” (P106). Some were aware that the vaccine was prophylactic and had to be given to young girls “because they are not in a relationship” (P202). There was limited discussion around HPV and cervical cancer, with one participant saying “No, no, no; HPV is not related to cancer” (P197) and another that it must be transmitted “from the partner probably” (P202).
Acceptability of HPV self-collected sample testing
Self-collection or clinician sample preference
Women were positive about the HPV self-collected sampling but comments were weighted towards preferring to have a test done at their doctor's surgery: “It [HPV self-collected sample] saves you going, saves you embarrassment … if you haven't got time to go … I would rather do it at the doctor” (P202). Their concerns stemmed from lack of confidence that they had done the test correctly: “prefer doctor's test because they are perfect and we are not perfect” (P204). An increased screening interval if HPV testing was adopted did not have any significant appeal: “it's not worth it” (P201).
Differences between generations
Regarding younger women, “I think they'll be fine they are really quite forward” (P120) but “the older generation they wouldn't know how to do it. It would be like a bit frightening for them” (P120). Also that widows “won't even bother I think … for them they are like more in grief really at that point”. They will just say “… let's ignore it we are not having sex” (P106). They felt it would be more appropriate for them to collect and return samples to the GP rather than receive them at home. One participant, however, felt strongly that “I know my daughter … she would rather go to the GP than do this, … she would find that really dirty having to do that herself” (P103).
Effect of an HPV-positive result
It was expressed that “If you know you are positive then it disturbs your relationship with your partner and if there is no treatment then there is no point in having it” (P197). Countering this, however, were the views expressed that “it is up to the individual … you have got to have trust in every marriage … not just me but my husband as well” (P134).
It was felt by some that HPV disclosure would not be such a problem for the younger generation: “they are broad minded, they are not like us … if someone knows or not they don't worry” (P196); “in our generation you never expect that your partner will be liaising with somebody else” (P197).
With regard to the wider family: “it's up to them to sort it out. … it is up to them I can't get involved in that” (P202). However, some women felt “the same thing is with the children also … because you have lost the trust” (P197).
Women commented that they would find a positive result “frightening” and that “they shouldn't … come out with a letter to say you've got this virus. They can say go to your GP” (P103).
Acceptability of the HPV self-collection devices and the instruction sheets
Women felt able to use the Dacron swab and instructions despite some concerns that “it did break easily” (P90) and it could be lost inside them. Overall it was considered “much easier; everyone can do it, even older generation women they don't know how to read or write even so even they can do it” (P120). The Evalyn brush, however, was not so well received: “this one is too big and painful [Evalyn brush]; this one [Dacron swab] is small, this one is good, easier” (P204) and it was a “bit complicated, isn't it?; there is so many things we have to do” (P87).
Discussion
This is the first study looking specifically at Hindu women in England and attendance for cervical screening. Hindus in the UK are moderately diverse in terms of deprivation with 7% living in the lowest decile of housing deprivation areas and 7% in the most advantaged decile.39 The participants in this small study represent well-educated Hindu women with an above-average education profile. Only 15% had not continued onto further education at a college or university compared with 39% of the Hindu population of England and Wales.18 The evidence from this study, however, does not support the hypothesis that a well-educated cohort would be more likely to attend for cervical screening than the general population, with a 5-year attendance rate for cervical screening of 75% vs 78.6% in the general population. This, may, however, simply be a fact of being Hindu rather than educational level.
Barriers to screening attendance were similar to those of other populations. It was suggested that the older generation of Hindu women (mothers and mothers-in-law) would be less likely to attend for screening or to collect a sample themselves, especially if they were born in India where there may have been less exposure to health care or education. This view on cervical screening attendance was not, however, totally borne out in this study. Within this group of women, 76% of those aged 50–64 years reported having had cervical screening within the last 5 years, and attendance for screening in accordance with recommended screening intervals was similar in women born in India and the UK (61% vs 63%).
With regard to self-collected samples for HPV testing, women accepted the Dacron swab collection device and instructions but were all unenthusiastic about the Evalyn brush, believing that not only was it big but they did not think that they would be able to use it. They were positive towards self-collected sampling but still expressed a preference to attend for testing at their GP surgery as they would have more confidence in the reliability of their GP's sample than their own. They were also reluctant to receive a positive HPV result, due to it being a sexually transmitted infection that could not be treated, and the impact this might have on the trust within their relationships.
Limitations
The quantitative part of the study involved a relatively small sample size, further reduced by a number of incomplete surveys. In addition, for simplicity, women were asked about their screening attendance within the last 3 years, whereas the NHSCSP reports coverage within the last 3.5 years, so the figures are not strictly comparable. In addition, women were recruited at health-related events, which might mean they were more engaged with health issues than the wider Hindu population in London.
There are limitations associated with holding focus group discussions within community groups. There may be concerns within the group around confidentiality despite clearly stated ground rules. Pragmatism meant that this was the most practical approach however.
It is recognised that by participating in research around cervical screening there may be a bias towards women who have attended for cervical screening and so the women are not necessarily representative of the Hindu population as a whole. There would be further self-selection by those women agreeing to participate in focus group discussions. This population in particular may not be representative of all Hindus in the UK.
Conclusions
It is hard to extrapolate the evidence gathered in this study to the Hindu population of England as a whole because it is a diverse population whereas this study population seems less so. However, the message these women are communicating is similar to that of other communities (e.g. Muslim37). They prefer to attend for cervical screening performed by a female professional than collect a sample themselves. Therefore, before self-sampling could be introduced on a larger scale efforts would need to be made to build the confidence of women regarding the quality of the sample they could collect and to address anxieties surrounding being told that they had an untreatable sexually transmitted infection. With regard to collection devices, as shown in previous research by this group, women find the Dacron swab the most acceptable device.
It would be useful to explore these issues further in harder-to-reach Hindu groups including those from less-educated backgrounds or those who do not attend for cervical screening. It would also be useful to explore methods of disseminating information around HPV and cervical cancer prevention within Hindu religious organisations and groups.
Acknowledgments
The authors thank Dr Sejal Saglani and the women who took part in this research and representatives from the BAPS Shri Swaminarayan Mandir.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Funding This study was funded by an Investigator Initiated Study Grant from Bayer AG. The study was also supported by Cancer Research UK Programme Grants (C569/A10404 and C8162/A10406).
Competing interests None.
Ethics approval UCL Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue