Article Text

Statistics from Altmetric.com
- intrauterine devices
- long-acting reversible contraception
- emergency contraception
- family planning service provision
- infertility
- education and training
We enjoyed reading the article by Moro et al.1 on their case series of the ultrasound-guided retrieval of lost intrauterine contraceptive devices using fine hysteroscopic grasping forceps.
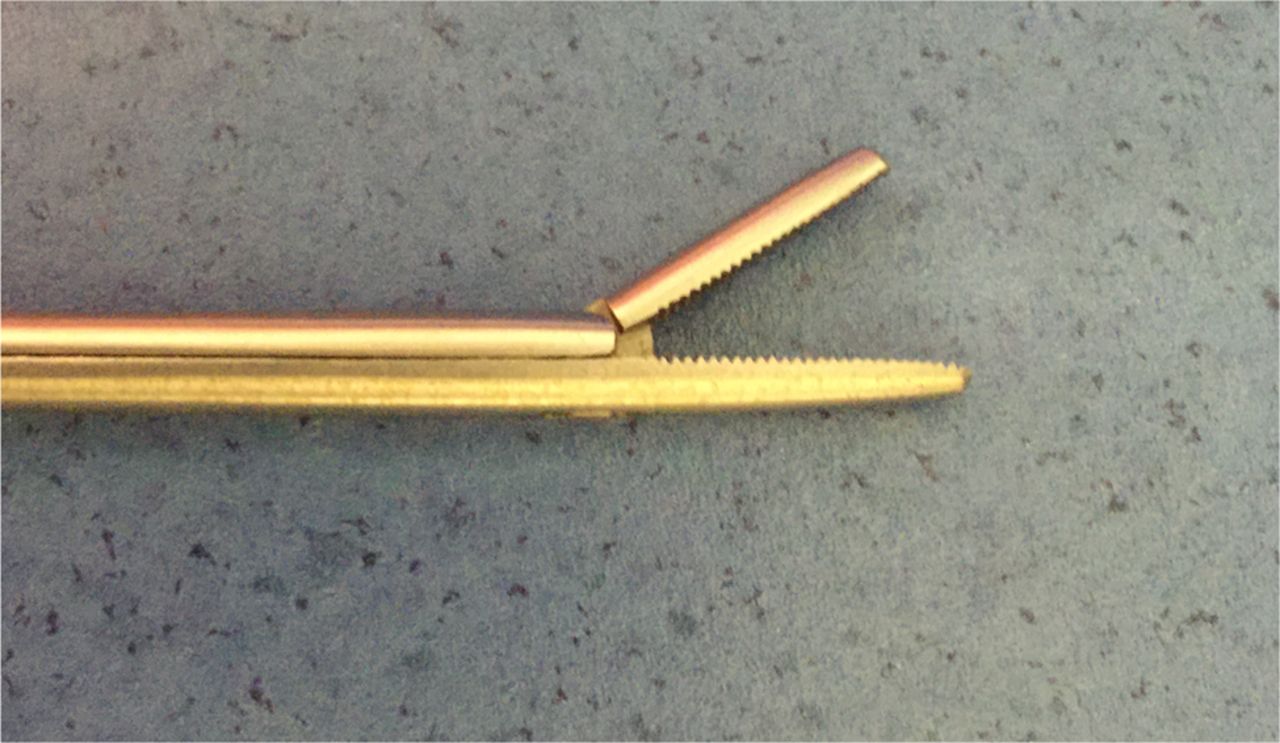
Like all contraception clinics we have our share of referrals with lost intrauterine devices (IUDs) and levonorgestrel intrauterine systems (IUSs). We scan all such women first. We then use a thread retriever and/or Spencer Wells artery forceps for blind retrieval as the first step in all cases. When this is unsuccessful we have been performing such retrievals in the outpatient contraceptive clinic setting under intracervical block (2 ml 1% lidocaine at 12 o'clock initially and if needed 2 ml at 3 and 9 o'clock positions). The anterior cervical lip is grasped with a vulsellum forceps. Instead of using a 5 Fr hysteroscopy grasping forceps transcervically as described by Moro et al., we have been using disposable single-use 22 cm Hartmann crocodile forceps (Instrapac™, Robinson Healthcare Limited) (Figures 1 and 2).

Hartmann crocodile forceps.

{kind=link}
{kind=link}
Tip of crocodile forceps.
Over the last 18 months we have removed 22 lost IUDs/IUSs under ultrasound guidance. The use of crocodile forceps enables removal and saves referral to a gynaecology clinic with an outpatient hysteroscopy service. A hysteroscope or hysteroscopy grasping forceps is unlikely to become readily available in a community contraceptive clinic.
Prior to using the crocodile forceps we used to refer women to the local hospital gynaecology service. As these were ‘routine’ referrals they waited 12 weeks or more and removal was performed at hysteroscopy, without local anaesthetic, without grasping the anterior cervical lip and without ultrasound, but with hysteroscopic grasping forceps as in Moro et al.'s1 series. Since using the crocodile forceps we have not needed to refer any women for outpatient hysteroscopy removal.
In 19/22 cases ultrasound showed that an IUD was correctly sited in the uterine cavity although the threads were not visible. All women had been asked by the booking clerk to take two tablets of naproxen 1 hour prior to attending but only 14/22 had done so. In one case the IUD was partially in the myometrium and in two others the IUD was stringless as the women had had their device inserted in China. We did not record the pain score or duration of the procedure but all devices were successfully removed and all women left the clinic immediately, with just 1/22 needing observation for a vasovagal episode for 10 minutes post-retrieval. Eight women were given two additional tablets of paracetamol to be taken in the clinic. Of the 22 women, nine were nulliparous and eleven had had caesarean births only. Similar successful removals in an office-based setting using ultrasound guidance have recently been described by Verma et al., 2 even in cases with embedded IUDs.
Avoiding referral to secondary care saves time, is safe and cost effective. It increases patient satisfaction (unpublished questionnaire study) especially when women are eager to start trying to conceive immediately or are suffering from unwanted effects due to the device.
Footnotes
Competing interests None declared.
Linked Articles
- Letters to the editor
- Highlights from this issue