Article Text

Abstract
Background Effective cervical screening reduces cancer incidence and mortality. However, these benefits may be accompanied by some harms, potentially including, adverse psychological impacts. Studies suggest women may have concerns about various specific issues, such as cervical cancer.
Aim To compare worries about cervical cancer, future fertility, having sex, and general health between women managed by alternative policies at colposcopy.
Design Multicentre individually-randomised controlled trial, nested within the National Health Service Cervical Screening Programmes.
Setting UK.
Methods 1515 women, aged 20–59 years, with low-grade cytology who attended colposcopy during February 2001–October 2002, were randomised to immediate loop excision or punch biopsies with recall for treatment if cervical intraepithelial neoplasia (CIN)2/3 was confirmed. Women completed questionnaires at recruitment and after 12, 18, 24 and 30 months. Outcomes were prevalence of worries at each time-point (point prevalence) and at any time-point during follow-up (12–30 months; cumulative prevalence). Primary analysis was by intention-to-treat (ITT); secondary per-protocol analysis compared groups according to management received among women with an abnormal transformation zone.
Results Cumulative prevalence of worries was: cervical cancer 40%; having sex 26%, future fertility 24%, and general health 60%. In ITT analyses, there were no statistically significant differences between management arms in cumulative or point prevalence of any of the worries. In per-protocol analyses, between-group differences were significant only for future fertility; cumulative prevalence was highest in women who underwent punch biopsies and treatment.
Conclusions There is no difference in the prevalence of specific worries in women randomised to alternative post-colposcopy management policies.
Clinical trial registration ISRCTN:34841617.
- cervical neoplasms
- cervical screening
- psychosexual
- service delivery
- epidemiology
Statistics from Altmetric.com
Key message points
In a randomised controlled trial, we investigated context-specific worries over 30 months between women following alternative management policies at colposcopy.
During follow-up, the percentages of specific worries in women were: cervical cancer, 40%; having sex, 26%; future fertility, 24%; general health, 60%.
The prevalence of worries reported by women randomised to immediate loop excision and punch biopsies with selective recall for treatment did not differ.
Introduction
Cancer screening involves balancing benefits, harms and affordability.1 Population-level benefits include reduced cancer incidence and/or mortality, and individual-level benefits include cancers avoided or detected earlier. However, these benefits are rarely achieved without some harm and considerable cost. For example, over-diagnosis and over-treatment are increasingly recognised as important consequences of screening2 ,3 because of their potential adverse effects, which include unnecessary health service expenditure and risk of physical and/or psychological after-effects.
There is potential for over-treatment in cervical screening, particularly regarding follow-up of women who have an abnormal primary screening test (either cervical cytology or human papillomavirus (HPV)). Internationally, one of the main follow-up options is referral for a colposcopy examination, which may be followed by immediate loop excision (LLETZ—large loop excision of the transformation zone; or LEEP—loop electrosurgical excision procedure) or targeted punch biopsies with recall for treatment of cervical intraepithelial neoplasia (CIN). Immediate loop excision removes the whole transformation zone and any lesions at a single appointment.4 However, it may result in over-treatment, and puts women without CIN at risk of physical after-effects (eg, bleeding, infection) and possibly preterm labour.5–8 A policy of biopsies and selective recall limits treatment to women with histologically-confirmed disease, but these women must return for a second clinic visit. Moreover, some disease may go undiagnosed.
Over-treatment could, potentially, increase the population-level psychological burden associated with screening. However, the psychological impact of alternative post-colposcopy management strategies has received little attention. Two small non-randomised studies and one large population-based randomised controlled trial (RCT), nested within the UK National Health Service Cervical Screening Programmes and known as Trial of Management of Borderline and Other Low-grade Abnormal smears (TOMBOLA), have been reported.9–12 The RCT found no difference in clinically significant anxiety or depression between women managed by a policy of punch biopsies and selected recall for treatment, and those managed by immediate loop excision.12 Evidence suggests women who have abnormal cervical screening tests experience a range of very specific concerns (eg, about cervical cancer, their sex lives, and future fertility).13–17 However, these concerns may not be well captured by generalised measures of psychological wellbeing (such as anxiety) and it is possible that, while different management policies may not differ in their impact on anxiety, for example, they could differ in their impact on specific concerns.
Using data from the TOMBOLA trial, we compared prevalence of context-specific worries over 30 months in women undergoing colposcopy and managed by policies of immediate loop excision, or punch biopsies and selective recall for treatment.
Methods
Study population
The study was nested within the colposcopy arm of the multicentre TOMBOLA trial.18 ,19 Eligible women were aged 20–59 years and had a routine screening cytology test during October 1999–October 2002 which showed mild dyskaryosis or borderline nuclear abnormalities (BNA)—broadly equivalent to low-grade squamous intraepithelial lesions (LSIL) and atypical squamous cells of undetermined significance (ASCUS), respectively. They could have up to one additional BNA result in the previous 3 years. Consenting women were randomised to cytological surveillance (repeat cytology tests in primary care) or a hospital-based colposcopy examination. Those allocated to colposcopy were sent a clinic appointment and a brief information leaflet describing the procedure and a second randomisation; this leaflet did not mention cancer, sex, or fertility.
Procedures and follow-up
At colposcopy, consenting women were further randomised, using a central telephone service, to immediate treatment by loop excision, or punch biopsies with recall for treatment if CIN2/3 was found. This randomisation was stratified by trial centre, age group, cytology grade, and high-risk HPV status at recruitment. Colposcopists were not blinded to the randomisation. Women who had an adequate colposcopy, and whose transformation zone was considered abnormal, received the assigned intervention. Women with a normal transformation zone were discharged to primary care follow-up by a cytology test after 12 months.
In the immediate loop arm, the whole transformation zone, including the abnormality, was removed. In the other arm, up to four targeted punch biopsies were taken from the most abnormal areas. Women with CIN2/3 on histology were recalled for treatment, usually by loop. Women with no CIN or CIN1 did not receive any further treatment at that time. Follow-up after biopsies or loop was by 6-monthly cytology tests in primary care. Results of these tests determined subsequent actions (next recommended cytology test date or colposcopy referral). If women were referred for colposcopy during follow-up, they attended local NHS clinics and were managed following local protocols. Approximately 3 years post-recruitment, which broadly represented the interval between screening rounds in the NHS screening programmes, women were invited for an exit colposcopy.
Ethical approval was obtained from local research ethics committees and participants provided written informed consent.
Psychological assessments
Women in this analysis were recruited to TOMBOLA from February 2001 onwards (when the psychosocial questionnaires were introduced), had an adequate colposcopy, and consented to the second randomisation (see online supplementary Figure S1; n=1515). The trial protocol specified that the psychological outcomes would include anxiety and depression and context-specific worries.18 This paper reports only these context-specific worries; the results relating to generalised anxiety and depression (assessed in a subgroup of 989 of the 1515 women included in this analysis) have been reported elsewhere.12
Psychological assessments were completed at the recruitment clinic (T0: baseline assessment) and by post at 12 (T1), 18 (T2), 24 (T3) and 30 (T4) months post-recruitment. The timing was designed to be between follow-up visits to avoid potential ‘spikes’ of distress associated with these. Outcome information came from the post-colposcopy assessments (ie, T1–T4). The outcome measures were worries about (1) cervical cancer, (2) fertility, (3) having sex, and (4) general health. These were assessed by the Process Outcome Specific Measure (POSM), an instrument developed from focus groups among women who had undergone a low-grade cytology test and follow-up.20 The instrument as a whole has acceptable repeatability and internal consistency and discriminant validity against the Hospital Anxiety and Depression Scale (HADS).21 The four relevant questions related to how the respondent had felt in a defined period (table 1). Responses options were 6-level Likert scales ranging from ‘strongly disagree’ to ‘strongly agree’.
Statement stems for the four outcome measures
The baseline assessment (T0) included questions on socio-demographics and lifestyle, the Multidimensional Health Locus of Control Scale (MHLCS),22 and the HADS.
Statistical analysis
Questionnaire response rates were computed for each time-point with the denominator comprising the number of women randomised. Socio-demographic characteristics of responders and non-responders were compared at each time-point.
Primary analyses were by intention-to-treat (ITT). Each outcome was analysed separately. Women's responses were reduced to a binary variable: agree/disagree. The point prevalence of ‘agreement’ was calculated at T0 (baseline) and T1–T4. This was done for all women (ie, combining trial arms) to describe temporal trends in the outcomes, and by arm to compare the psychological impact of the policies. Using data from T1 to T4, the cumulative prevalence of agreement was computed (ie, the percentage of women who agreed with the relevant statement at one or more follow-up time-points). Odds ratios for immediate loop versus biopsies and recall were computed by logistic regression. A model was built for cumulative prevalence and applied to the individual time-points. Risk estimates were adjusted for minimisation variables23 and significant confounders based on T0 data. Confounders were included in models if they were significant (p<0.05) on likelihood ratio tests (LRT). Final models had adequate fit.24
For future fertility, the primary analysis included all women. A supplementary analysis was restricted to women who indicated at specific time-points (T1–T4) that they were planning to have a child in the future.
A secondary per-protocol analysis was based on management received, and restricted to women who had an abnormal transformation zone. Women were grouped as follows: punch biopsies only; immediate loop only; and punch biopsies and treatment. The between-group cumulative and point prevalence of each worry was compared using χ2 tests.
Results
Participants’ characteristics
A total of 1515 women were included—754 randomised to immediate loop and 761 to biopsies and recall (see online supplementary Figure S1). Almost three-quarters (73%) were recruited with BNA cytology (see online supplementary table S1). The minimisation variables, and socio-demographic, lifestyle and psychosocial variables assessed at recruitment (T0), were balanced between arms. Worries about cervical cancer, having sex, future fertility and general health at recruitment were also balanced (table 2). Seven hundred and eighty-four women (52%) had an abnormal transformation zone at colposcopy (immediate loop, 343; biopsies and recall, 441) and were included in the secondary per-protocol analysis.
Primary analysis by intention-to-treat: prevalence of worries at recruitment and during follow-up, overall and by management arm, with OR*, 95% CI and p values from likelihood ratio tests
Response rates
At recruitment, 98% of women completed the psychosocial questionnaire (see online supplementary figure S1). Response rates were 73%, 67%, 64%, and 60% at 12, 18, 24, and 30 months, respectively, and did not differ between arms. At every time-point, the response rate was higher among women who were: older; recruited with BNA cytology; white; married/co-habiting; parous; not currently using oral contraceptives; or ex-smokers.
Cervical cancer worries
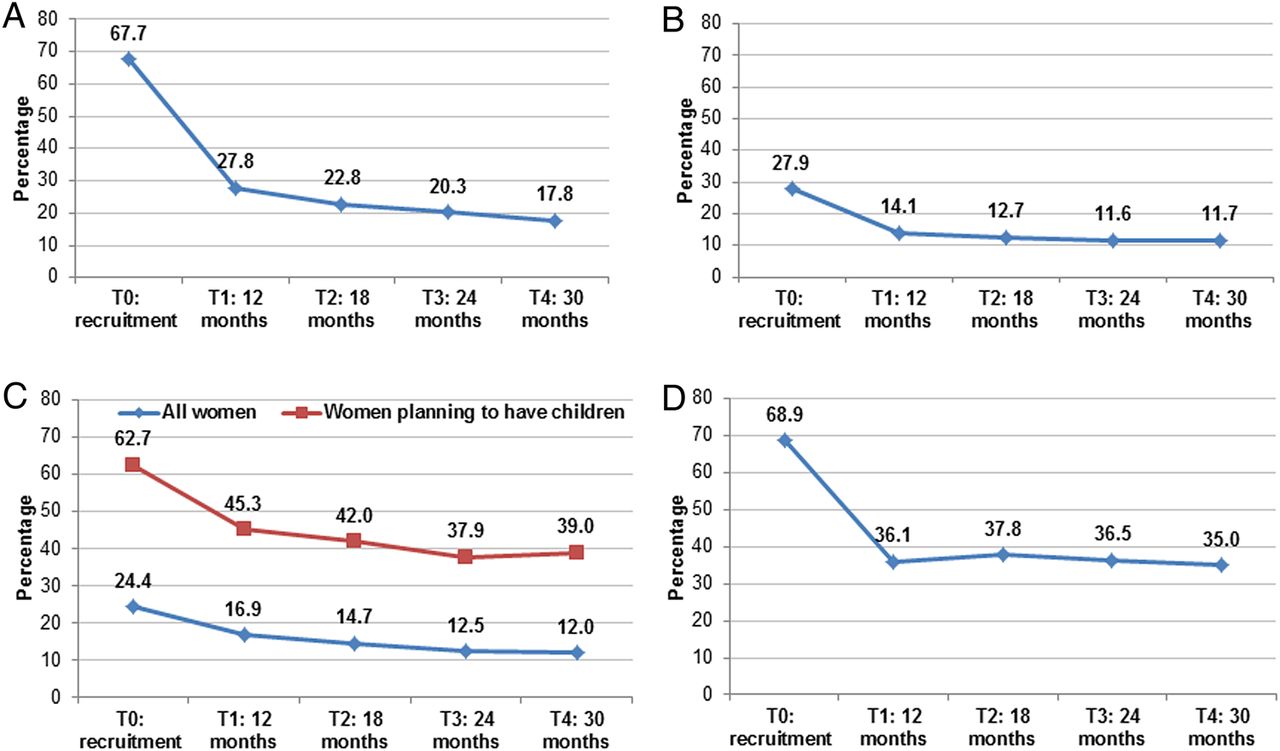
At recruitment, 68% of women were worried about having cervical cancer (figure 1). By 12 months, this had declined to 28% and fell at each subsequent time-point (18 months, 23%; 24 months, 20%; 30 months, 18%). The cumulative prevalence of cancer worries during follow-up (ie, at one or more of T1–T4) was 40%. In ITT analysis, the cumulative prevalence of cancer worries was slightly lower in the immediate loop arm than the biopsies and recall arm (39% vs 42%), but the multivariate odds ratio did not differ significantly from unity (OR 0.86, 95% CI 0.67 to 1.10; LRT p=0.232) (table 2). There were no differences between arms in point prevalence, or risk, of cancer worries at any follow-up time-point (T1/T2/T3/T4).
{kind=link}
Overall prevalence of worries at recruitment and each time-point during follow-up. (A) Percentage of women worried about having cervical cancer. (B) Percentage of women worried about having sex. (C) Percentage of women worried about their ability to have children. (D) Percentage of women worried about their general health.
In per-protocol analysis, cumulative prevalence of cancer worries was highest in women who underwent biopsies and treatment (55%), slightly lower in those who had biopsies only (49%), and lowest in those who had immediate loop only (43%); these differences were not statistically significant (p=0.120) (table 3). There were no significant between-group differences in cancer worries at any follow-up time-point (see online supplementary table S2).
Secondary per-protocol analysis: cumulative prevalence of worries during follow-up, by management received*
Sex worries
At recruitment, 28% were worried about having sex, falling to 12–14% during follow-up (figure 1). The cumulative prevalence was 26%. In ITT analysis, there were no significant differences between arms in cumulative prevalence (table 2), or point prevalence.
In per-protocol analysis, cumulative prevalence of worries about sex was highest in women who had biopsies and treatment, and slightly lower in other groups, but these differences were not statistically significant (table 3). No significant between-group differences were found at any individual time-point (see online supplementary table S2).
Future fertility worries
One-quarter of all women were worried about future fertility at recruitment, 17% at 12 months, and 12% at 30 months (figure 1). The cumulative prevalence was 24%. By ITT, there were no significant differences in cumulative or point prevalence between arms (table 2). When the analysis was restricted to women who were planning to have a child in the future, 45% were worried about future fertility at 12 months and 39% at 30 months (figure 2). In ITT analysis, neither cumulative nor point prevalence differed significantly between arms.
In per-protocol analysis of all women, cumulative prevalence of future fertility worries varied significantly between groups (biopsies and treatment, 48%; immediate loop only, 33%; biopsies only, 26%; p=0.001) (table 3). Significant between-group differences were also seen at 12 and 18 months. When the analysis was restricted to women planning to have a child in the future, significant between-group differences were found only at 12 months (see online supplementary table S2).
General health worries
At recruitment, 69% of women were worried about their general health. This fell to 36% at 12 months and did not change thereafter (figure 1). Cumulative prevalence of general health worries was 60%. This did not differ significantly between arms; nor did point prevalence (table 2).
In per-protocol analysis, cumulative prevalence of general health worries was highest in women who had biopsies and treatment and slightly lower in other groups (p=0.057) (table 3). There were no significant between-group differences at any time-point.
Discussion
Long-term post-colposcopy worries
In this study of context-specific worries reported by women undergoing colposcopy and related interventions, the proportion who reported worries at one or more time-points during 30 months’ follow-up was high (general health, 60%; cervical cancer, 40%; having sex, 26%; future fertility, 24%). Given how many women undergo colposcopy annually (whether following abnormal cytology and/or a positive HPV test), this implies that the population-level psychological burden of context-specific worries is considerable. In terms of possible explanations, rather than ‘resolving’ an abnormal screening test, a colposcopy is the start of a series of follow-up ‘events’ (which may include further tests or examinations in primary care or hospital clinics, biopsies or treatment over an extended time). For example, in TOMBOLA, women with a normal colposcopy were recommended to have annual cytology tests and other women 6-monthly tests; women only returned to routine recall after three negative tests. Being under ongoing follow-up at a colposcopy clinic has recently been shown to be an important driver of long-term distress.25 In some settings, HPV testing has recently been introduced in follow-up of women treated for CIN.26–28 Under these protocols, HPV-negative women are returned to routine recall, thereby removing them from extended follow-up. Whether this approach will alleviate women's worries remains uncertain. In recent qualitative work among women who had an HPV test as part of their follow-up, most were overwhelmingly concerned about their initial cytology result and/or its treatment, and the HPV test did not mediate these concerns.29
Alternative management policies
While immediate loop offers advantages to the health services because women can be investigated and treated in a single appointment, it may result in considerable over-treatment, at least among women with low-grade cytology.5 ,19 ,30 It is possible that this potential overtreatment could result in a greater population-level psychological burden because women may associate treatment with there being ‘something wrong’ with their cervix, irrespective of whether or not they actually had CIN. Indeed, some women view any treatment as undesirable.9 Alternatively, this policy could result in a lower psychological burden since it involves a single appointment and attending a colposcopy clinic is associated with considerable anticipatory distress.31 In fact, our ITT analysis found no significant differences between management policies for any worries, either over the entire follow-up period or at any individual time-point, in line with our findings for clinically significant anxiety and depression.12 Our findings are consistent with a small (n=100) non-randomised study from Sweden which reported no significant differences in state anxiety or sexual functioning at 6 and 24 months between women who did, and did not, have loop following punch biopsies.10 ,11 In contrast, another study reported lower anxiety in women who had immediate loop than in those managed by biopsy and selective recall; however, that study was also small (n=272), was not randomised, and administered a generalised measure of the psychological burden 1 week post-colposcopy when women managed by punch biopsy were still awaiting results.9
Because eligible women had low-grade cytology, half had a normal colposcopy and no further investigation or treatment at that time. The per-protocol analysis was conducted in recognition of this. Cumulative prevalence of every worry was highest in the group who underwent biopsies and treatment (although between-group differences were mostly not statistically significant). In terms of potential explanations, some women express a desire not to return to a colposcopy clinic,9 so a second treatment-related visit may generate distress and worries. In addition, returning for treatment extends the length of time a woman waits for a more ‘definitive’ outcome and this wait may induce worries. Moreover, women in the biopsy and treatment group had CIN2/3, and this diagnosis has been associated with increased anxiety post-colposcopy.32 Finally, women undergoing biopsies and treatment have more physical after-effects than other women, and physical and psychological after-effects appear related.6 ,33
Specific worries
In TOMBOLA, most women were recruited following a single low-grade cytology test and their risk of cancer would have been very low.34 The findings that more than one-quarter were worried about having cervical cancer at 12 months and one-fifth at 30 months are, therefore, of particular concern. This observation is not limited to our setting; among 100 women in Sweden who were followed post-colposcopy, fear of cancer was reported by 26% at 6 months and 30% at 24 months.11 The most likely explanation is that women commonly (but erroneously) think that cervical cytology is a test for cancer12 ,17 ,35 In TOMBOLA, during follow-up, women would have had several interactions with healthcare professionals both in hospital and in primary care facilities. The fact that so many remained worried about cancer suggests there may be some deficiency in services, information or support.
Given that women underwent investigations and procedures specifically for follow-up of abnormal cervical cytology, it was surprising that prevalence of worries about general health at recruitment (69%) and during follow-up (60%) was so high. We asked about general health because focus group research found that women who'd had abnormal cytology and follow-up were concerned about this. The high prevalence of these worries may, in part, be due to women with a high level of general health concerns choosing to participate in cervical screening and/or our trial which was investigating optimal management of low-grade cytology results. More generally, further research is needed to understand how an abnormal screening result and its follow-up translates into more general heath worries. As regards future fertility, in the Swedish study 31% of women aged 23–50 years reported fears about future fertility at 6 months and 20% at 24 months.11 Our percentages were slightly lower but we included women aged 50–59 years who would not have had such concerns. Our finding that one-quarter of women had worries about having sex during follow-up complements growing evidence that colposcopy and related procedures may impact adversely on women's sexual functioning.10 ,14 ,36–38
Strengths and limitations
TOMBOLA is one of the few longitudinal studies of psychological after-effects of colposcopy and the only randomised comparison of the psychological burden of alternative post-colposcopy management policies. Further strengths include the large size and population basis, and consideration—in this paper—of specific concerns raised by women with abnormal cervical cytology. The 52% participation rate compares favourably with population-based epidemiological studies.39 Questionnaire response rates fell over time and it is impossible to know whether respondents’ and non-respondents’ psychological outcomes differed. While the questionnaire was informed by the findings of focus groups and had acceptable psychometric properties,20 the outcome measures were single items and this is a limitation. It is possible that sending women a questionnaire asking about how they were feeling may have prompted some to report worries that they would not otherwise have been concerned about, but this is a limitation of all similar questionnaire-based studies. We distributed a brief standard information leaflet before colposcopy, but know nothing about other information provided to women (or that which they sought themselves) at the appointment or during follow-up. Women are likely to differ substantially in information seeking and receipt, but the randomisation should have provided balance between the arms in this regard. Neither the information leaflet, nor the letter which informed women in the immediate loop excision arm of their histology results, mentioned overtreatment so the worries reported here by these women should not reflect concerns associated with having received a procedure that may not have been necessary. Although there are some concerns about the impact of loop excision on pregnancy outcomes, these largely emerged in the scientific literature after TOMBOLA follow-up was completed (the last psychosocial questionnaire were dispatched in spring 2005), meaning that the results reported here for worries about future fertility should be unaffected. Almost all treated women had loop excision so the results do not necessarily generalise to other treatments (eg, ablation). Finally, while we describe patterns over time in each worry for all women in each arm, it is likely that these conceal different temporal trajectories in different groups of women (eg, for some women worries may decline over time while for others they may remain stable or rise); future research would be of value to describe these patterns and determine which women follow each trajectory.
Implications
We have previously shown that, in the UK context (with well-organised, population-based screening), in women referred to colposcopy with low-grade cytology, the policies of immediate loop excision and punch biopsies and selective treatment are equivalent in both clinical effectiveness (ability to detect CIN2/3 over 3 years) and cost effectiveness.19 ,40 Where they differ is in relation to the potential for over-treatment, which is greater with immediate loop. Despite this difference, the ITT findings reported here, together with our previous work on clinically significant anxiety and depression,12 indicate that the long-term psychological burden of the two policies does not differ.
Conclusion
The over-treatment associated with a policy of immediate loop excision at colposcopy does not translate into a differential prevalence of context-specific worries compared with a policy of punch biopsies and recall for treatment. Irrespective of how women are managed, the worries reported by women undergoing colposcopy and related interventions are multi-dimensional and may persist longer-term. Strategies to alleviate this psychosocial burden are needed to reduce the harms associated with cervical screening.
Acknowledgments
ISRCTN 34841617 (http://www.isrctn.org/). The authors are grateful for the cooperation and assistance that they received from NHS staff in the coordinating centres and clinical sites. They thank the women who participated in TOMBOLA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figure
- Data supplement 2 - Online tables
Footnotes
LS and SC contributed equally.
Collaborators The TOMBOLA Group comprises: Grant-holders: University of Aberdeen and NHS Grampian, Aberdeen, Scotland: Maggie Cruickshank (Principal Investigator 2009-), Graeme Murray, David Parkin, Louise Smart, Eric Walker, Norman Waugh (Principal Investigator 2004–2009). University of Nottingham and Nottingham NHS, Nottingham, England: Mark Avis, Claire Chilvers, Katherine Fielding, Rob Hammond, David Jenkins, Jane Johnson, Keith Neal, Rashmi Seth, Dave Whynes. University of Dundee and NHS Tayside, Dundee, Tayside: Ian Duncan, Alistair Robertson (deceased). University of Ottawa, Ottawa, Canada: Julian Little (Principal Investigator 1999–2004; currently Canada Research Chair in Human Genome Epidemiology). National Cancer Registry, Cork, Ireland: Linda Sharp. Bangor University, Bangor, Wales: Ian Russell. University of Hull, Hull, England: Leslie Walker.
Staff in clinical sites and coordinating centres: Grampian: Breda Anthony, Sarah Bell, Adrienne Bowie, Katrina Brown (deceased), Joe Brown, Kheng Chew, Claire Cochran, Seonaidh Cotton, Jeannie Dean, Kate Dunn, Jane Edwards, David Evans, Julie Fenty, Al Finlayson, Marie Gallagher, Nicola Gray, Maureen Heddle, Alison Innes, Debbie Jobson, Mandy Keillor, Jayne MacGregor, Sheona Mackenzie, Amanda Mackie, Gladys McPherson, Ike Okorocha, Morag Reilly, Joan Rodgers, Alison Thornton, Rachel Yeats. Tayside: Lindyanne Alexander, Lindsey Buchanan, Susan Henderson, Tine Iterbeke, Susanneke Lucas, Gillian Manderson, Sheila Nicol, Gael Reid, Carol Robinson, Trish Sandilands. Nottingham: Marg Adrian, Ahmed Al-Sahab, Elaine Bentley, Hazel Brook, Claire Bushby, Rita Cannon, Brenda Cooper, Ruth Dowell, Mark Dunderdale, Dr Gabrawi, Li Guo, Lisa Heideman, Steve Jones, Salli Lawson, Zoë Philips, Christopher Platt, Shakuntala Prabhakaran, John Rippin, Rose Thompson, Elizabeth Williams, Claire Woolley. Statistical analysis: Seonaidh Cotton, Kirsten Harrild, John Norrie, Linda Sharp. External Trial Steering Committee: Nicholas Day (chair, 1999–2004), Theresa Marteau (chair 2004-), Mahesh Parmar, Julietta Patnick and Ciaran Woodman. External Data Monitoring and Ethics Committee: Doug Altman (chair), Sue Moss, Michael Wells.
Funding TOMBOLA was funded by the Medical Research Council (MRC) 9970080 and NHS in Scotland and England. The funders had no role in the study design; the collection, analysis and interpretation of data; the writing of the report; or in the decision to submit the article for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Joint Research Ethics Committee of NHS Grampian and the University of Aberdeen, the Tayside Committee on Medical Research Ethics, and the Nottingham Research Ethics Committee.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement Applications for access to unpublished, anonymised data should be made to the TOMBOLA Group, via the PI Professor Margaret Cruickshank.
Linked Articles
- Highlights from this issue