Article Text

Statistics from Altmetric.com
- education and training
- family planning service provision
- general practice
- health education
- service delivery
At different stages in their lives, most women and men alternate between wishing to prevent pregnancy (requiring contraception) and planning/preparing to become pregnant (requiring preconception care), with various levels of ambiguity in between. However, the assessment of pregnancy intentions is not a routine part of sexual and reproductive health (SRH) services, meaning that services are, at best, reactive to these needs. Furthermore, as contraceptive services, preconception care and maternity services are not integrated there are missed opportunities for their provision. For example, a woman attending an SRH service for removal of her intrauterine device should be counselled on preconception health issues, including folic acid, if she intends to become pregnant, but our experience is that this rarely happens.
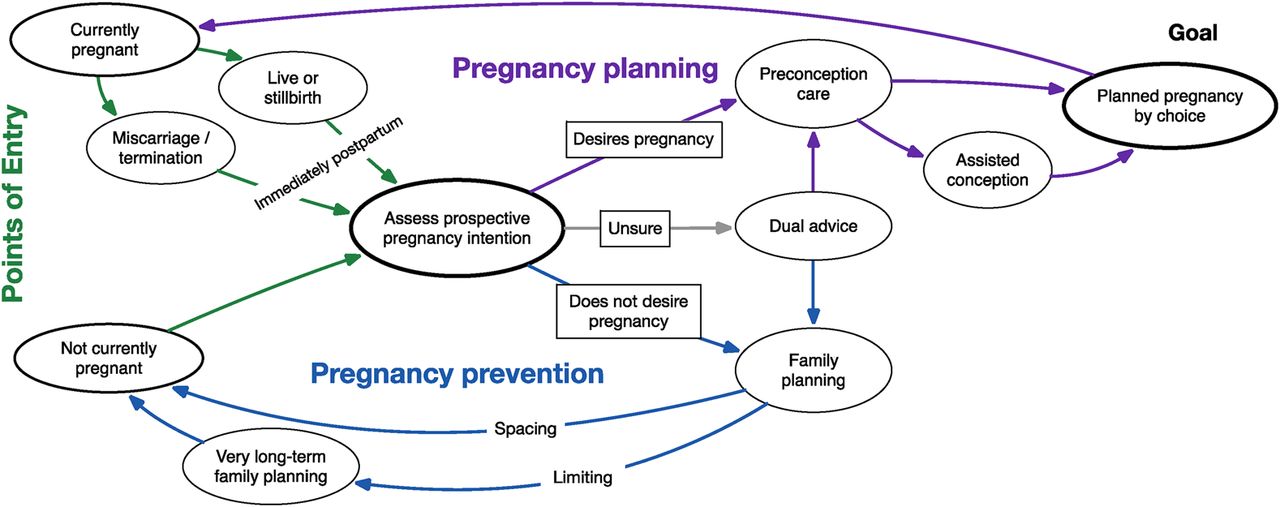
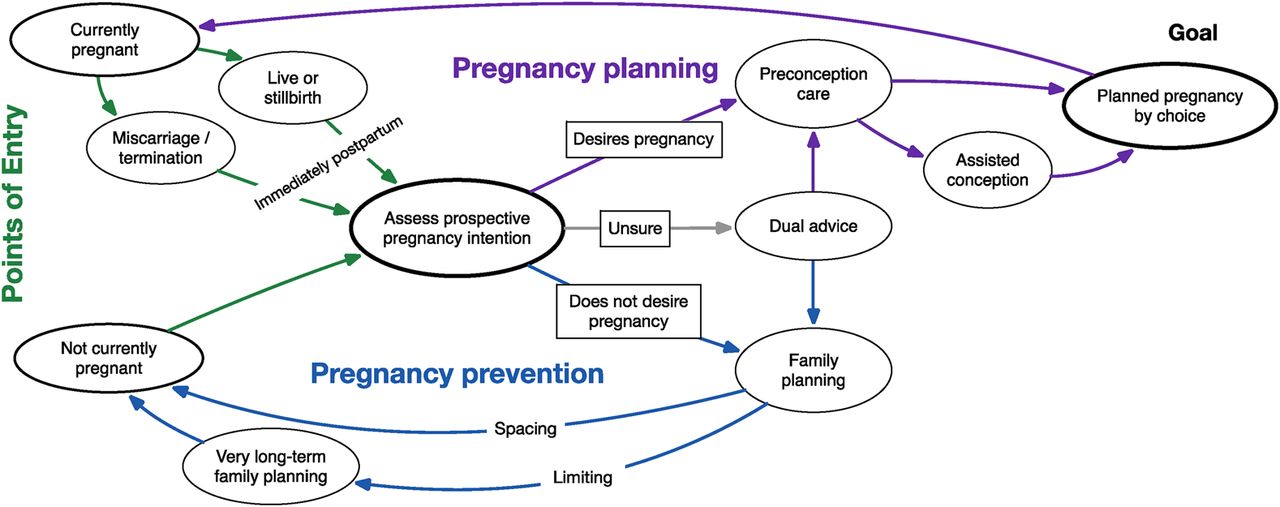
To fill this gap and facilitate an integrated and proactive approach to the pregnancy-related aspects of the reproductive life-course,1 we propose a conceptual framework for ‘Pregnancy Planning and Prevention’ (P3) (Figure 1). This describes the pregnancy-related reproductive needs of women and their partners, can be integrated into current care protocols, is easily applied to subpopulations, such as those with pre-existing conditions (e.g. diabetes, obesity, HIV) that may affect their fertility or pregnancy outcome, and is equally applicable in high- and low-resource settings, regardless of fertility rate.
{kind=link}
Conceptual framework for ‘Pregnancy Planning and Prevention’ (P3).
The goal of this framework is to support individuals to have children by choice, not by chance, thereby improving pregnancy outcomes and achieving desired fertility. To deliver this, women (and men) should be asked about their short-term pregnancy intentions. A robust measure of prospective pregnancy intention is needed; several tools have been proposed2 ,3 but none are psychometrically validated.4 Once such a tool exists it could be used at any health service contact (e.g. primary care, SRH services, postnatal care) and women (and men) could be given ‘pregnancy prevention’ (contraception) or ‘pregnancy planning’ (preconception care) advice/services.
The P3 framework can be applied at individual level (e.g. assessing pregnancy intention in non-pregnant women), at service level (e.g. to map current service provision, identify gaps and design more integrated, holistic services) and at policy level (e.g. ensuring preconception care is provided in primary and specialist healthcare and other settings, such as schools or community groups, where preparation for parenting could be included). The desired outcome is support for women and their partners to assess, articulate and actualise their reproductive health intentions, thereby reducing unplanned pregnancies, improving pregnancy outcomes, and potentially reducing chronic diseases in the long term.
Footnotes
* Corresponding author
Competing interests None declared.