Article Text

Abstract
Background Etonogestrel (ENG) implants (Implanon®/Nexplanon®/Implanon NXT®) are employed as contraception in early postpartum patients. Follow-up is often not conducted by the hospital prescriber. Little is known about duration of lochia, in a modern setting, and even less is known about the effect of ENG implants on lochia.
Aims To determine if early postpartum (pre-discharge) insertion of Implanon for contraception was associated with a significant difference in duration of lochia. To record the number of patients who went on to have their Implanon removed during the study period and the reasons for removal.
Methods Prospective cohort study of 152 postpartum patients from a tertiary maternity unit in Hobart, Tasmania, Australia. The treatment group was women requesting Implanon prior to discharge. Controls were recruited from the same unit over the same time period, with the aim to match for birth weight and parity. Information was collected during face-to-face interviews or via telephone contact. Multivariate survival analysis was used to investigate lochia duration.
Results There were 73 controls and 79 women who had early postpartum Implanon inserted. Fourteen (17.7%) patients in the treatment group had their Implanon removed during the postpartum study period. In all of these cases the reason for removal was bleeding disturbance – prolonged or intermittent vaginal bleeding beyond 50 days postpartum. There was no significant difference in duration of lochia between the groups [median predicted duration 25 days (95% CI 22–27) in controls and 24 days (95% CI 21–26) in the treatment group].
Conclusions Early postpartum insertion of Implanon for contraception was not associated with a statistically or clinically significant difference in duration of lochia.
- long-acting reversible contraception
- implants
- Implanon
- postpartum
- lochia
Statistics from Altmetric.com
Key message points
Early postpartum use of etonogestrel (ENG) implants does not appear to alter the duration of lochia.
In this setting the average duration of lochia was 3–4 weeks, regardless of the chosen contraception.
In this study the ENG implant was more popular in younger women who had used it before, and in women who had reported a previous unplanned pregnancy.
Providing access to immediate postpartum ENG subdermal implants is an important opportunity to prevent unplanned pregnancy.
Introduction
Routine postpartum inpatient care includes counselling about contraception, including available options. Prior to discharge from place of delivery is an ideal time to prescribe and administer contraception. The hospital setting is convenient for both doctor and patient, and the patient is often highly motivated to use contraception having recently delivered a child.
Implanon® is a rod-like implant designed for subdermal insertion and is a long-acting reversible contraceptive (LARC). Each implant contains 68 mg etonogestrel (ENG), which is released at very low rates of 25–70 μg per day depending on the time in situ. Implanon NXT® (Nexplanon® in the UK) is radio-opaque via the addition of barium sulphate to the core of the device. Implanon NXT and Nexplanon have replaced Implanon in Australia and the UK; due to the timing of this substitution both devices were used in this trial. For ease of reporting the term Implanon, when used in this article, refers to both Australian products.1 ,2
Studies show low rates of LARC use in Australia, with only 1.2% of women in a representative study population using Implanon.3 A recent Australian study showed low rates of use of Implanon specifically, with a reported use of 4.9 per 100 contraception problems managed in a general practice setting.4 Clinical guidelines in the UK state that Implanon can be used “at any time postpartum”.5 There are no Australian guidelines regarding the use of LARC in general or Implanon specifically in the early postpartum period.
At the Royal Hobart Hospital (RHH) this method of contraception has been offered to postpartum patients prior to discharge for the past 7 years, with increasing popularity. The trend towards increased use of LARC, especially in younger women, has been supported by published data.4 ,6 Studies also show a reduction in repeat pregnancy in adolescents with the immediate postpartum use of Implanon.7 ,8 Despite routine use, there is no scheduled follow-up of these patients after discharge as patients are encouraged to visit their general practitioner (GP) for this to be undertaken. Few data are available to support the efficacy, side effects and long-term acceptability for these patients. In particular, there are no known studies showing the effects of Implanon on postpartum bleeding/vaginal discharge patterns (lochia).
Lochia is historically divided into three phases: lochia rubra, serosa and alba. These phases refer to the colour of loss, explained in a previous study as red (lochia rubra), brown-pink (lochia serosa) or yellow-white (lochia alba).9 The origins of this classification remain obscure.
Despite being a normal physiological process, there is a dearth of published modern data regarding the duration of lochia and factors that affect this. Textbook descriptions of the total duration of lochia have varied greatly over time from 18 days in 187610 to 8 weeks in 2010.11 One recently published systematic review of lochia patterns included eight studies published between 1970 and 2010, which included tests of significance, where the mean duration of lochia ranged between 24 and 36 days.12 One of these studies, where data from 236 patients were analysed, found a significant relationship between duration of lochia and parity, with increasing parity significantly related to decreased median duration of lochia (p<0.05).9 Two studies found a correlation between increased infant birth weight and increased median duration of lochia (p<0.05).9 ,13 The following factors have also been studied in relation to duration of lochia and found to have no impact: maternal weight, oral contraception use postpartum, smoking habit, maternal age, gestational age at delivery, infant sex, mode of delivery, method of infant feeding, weight of placenta, previous Caesarean section, induction of labour, use of oxytocic agent immediately after delivery, ethnic origin, duration of normal menses, and resumption of sexual intercourse postpartum.12
The main physiological effect of Implanon is inhibition of ovulation. It is a highly effective form of contraception with an estimated method failure rate in Australia of 1.25 per 1000 women per year.14 Progestogen-only contraceptives are a suitable alternative when estrogens are contraindicated, such as in breastfeeding mothers. Implanon has been approved for use in Australia by breastfeeding mothers since 2007.1 Implanon exerts complex effects on the endometrium both directly and indirectly. Direct effects occur via activation of progestogen target sites on endometrial cells. Indirect effects occur through suppression of the hypothalamic-pituitary-ovarian axis. Current research is concentrating on the potential of progestogens to modify endometrial vascular, androgenic, steroid receptor and proto-oncogene function. These processes may be involved in the development of progestogen-induced abnormal bleeding.15
The primary aim of this study was to conduct a prospective cohort study to evaluate the effect of early postpartum Implanon use on duration of lochia. The null hypothesis was that early postpartum Implanon use did not have a significant impact on the duration of lochia, hence reassuring women that it did not have a harmful effect on this physiological process. The secondary aim was to record the number of patients who went on to have their Implanon removed during the first 2 months postpartum and the reasons for removal.
Methods
Study design and setting
The study was undertaken at the Queen Alexandra Maternity Unit, RHH, in Hobart, Tasmania. The RHH is Tasmania's primary tertiary teaching hospital with approximately 2000 deliveries each year. At the time of the study approximately five Implanon devices were inserted in inpatients each week, upon patient request. For the purpose of this study, early postpartum insertion was defined as insertion within 7 days of delivery.
Recruitment
Any postpartum patient requesting Implanon insertion prior to discharge during the recruitment period was invited to participate in the study. Doctors within the Department of Obstetrics & Gynaecology at the RHH, who are accredited to insert the Implanon device, were able to recruit women into the study at the time of implant insertion. Control participants were recruited by the study authors during the same weeks with an aim to match for birth weight and parity. All recruitment was done at the bedside by face-to-face meetings with inpatients. Prior to contact with any inpatients the midwives in charge of the postnatal unit were consulted and gave permission, where appropriate, for the researchers to approach each patient. This review of inpatients suitable for inclusion in the study was conducted at midwifery morning handover. Participants were provided with written information describing the nature of the study and ongoing participation requirements by their midwife in advance of the recruitment meeting, where possible. Written informed consent was obtained prior to recruitment.
Only women who could speak English and who were able to be contacted via telephone were recruited. Any patient who had a mid-trimester delivery, manual removal of placenta, multiple birth, or who was prescribed low molecular weight heparins (LMWH) for more than 7 days postpartum was excluded from the study. All women who were diagnosed with retained products of conception or endometritis requiring antibiotic treatment were also excluded. Contraception use during the postpartum period in the control group was recorded. Patients who used depot medroxyprogesterone acetate (DMPA) prior to the cessation of lochia were also excluded.
Data collection
Consenting women were interviewed by the researchers either at the time of enrolment or by telephone after discharge from hospital, for completion of an initial profile of relevant health and personal data. These interviews were augmented by the patients’ medical records and the Tasmanian statewide obstetric database (ObstetrixTas). Details collected are listed, with comparisons between groups, in Table 1.
Characteristics of 152 study participants at entry to the study
A series of follow-up interviews was undertaken by telephone starting fortnightly, then increasing to weekly, finishing at least a week after reported cessation of lochia. No specific details were recorded about the patient's perceived quantity or quality of lochia. The patient was simply asked if bleeding had stopped. Reasons for removal of implants during follow-up were recorded. Any treatments prescribed for bleeding or clotting disorders (including endometritis) were also recorded. Internal validity was tested by repeating a question about previous contraception failure during both the initial and final interviews. Interviewers were not blinded at initial or subsequent interviews.
Statistical analysis
Data were imported into Stata V.13™ (StataCorp LP, College Station, TX, USA). Descriptive statistics were run to investigate the data. Pearson's Chi-square (χ2) and Fisher's exact tests were used to investigate categorical variables between the control and intervention groups. Independent t-tests and Mann–Whitney U-tests were used to investigate continuous data.
Prior to conducting the analysis of lochia duration in the control and treatment groups, 14 women who had their Implanon removed were excluded. The reason for this was two-fold. The most common side effect of Implanon in any setting is prolonged bleeding/spotting. Given that lochia and the most common Implanon side effect are very similar physiological processes, unfortunately it is impossible to ascertain which vaginal loss is related to lochia and which relates to a side effect of Implanon.A second reason is that progestogen (Implanon) removal will always cause a ‘withdrawal’ bleed and this cannot be classified as lochia.
Scatterplots and Pearson correlation coefficients were utilised to investigate the relationship between lochia duration and age, gestation and birth weight, while a scatterplot and Spearman's rank-order correlation was used to investigate the relationship between lochia duration and body mass index (BMI) and parity. Variables described in the literature as being associated with lochia duration, or theoretically associated (e.g. mode of delivery, breastfeeding, smoking status), were entered into separate univariate survival models. The Wilcoxon Breslow test was used to assess equality of lochia duration survivor functions. Variables significantly associated with lochia duration in univariate analyses were included as covariates in a Weibull Accelerated Failure Time (AFT) survival model of lochia duration in the control and treatment groups. Previous Implanon was included as a covariate in the model as it was theorised that repeat users were unlikely to have experienced significant side effects with use. A Weibull (AFT) model was used rather than a Cox proportional model as preliminary modelling indicated the proportional hazards assumption was violated. Akaike's16 Information Criterion was used to validate selection of the model.
Results
Recruitment was undertaken during two time periods (October 2011–January 2012 and January–May 2013). Approximately 750 deliveries occurred during these periods. All women who were approached agreed to participate. In the Implanon group 89 patients provided consent. Of these three were deemed not eligible: two for endometritis and one for therapeutic LMWH use for 6 weeks postpartum. Of the 87 recruited patients in the control group seven were not eligible: five for endometritis, and one each for retained products and DMPA use. Seven controls and seven Implanon group women provided consent to participate but were discharged from hospital prior to baseline interview.
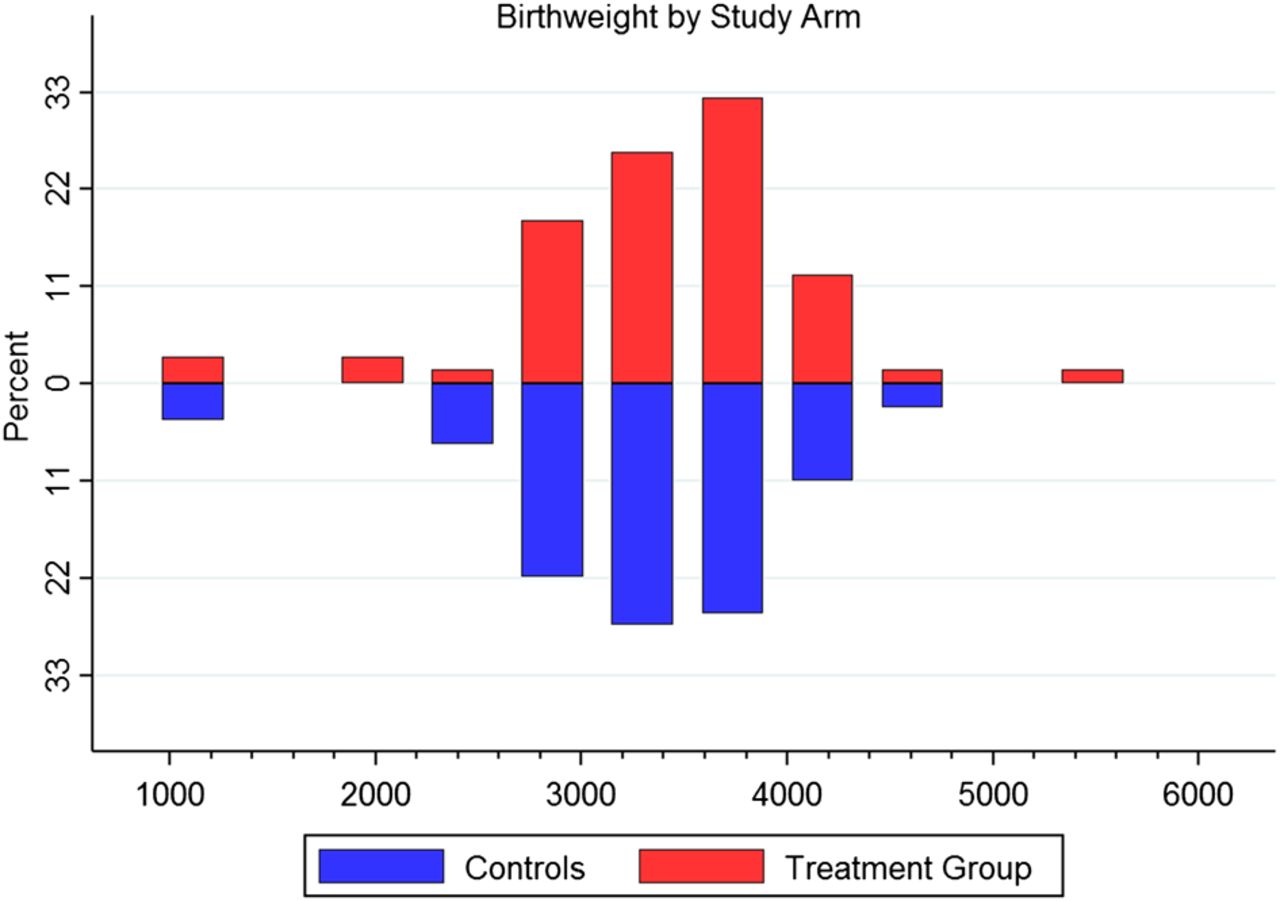
Comparison of control (n=73) and Implanon (n=79) groups is shown in Table 1. Groups were well matched for parity, birth weight, BMI, mode of delivery, smoking status, gestation at delivery, breastfeeding and postpartum haemorrhage (PPH) rates (see Figure 1 for birth weights for each group). However, control women were slightly older (28 vs 25 years, t(150)=3.23, p=0.002) and treatment group women were more likely to have used Implanon previously (41.8% vs 20.5%, χ2(1)=7.9, p=0.005).

Frequency versus birth weight for treatment and control groups.
Fourteen (17.7%) treatment group patients elected to have their Implanon removed. In all these patients the duration of bleeding was reported to have continued for over 50 days. In 6/14 patients the irregular bleeding/vaginal discharge pattern did not resolve within 14 days of Implanon removal. There was also one patient in the control group whose lochia continued for over 50 days (54 days). There were no statistically significant differences between the Implanon removed and Implanon continued groups, largely due to the small sample size of the Implanon removed group. However, there was a trend for women who had Caesareans and breastfed their babies to continue with Implanon, while a larger (but not statistically significant) proportion of women who had Implanon removed were smokers.
Univariate analysis of lochia duration
After excluding the 14 women who had Implanon removed, there were 138 women (73 controls and 65 treatment group) in the univariate survival analysis. This resulted in a total of 3423 days to event (cessation of lochia) included in the analysis. A preliminary Kaplan–Meier plot and Wilcoxon Breslow test demonstrated no significant difference between controls and the Implanon group for lochia duration survivor functions (p=0.54). Furthermore, the Kaplan–Meier plot (Figure 2) illustrates no significant difference in the overall proportion of women with lochia over time. The survival model of lochia duration and mode of delivery demonstrated significantly shorter lochia duration among women who had a normal vaginal delivery compared to Caesarean section [median 23 days, 95% confidence interval (95% CI) 21–26 vs 28 days, 95% CI 24–36, p=0.017]. No other variables investigated in univariate analyses were significantly associated with lochia duration.

{kind=link}
{kind=link}
Kaplan–Meier plot of survival for duration of lochia.
Multivariate analysis of lochia duration in the control and treatment groups
The multivariate Weibull AFT regression included mode of delivery and previous Implanon as covariates. The model indicated that the ratio of estimated median lochia duration was not significant for women who had Caesarean deliveries versus normal vaginal deliveries (time ratio 1.12, 95% CI 1.01–1.32) or for the previous Implanon group compared to the Implanon naïve group (time ratio 0.93, 95% CI 0.81–1.07). The ratio of estimated median lochia duration for the intervention group compared to controls (time ratio 0.98, 95% CI 0.86–1.16) was also not significant. Median lochia duration predicted from the model was 25 days (95% CI 22–27) for the control group and 24 days (95% CI 21–26) for intervention group. Overall, the multivariate Weibull AFT regression model was not significant (p=0.27).
Discussion
We found that early postpartum insertion of Implanon for contraception was not associated with a statistically (or clinically) significant change in duration of lochia. In our groups the average durations of lochia were 25 and 24 days, which corresponds well with recently published data on this topic.12
The trend towards shorter duration of lochia among women who had a vaginal delivery compared to Caesarean section has not been shown in other studies. This is possibly a result of modern obstetric practice, given that historically there were not large numbers of patients undergoing Caesarean delivery, and there has not been a great deal of research regarding lochia in the past decade. It must be noted that our study was not designed to assess this outcome. This is certainly an area for further research.
Strengths and weaknesses
A selection bias may have occurred at enrolment given that all participants approached had been pre-screened for suitability by the midwives in charge of their care. Also, some women who provided consent to participate were discharged from hospital prior to interview. This probably led to a reduced number of patients lost to follow-up as the researchers did not approach any patient whom the midwife deemed to be unreliable and/or uninterested. Given this process of midwife-led pre-screening for recruitment, the true number of eligible women who delivered during the recruitment periods is unknown. However, it is likely that the study population represents a true reflection of the type of patient delivering in our unit given that the two groups were consented at random and were well matched for birth weight, parity and BMI.
The definition of cessation of lochia was sometimes queried by the participant during the telephone interview. The main confusion regarding this was in patients who noted lochia alba and quite rightly stated that their ‘bleeding’ had stopped, but they were still using sanitary items for ongoing postpartum vaginal loss. If questioned, the researcher's consistent reply was to record from the last day that sanitary items were required for postpartum vaginal discharge of any kind. Previous studies on lochia report that approximately one-third of patients do not experience lochia alba.9 As the same researcher performed all follow-up telephone interviews, the potential for inconsistently interpreted lochia duration, and resulting misclassification bias, was reduced. A written or diagrammatic explanation about lochia and Implanon-related vaginal discharge could have been useful for participants in this study. The study team did, however, feel that this might be cumbersome for the mothers of newborns. As this may have resulted in a higher number of women refusing to participate, this option was not employed. A strength of this study was the consistency of interviewer for all participants.
This study required accurate recall regarding cessation of lochia by the patient. In an effort to avoid forgetfulness, patients were contacted on a weekly basis (after the first fortnight). However, not all patients were successfully contacted each week, and on occasion it was over 2 weeks after cessation of lochia that telephone contact could be made and data collected. This may have resulted in some degree of recall bias.
Many study participants no longer used fixed-line telephones at home. Whilst the use of patients’ mobile telephones as a point of contact may have been more reliable at times, allowing the researcher to contact patients when they were not home, it created difficulties with follow-up in circumstances where the mobile number provided had been disconnected or was consistently unanswered. In an effort to increase pickup rates the researcher chose to display her contact phone number. This may have led to a substantially higher number of participants answering calls.
LARC and abnormal bleeding
Eighteen percent of patients in the treatment group had their Implanon removed during the study period for prolonged (continuous or intermittent) bleeding. In some but not all cases, the patient's GP organised a pelvic ultrasound and/or prescribed antibiotics prior to removing the Implanon.
Abnormal bleeding patterns are common in women using LARC. When recorded over a longer time frame than the postpartum period (2 years post-insertion), frequent or prolonged bleeding occurs in fewer than 10% of patients at any time.17
Limited data are available relating to the treatment of abnormal bleeding patterns in Implanon users. A promising pilot study was published by Weisberg et al. in 2006,18 which showed efficacy of either mifepristone in combination with ethinylestradiol (EE) or doxycycline alone. Current National Institute of Health and Care Excellence (NICE) guidelines5 suggest treatment with either mefenamic acid or EE; however, the specifics for prescribing are not provided.
Menstrual disruption is the main reason for discontinuation of use of LARC. Many studies have shown that early discontinuation of implant use is primarily due to bleeding problems.14 ,19–21 One study demonstrated that long-term bleeding patterns could be partly predicted by the bleeding pattern experienced during the first 3 months after insertion; however, the study did not include postpartum patients.22 A follow-up study of the present treatment group after many months would be useful to record Implanon continuation rates and reasons for removal.
A study by Gezginc et al.23 using Implanon included 25 postpartum patients out of a total of 80 participants. In these women, insertion occurred during menses and “at least 6 weeks after … delivery”. In this study Implanon was removed from 20 (25%) patients, a similar proportion to our study, with frequent/prolonged bleeding being the most common reason for removal. No specific data were provided about the postpartum subgroup of participants.
A recently published trial by Tocce et al.,7 in which the majority of patients had early postpartum Implanon inserted, gave much higher continuation rates (e.g. 96.9% at 6 months). This very high continuation rate may be attributed to the comprehensive, multidisciplinary, adolescent-orientated ‘Colorado Adolescent Maternity Program (CAMP)’ that the patients were enrolled in concurrently, which was aimed at preventing repeat unwanted adolescent pregnancies.
Implanon and breastfeeding
In the present study over 50% of the participants were breastfeeding their infants. Studies performed to assess milk quality and quantity as well as infant growth and development using progestogen implants as contraception have been performed.24 ,25 These studies do not show any deleterious effects; however, in these studies patients were recruited from 4 weeks postpartum. More recently a study of breastfeeding outcomes has been published that showed no difference in women who had early (Day 1–3) versus standard (4–8 weeks postpartum) Implanon insertion.26 There are no published studies regarding this aspect of implant use since the addition of barium to the Implanon NXT/Nexplanon device.
Implanon, adolescents and unwanted pregnancy
In our study patients requesting early postpartum Implanon for contraception were significantly younger. This tendency for younger women to use this type of contraception has been supported by other recently published research.4
Our study showed an overall reported unplanned previous pregnancy rate of 58%, which correlates well with published data estimating that over 50% of women in Australia have had an unplanned pregnancy.27 Early postpartum Implanon use is gaining increasing recognition as an important and often missed opportunity to avoid repeat unplanned pregnancy. Its success at doing this in adolescent mothers has been shown in prospective observational studies.5 ,6
Conclusions
Early postpartum Implanon administration does not appear to alter the duration of lochia. As use of Implanon in the early postpartum period becomes more widespread, further research is needed to assess the risks and benefits of this method for mothers and for breastfed babies.
Acknowledgments
The authors would like to thank the RHH Queen Alexandra Maternity (QAM) midwifery staff for their assistance with recruitment of participants. They would particularly like to thank Ms Becky French, RM, QAM Unit Staff Co-ordinator at the time of implementation of this study for her valuable support. They would also like to thank the RANZCOG Research Foundation for their grant which funded this study.
References
Footnotes
Funding This was a prospective cohort study in which all information collected after discharge was done via telephone by Kim Dobromilsky. A RANZCOG Research Foundation grant to the value of $500 was received and used predominantly towards the cost of these telephone calls.
Competing interests Kim Dobromilsky has been educated as an Implanon® insertion and removal trainer; she has received funding from the manufacturer in the past for her participation in these training sessions (2008–2011).
Ethics approval Human Research Ethics Committee (Tasmania) Network, reference number H0012037.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue