Article Text

Abstract
Migraine is a common headache disorder, particularly in women. It usually starts during the teens and twenties, a time when many women are seeking contraception advice. Migraine without aura is the most prevalent type of migraine, affecting up to 70% of people with migraine, while the remainder experience attacks with and/or without aura. Aura is a phase of focal neurological symptoms, typically visual. An increasing body of evidence identifies aura as a marker of increased risk of ischaemic stroke and its presence is a contraindication to the use of combined hormonal contraception (CHC). However, aura is often confused with more generalised premonitory visual symptoms of migraine that may precede attacks of migraine with and without aura, which are not associated with stroke risk. Diagnostic confidence is needed so that CHC is not withheld unnecessarily.
- aura
- headache
- migraine with aura
- migraine without aura
- contraception
Statistics from Altmetric.com
Key message points
Onset of migraine is usually during the teens and twenties, and so may occur coincidently with starting contraception.
ID-Migraine™ is a screening tool for the three best predictors for diagnosing migraine without aura: photophobia, disability and nausea.
The visual aura rating scale screens for the specific visual symptoms of migraine aura, which is a contraindication to the use of combined hormonal contraception.
Introduction
Migraine is the commonest cause of severe episodic recurrent headache, affecting 19% of women and 11% of men worldwide.1 It is recognised by the World Health Organization (WHO) as the sixth leading cause globally of years lived with disability.2
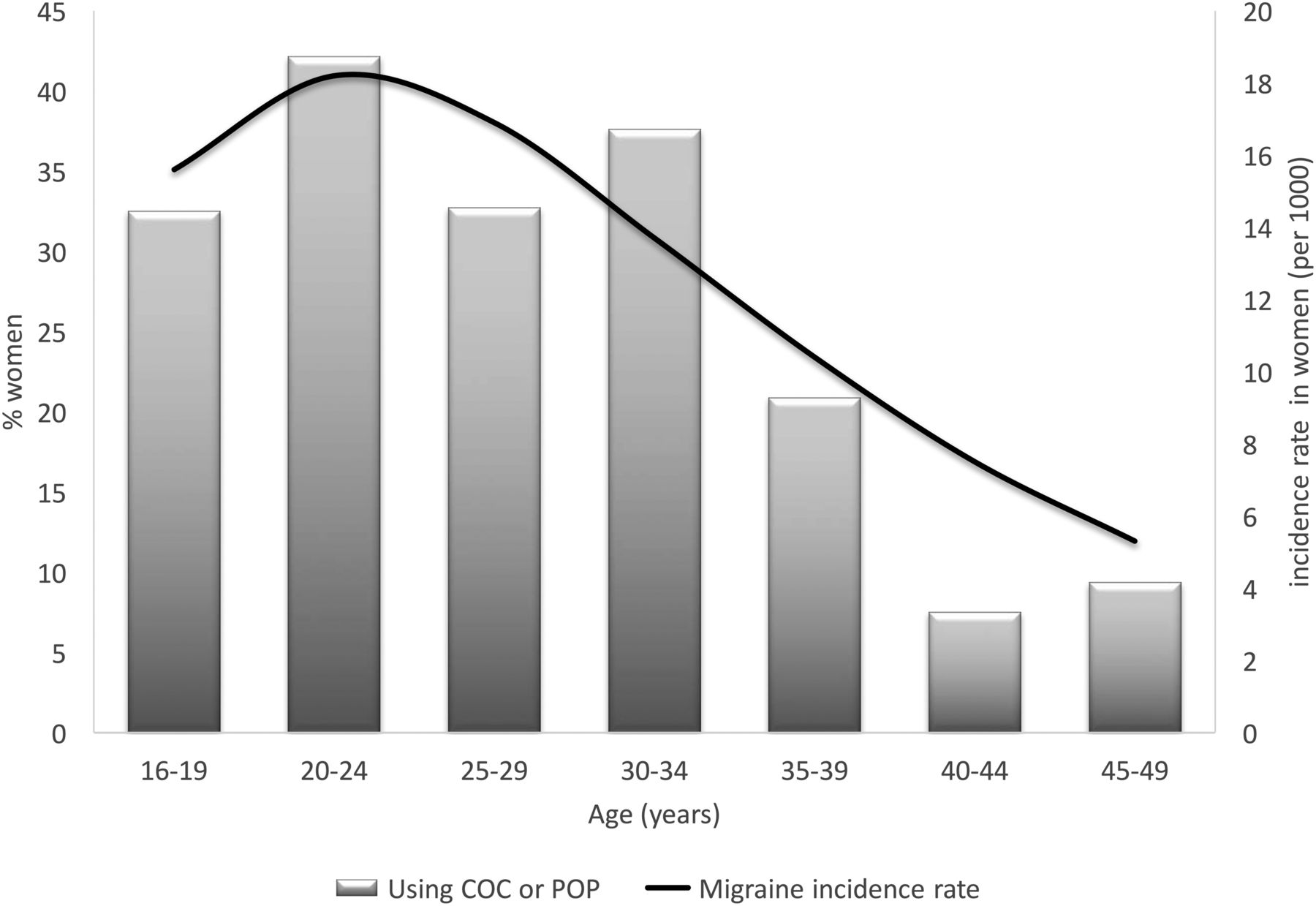
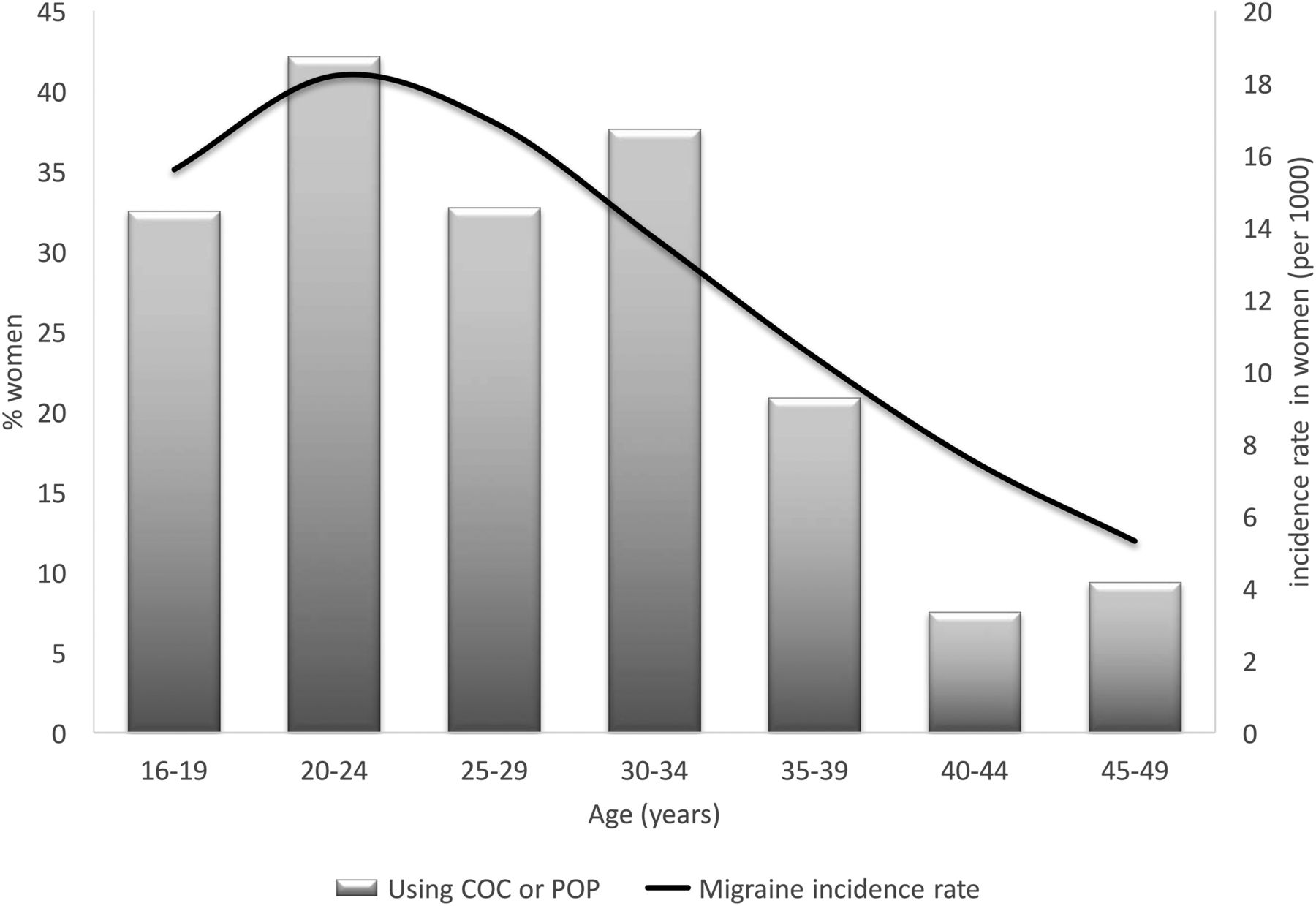
Migraine incidence peaks between the ages of 20–24 years in women and 15–19 years in men,3 with 90% of first attacks occurring before age 40 years.4 In both men and women, peak migraine prevalence is between 30 and 39 years,5 and peak disability is between 35 and 44 years.6
The two most common types of migraine differ only in the presence or absence of an aura. Migraine without aura is most simply defined as disabling episodic headache attacks accompanied by sensitivity to light, nausea, and/or vomiting, lasting up to 72 hours.7 During attacks, activity is limited as it usually worsens the symptoms. In attacks of migraine with aura, the migraine headache is preceded by focal neurological symptoms. In both types of migraine, the person is symptom-free between attacks.
Types of migraine are not mutually exclusive within individuals. About 70% of people with migraine have attacks of migraine without aura (formerly known as common or simple migraine); 20% have migraine with aura (formerly known as classical or focal migraine); and 10% have both types of attack. Less common is migraine aura without headache, which accounts for fewer than 1% of attacks.
The changing hormonal environment in women is considered to be the main reason for the higher prevalence of migraine without aura in women during the reproductive years, with varying improvement or deterioration associated with menstruation, use of hormonal contraception, pregnancy, menopause, and use of hormonal drugs and hormone replacement therapy (HRT). In contrast, the prevalence of migraine with aura increases with age, occurring in around 13% of attacks in people with migraine aged 18–29 years, 20.1% between ages 40–49 years, and 41% by age 70 years or older.8
Around 25% of women living in Great Britain aged 16–49 years use oral contraception, so there is a high likelihood that a proportion of these women will also have migraine (Figure 1).3 ,9 Correct diagnosis of the type of migraine is important since migraine with aura (but not migraine without aura) is associated with a two-fold increased risk of ischaemic stroke.10 ,11 Use of combined oral contraceptives (COCs) is an independent risk factor for ischaemic stroke: odds ratio (OR) 1.56 [95% confidence interval (CI) 1.61–1.89] for COCs containing 20 μg ethinylestradiol and OR 1.75 (95% CI 1.36–1.79) for 30 μg COCs.12 Hence in the UK, USA and WHO Medical Eligibility Criteria, COCs are contraindicated in women with migraine aura.13–15 Progestogen-only methods do not increase risk of ischaemic stroke,12 and may benefit migraine with aura.16 Aura does not restrict use of physiological doses of estradiol in HRT, specifically transdermal estradiol, which is not associated with increased risk of ischaemic stroke.17
While the International Headache Society (IHS) has developed criteria for the diagnosis of migraine,7 these are more suited to research than to clinical practice. The aim of this review article is therefore to provide clinicians with quick and simple tools to diagnose migraine with and without aura.
What is migraine?
Migraine is more prevalent than diabetes, epilepsy and asthma combined. Although migraine is not life-threating in itself, the severity and frequency of attacks can result in significant disability and reduced quality of life, even between attacks.18 ,19
Episodic attacks result from internal and environmental triggers that combine to reach the attack ‘threshold’, which is likely to be genetically determined (Figure 2).20 Crossing the threshold triggers changes in brain chemistry, which gradually resolve over the course of the attack. Prophylactic medication raises the migraine threshold and, depending on the type of medication, can treat some triggers, thus reducing the frequency of attacks; symptomatic treatment can interrupt the process of an attack, but cannot abort it.
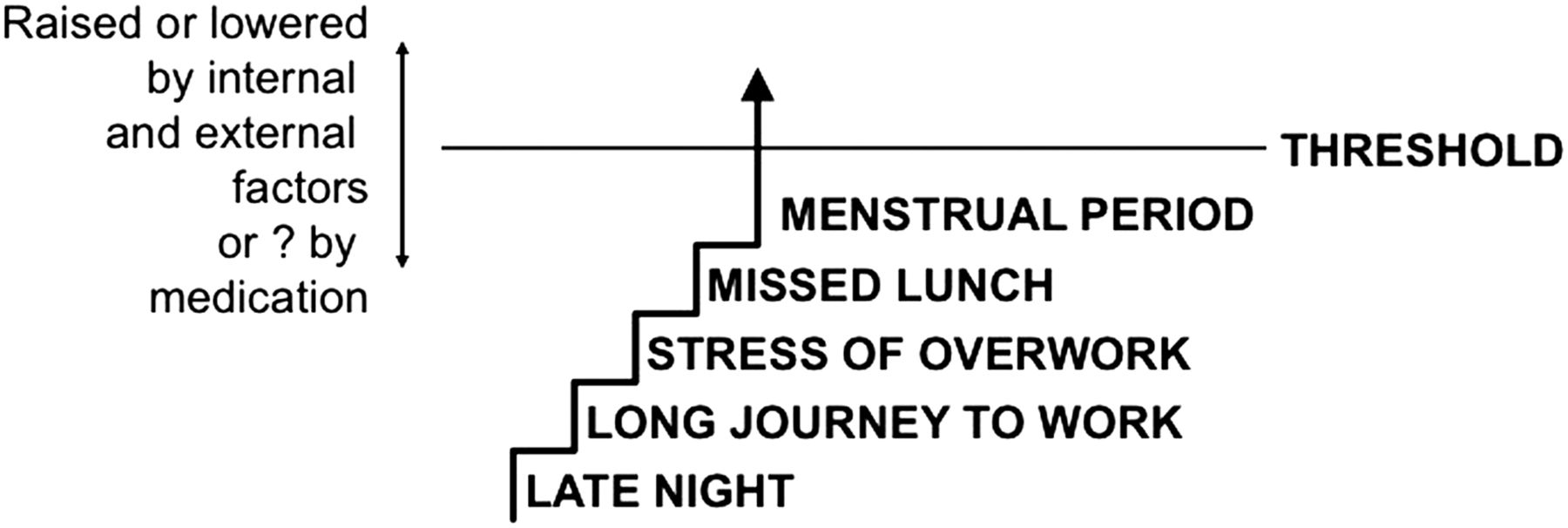
The threshold theory of migraine. Reproduced from MacGregor,20 by permission of SAGE publications.
Clinical phases of a migraine attack
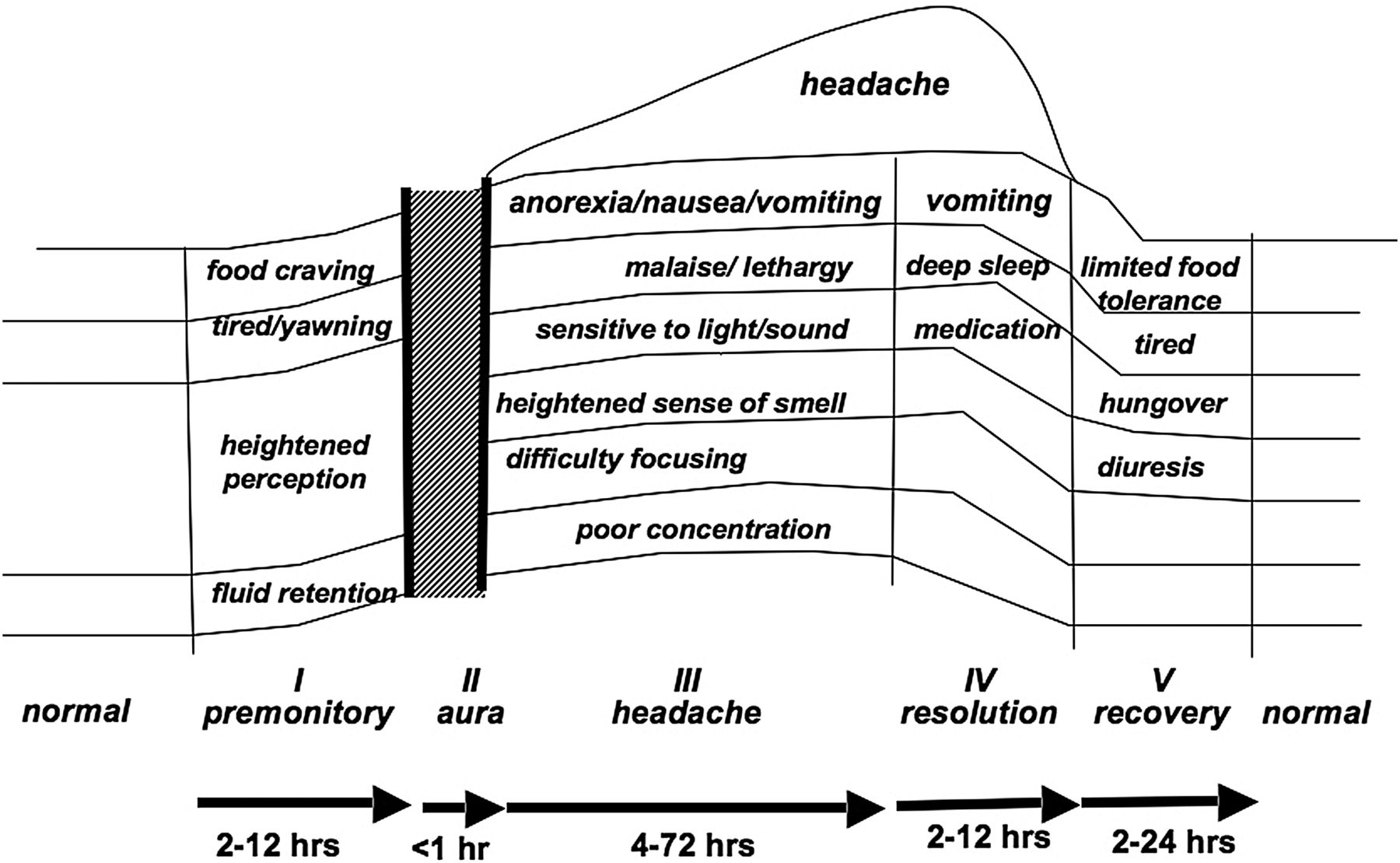
An attack of migraine has five distinct clinical phases (Figure 3).21 The important point to note is that the migraine process is more than just aura and/or headache, but starts and ends with distinct and discrete phases.
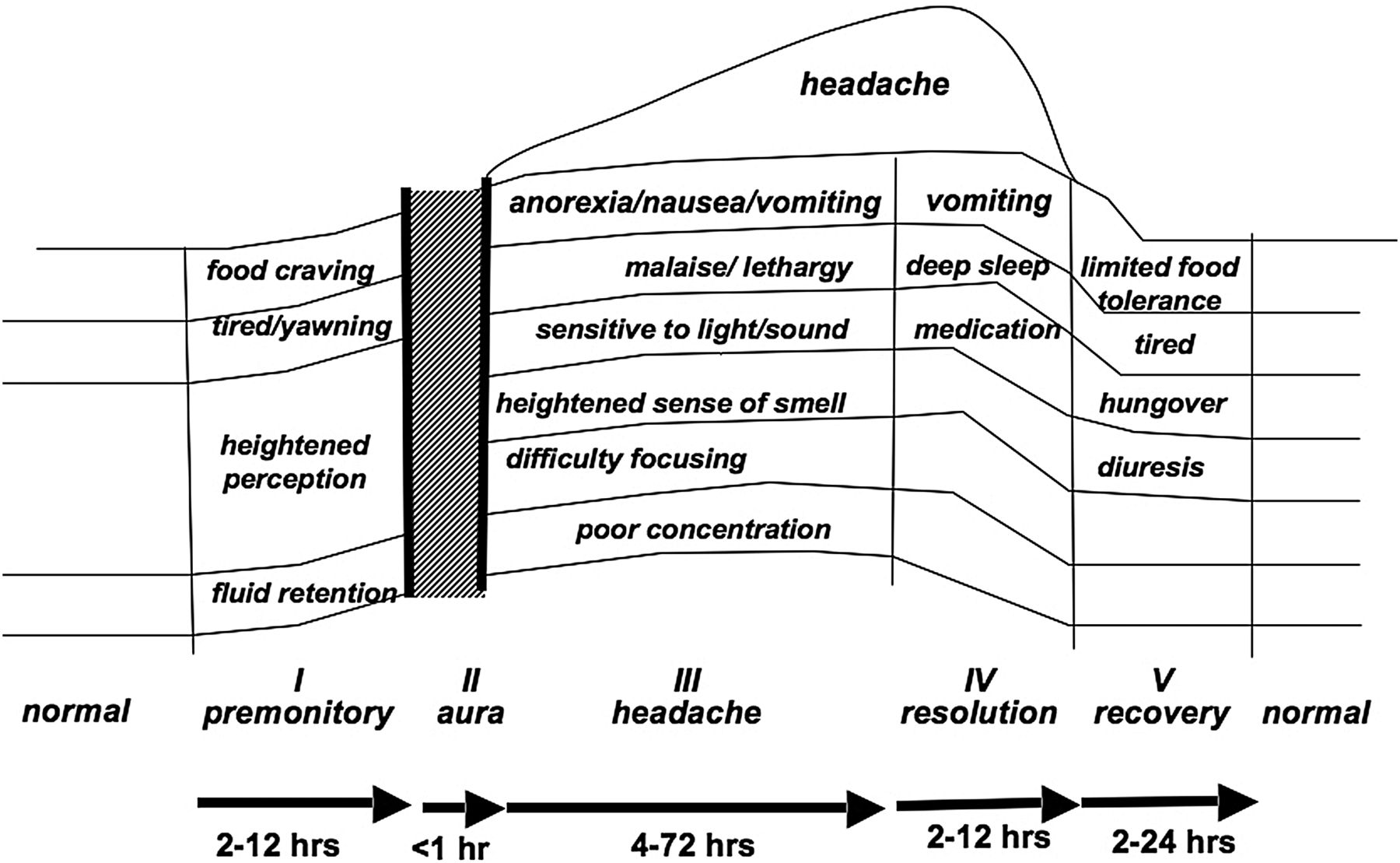
The five stages of a migraine attack. Adapted from Blau,21 by permission of Elsevier.
Premonitory phase
Premonitory symptoms are distinct from, and unrelated to, the aura and can precede attacks of both migraine with and without aura by up to 48 hours.22 They are considered to be due to a transient hypothalamic disturbance.23 ,24 Typical symptoms include unusual tiredness, difficulty concentrating, neck stiffness, yawning, food cravings, blurred vision, and sensitivity to light, sound and smell. These are often mistaken for triggers, rather than symptoms that the attack has already started. In her book Hotel du Lac, Anita Brookner eloquently describes premonitory symptoms which Edith experiences, the night before waking with a migraine headache:“When … she sat down to dinner, she was aware that the lights were brighter, the room more alive with personalities, the tables full … she felt very tired, and thought that she would sleep soundly that night … But sleep did not come easily … When she awoke, rather later than usual, it was with the ancient and deadly foreknowledge that the day would be a write-off. Her broken night had left her with an aching head and an instinctive shrinking from both food and company. Minute noises seemed magnified: a trolley was wheeled vigorously along the corridor, and the high voices of the maids sounded unbearably piercing.”25
Aura
Aura, when present, may follow premonitory symptoms or may start without apparent warning. It is typically characterised by any combination of visual, hemisensory (sensory differences affecting only one side of the body, usually the arm, spreading up from the hand into the face), or language abnormalities, with each symptom developing over at least 5 minutes and lasting a maximum of 60 minutes. Other symptoms that can accompany migraine, such as vertigo or dizziness do not constitute aura.
Although some retrospective studies have suggested that migraine headache may develop during aura, the majority of prospective studies support that migraine headache follows aura.26–30 There may be a gap of several hours between resolution of aura and onset of migraine headache.31
Although there is no definitive proof, the mechanism underlying migraine aura is considered to be cortical spreading depression (CSD), a transient wave of depolarisation spreading across the visual cortex followed by suppression of brain activity.32 The rate of propagation of CSD is approximately 3 mm per minute,33 the same rate at which the clinical symptoms of aura spread.34 Animal models suggest that estrogen increases susceptibility to CSD,35 which might account for increased risk of migraine aura seen clinically during high estrogen states such as pregnancy, use of CHC and estrogen replacement therapy.36
Aura has been vividly depicted in lay and medical literature over centuries and is well defined in this patient description:“I first notice visual symptoms, starting with blind spots varying from perhaps part of a letter missing on a page, looking like a misprint, to somebody's chin missing, or the loss of half my field of vision. This culminates in pulsating zigzag lines around objects giving the impression of the scene being viewed through a shattered mirror. My speech is affected – I can't put a sentence together. I feel confused and disorientated. This is the most distressing part of the migraine attack and it lasts about 15 to 20 minutes. Then my vision restores itself at the same time as a sick, one-sided pain starts in my head.”
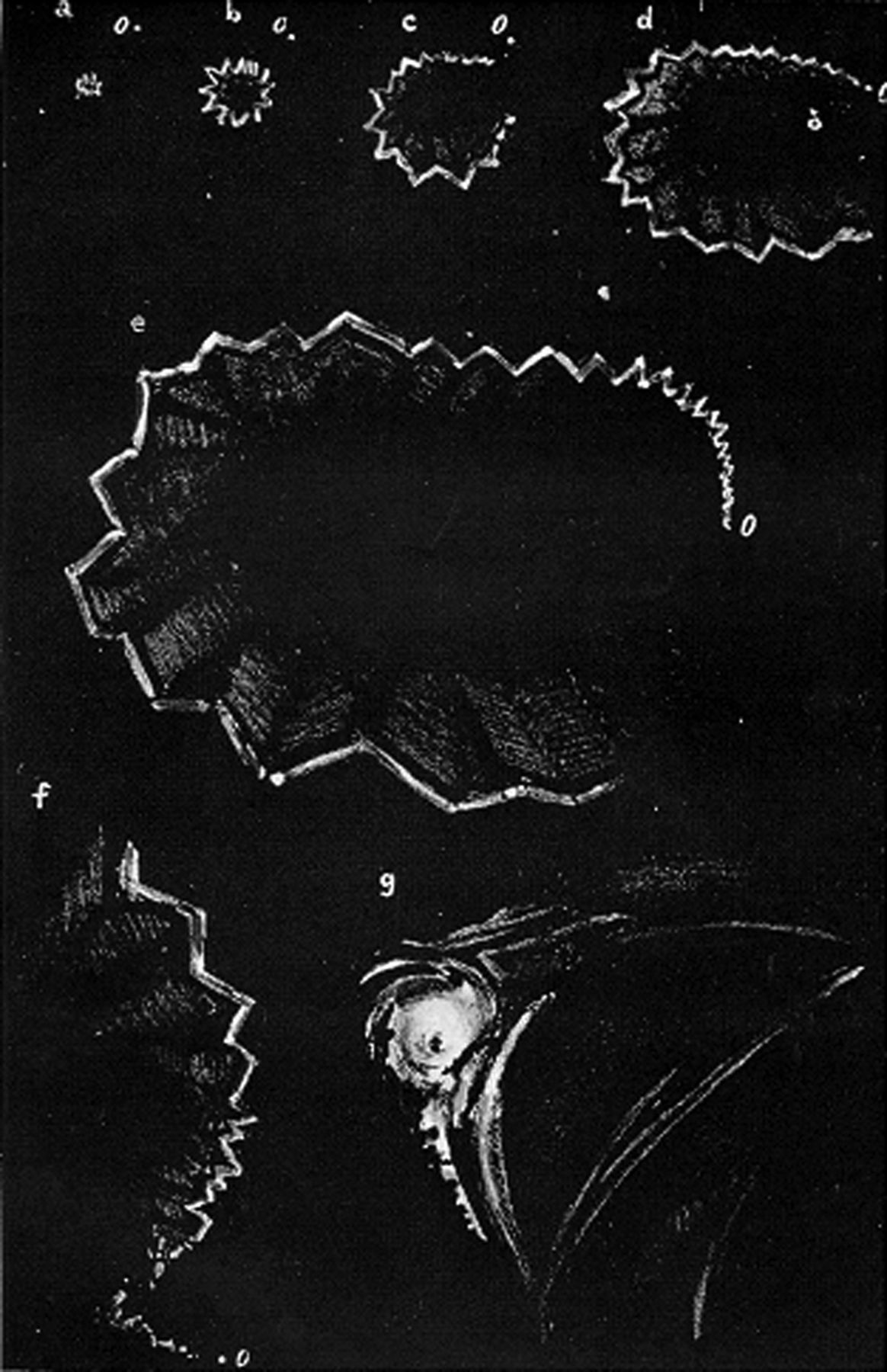
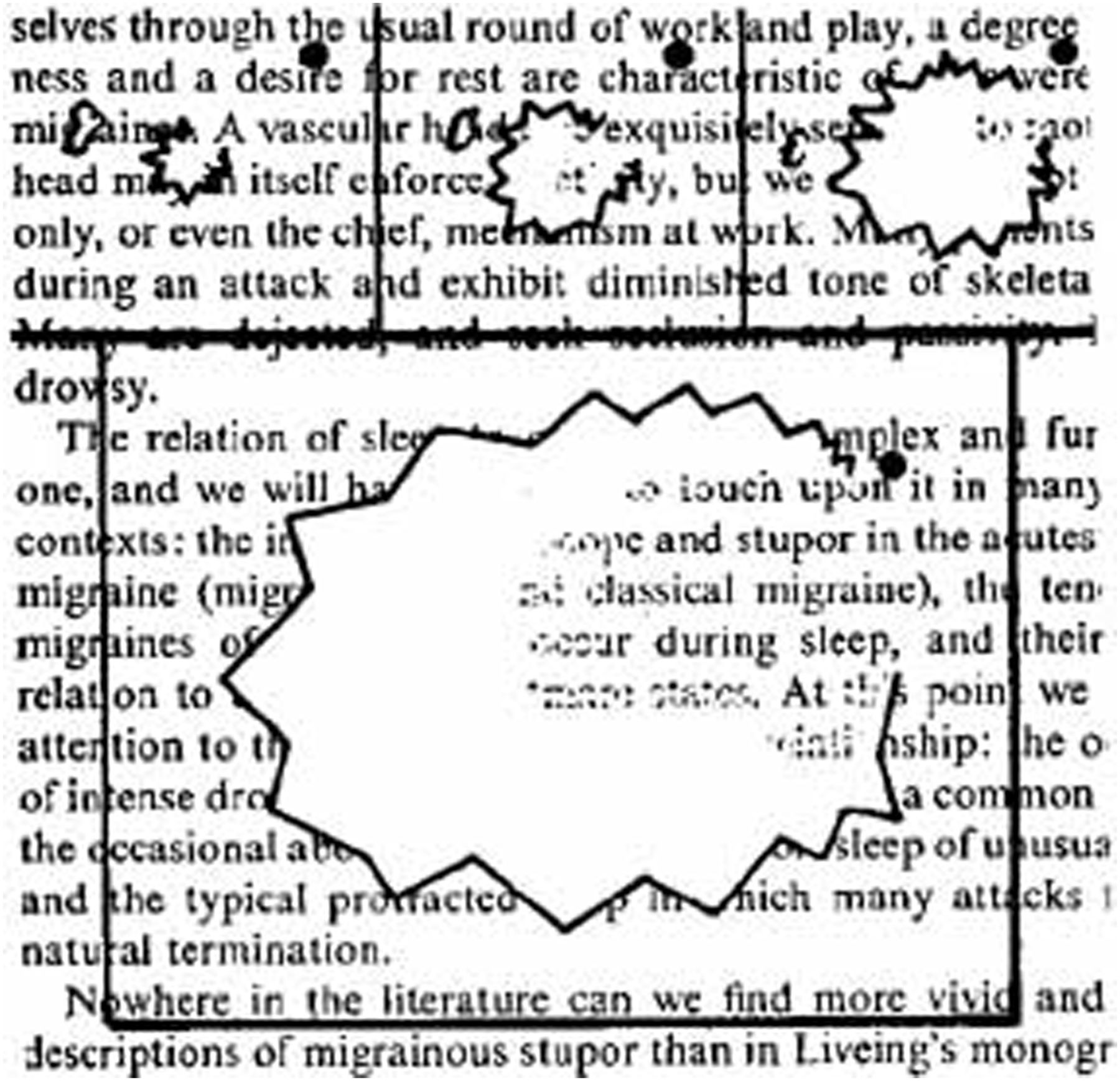
Visual aura is present in over 98% of auras.27 ,30 ,37–40 The classic description is of a scotoma, an enlarging blank spot starting as a small spot and gradually increasing in size, which may be ‘scintillating’ – like the bright flashbulb effect from a camera. The curved margin of the scotoma can appear as zigzags or fortification spectra – a term coined in the late 18th century because the visual disturbances resembled a fortified town surrounded by bastions. In a prospective study of 32 patients with migraine with aura, all patients reported either scintillating scotomas, or fortification spectra, or a combination of both.30 The uniformity of visual aura is evidenced by migraine art over centuries (Figures 4 and 5; further reading/information).41 ,42

Depiction of an expanding scintillating scotoma and fortification spectra (by Sir William Richard Gowers).41
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Depiction of an expanding scintillating scotoma and fortification spectra (by Hubert Airy).42
The aura usually starts at or near the centre of fixation, gradually spreading laterally, expanding at a rate of 3 mm per minute over a period of 5–60 minutes, typically around 20–30 minutes.
You do not need eyes to ‘see’ migraine aura, since it is emanating from the visual cortex, not from the eyes, so it will persist with the eyes closed.43 Visual aura symptoms are ‘seen’ in one half of the visual field in both eyes, although may subjectively be noticed only in one eye. Direct questioning can help elicit bilateral visual symptoms.
Sensory aura is often described as numbness or tingling affecting one arm.39 This sensation often spreads proximally from the hand over several minutes to affect the mouth and tongue, as in the following description:“The first symptom is when my eyes go. Then I get pins and needles in my hand which travels up my arm to my neck and into my mouth causing my tongue to go numb and my speech to be slightly affected. The headache then follows.”
Speech can also be affected during migraine aura, with difficulty finding the correct words, or the wrong words being used like a ‘word salad’. As with sensory symptoms, speech symptoms occur in combination with visual aura.
Aura should not be confused with symptoms of a stroke or transient ischaemic attack (TIA), which affect one side only, start suddenly, and do not have the scintillating and spreading features of migraine aura. In contrast to stroke and TIA, typical migraine aura does not affect the leg and there is no motor weakness.
Headache
Migraine headache is typically unilateral but may be bilateral. It is accompanied by nausea or vomiting, photophobia and/or phonophobia. Activity is limited since headache is aggravated by movement, with a need for bed rest a common feature of severe attacks. As one person describes:“The pain begins at the front of my head and travels all over my head making the back of my head feel very heavy. I have to stay as still as I can otherwise it gets worse. I can't sit in a room with the lights on or the TV as the light affects the strain on my eyes to my head. I feel very sick.”
The pain is assumed to arise from the large cranial blood vessels and the dura mater, which are innervated by the trigeminal nerve. When activated, the trigeminal nerve transmits pain impulses to the trigeminal nucleus caudalis in the brain stem, which relays pain impulses to thalamus and up to the cerebral cortex, where the messages are decoded into the experience of pain.
Resolution and recovery
The headache and accompanying symptoms resolve with time but can be attenuated by sleep and medication. In children, attacks often resolve with vomiting. The ensuing postdromal symptoms during the recovery phase can be as disabling as the headache itself, common symptoms being fatigue, cognitive impairment, and mood changes. A typical description is feeling “wrung through a mangle”.
Diagnosing migraine
Types of migraine are not mutually exclusive and around 30% of people with migraine with aura also have attacks without aura,37 ,40 ,44 with the pattern changing over time. Women often experience a flurry of attacks of migraine with aura around puberty and then only have attacks without aura for many years. In later life, migraine aura without headache is more prevalent as headache becomes less of a feature with advancing age.40 ,44 Most people with attacks of migraine aura without headache have or have had migraine aura with headache.30 ,39
Diagnosing migraine without aura
ID-Migraine™ is a valid and reliable symptom-based screener for migraine without aura that has been developed for use in primary care.45 It is based on the three best predictors for diagnosing migraine without aura, namely photophobia, disability and nausea; patients who report two of these symptoms have an 81% probability of having migraine and three symptoms increases the probability to 93%. A simple acronym for the ID-Migraine questions is ‘PIN’ (Box 1).46
Diagnosing migraine with aura
Since visual aura occurs in isolation or in association with sensory aura or speech disturbance, diagnosis of aura can be made based on the visual symptoms alone.27
Questioning needs to be specific, since visual symptoms occur during each stage of migraine, with blurred vision reported by 28% of people with migraine experiencing premonitory symptoms and 35% during the headache. However, non-aura visual symptoms differ from aura by their lack of gradual development and longer duration. For example, non-aura visual symptoms are often characterised by flickering lights or ‘phosphenes’ lasting less than 5 minutes and which may recur at intervals,47 ,48 or general blurring of vision lasting more than 60 minutes.47 So a report of “Seeing spots of light flashing before my eyes” before and during the headache is not migraine aura.
The question “Have you ever had visual disturbances lasting 5–60 minutes followed by headache?” is a useful screener as studies show that it correctly identified 74% of patients diagnosed with migraine aura by interview and correctly identified 91% of patients who did not have migraine aura.49 However, it is not specific to aura and may over-diagnose aura in a patient with migraine without aura.
A more sensitive and specific tool is the visual aura rating scale (VARS) for migraine aura diagnosis, which is based on the IHS's diagnostic criteria.47 The VARS score is the weighted sum of the presence of five visual symptom characteristics: duration 5–60 min (3 points), develops gradually over at least 5 min (2 points), scotoma (2 points), zig-zag lines (2 points) and unilateral (1 point) (Table 1). A VARS score of ≥5 out of a maximum score of 10 points has a sensitivity of 96% (95% CI 92–99%) and a specificity of 98% (95% CI 95–100%) for migraine aura.
Visual aura rating scale (VARS) score for diagnosis of migraine aura47
Additional tips to confirm the diagnosis of aura are to show patients pictures of aura to assess similarities with their own symptoms. As aura is so specific, a vagueness when describing symptoms makes aura unlikely. Asking patients to draw their symptoms is confirmatory as patients with aura will draw zig-zag lines. Further confirmation is persistence of visual symptoms with the eyes closed.
Diagnosing migraine aura without headache
Aura without headache is more prevalent with increasing age and there is usually a current or past history of migraine with aura. Aura is the same whether or not it is accompanied by headache and carries the same risk of ischaemic stroke as migraine with aura. The VARS score does not depend on presence of headache so VARS can be used to screen for aura without headache.
Case study
A 17-year-old woman was referred for contraceptive advice. She was taking the desogestrel progestogen-only pill but was unhappy with this method because of frequent unscheduled bleeding. The referral information stated that she had migraine with aura since the age of 15 years, so her preferred choice of CHC was contraindicated. The stated history was that the patient “lost her vision” and then developed a headache associated with nausea and vomiting, which resolved with sleep.
On direct questioning, the visual symptoms started a couple of hours before the headache and lasted for the duration of the attack. They were worse if the accompanying headache was severe. She experienced blurred vision and difficulty focusing, which resolved if she closed her eyes. When shown pictures of typical aura and asked if she experienced anything similar, her response was ‘No’.
This shows the importance of asking the right questions regarding visual symptoms to make the correct diagnosis. In this case, the duration of visual symptoms was longer than 60 minutes, they were present both before and during the headache, and the symptoms were non-specific. The correct diagnosis was migraine without aura, with no contraindication to CHC.
What to do when in doubt
There are always times when the story is unclear and it is impossible to be completely certain about the diagnosis. If in doubt, progestogen-only or non-hormonal contraception can be used while the woman keeps a diary of symptoms for subsequent review.
Conclusions
Migraine aura, with or without migraine headache, is an independent risk factor for ischaemic stroke and contraindicates use of CHC. Migraine without aura is not a risk factor for ischaemic stroke and CHC may therefore be used.
Visual symptoms are common in migraine, both with and without aura, which can lead to diagnostic confusion. Over-diagnosis of aura results in under-prescription of CHC. Simple screening tools such as ID-Migraine for migraine without aura or VARS for migraine aura can aid diagnosis in the clinical setting, enabling correct identification of women who can and cannot be offered the option of CHC.
Acknowledgments
The author is grateful to Alison Frith and Manori Bandara for their comments on the manuscript.
References
Further reading/information
Footnotes
Competing interests In the last 3 years the author has acted as a paid consultant to, and/or her department has received research funding from, Bayer Healthcare, Consilient Health, and Menarini.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Review
- Highlights from this issue