Article Text

Abstract
Aim To assess the incidence of visible strings of intrauterine contraceptive devices (IUDs) after postplacental insertion following vaginal or caesarean delivery and to establish a management protocol of follow-up visits when strings are not visualised.
Methods This was a prospective study of a cohort of 348 women who underwent postplacental insertion of Copper-T 380A IUDs following vaginal or caesarean delivery, conducted at a hospital in New Delhi, India. Women were followed up at 6 weeks, 3, 6 and 12 months after IUD insertion and were questioned about IUD expulsion or removal at each visit. The cervix was inspected to visualise the IUD strings. All women whose IUD strings could not be visualised at the cervical os at any given follow-up were identified. We analysed the cumulative incidence of visible strings and of procedures performed to locate the IUD when strings were not visible.
Results At 1 year follow-up, the IUD was in situ in 313/348 (89.9%) women. There were eight (2.3%) expulsions and 15 (4.3%) IUD removals. Among women with IUDs in situ, the strings were not visible in 73 (21%) cases. Pelvic ultrasound confirmed intrauterine position of the IUDs in these cases. At 1 year, string visibility was significantly lower after intra-caesarean insertions as compared to vaginal insertions (72.4% vs 98.1%; p<0.05).
Conclusions Visualisation of strings after postplacental vaginal insertion is more common than after intra-caesarean insertion. Pelvic ultrasonography can be used to verify the presence of the device in cases of missing strings.
- intrauterine devices
- education and training
Statistics from Altmetric.com
Key message points
Non-visibility of strings is more common following intra-caesarean Copper-T 380A intrauterine contraceptive device (IUD) insertion than after postplacental vaginal insertion.
Pelvic ultrasonography at 6 weeks and 6 months is usually sufficient to verify the presence of an IUD in situ in cases of missing strings.
Counselling and reassurance about location of an IUD in the uterus can improve continuation rates after intra-caesarean IUD insertion.
Introduction
The current national policy in India is to promote hospital delivery and to strengthen postpartum family planning. The role of immediate postpartum intrauterine contraceptive device (IUD) insertion, also referred to as postplacental IUD (PPIUD) insertion, as a method of postpartum contraception has expanded in the recent past. The government of India is taking the initiative to promote PPIUD insertion by training service providers and giving them incentives. This has resulted in a significant increase in the number of Copper-T 380A IUD insertions during the immediate postpartum period. PPIUDs are still emerging as a relatively new contraceptive choice with its unique set of problems.1
Copper-T 380A IUD strings are not visible immediately after postplacental insertion. Involution of the uterus makes the strings descend and become visible. In a significant number of women, threads are not visible on speculum examination at follow-up visits, especially after intra-caesarean (ICS) insertions.2–4 This may be a source of apprehension for service providers as well as for the women, who are always concerned about possible perforation of an IUD into the abdominal cavity. This misconception is the major deterrent for women in India to use this effective and safe, long-acting reversible contraception method. This myth gets momentum when women are informed about non-visualisation of their IUD strings during follow-up visits. Despite the fact that Copper-T 380A IUD services are provided free of cost in India, the method still remains largely underutilised.
Hence, a number of questions with regard to missing strings following PPIUD insertion have arisen that need to be answered. These questions are:
What is the magnitude of this problem?
What proportions of missing strings are due to unnoticed expulsion, non-descent or retraction of the strings, or perforation of IUDs into the abdominal cavity?
Should IUDs be removed in cases of missing strings?
What method of removal should be used in such cases and is such removal difficult?
What should be the duration of follow-up for women with PPIUD insertions and should this be scheduled earlier than with interval insertions in order to detect missing threads in time?
What decisions will women take when faced with the situation of non-visible strings?
Knowledge of these issues should be helpful for effective counselling of women undergoing PPIUD insertion. At present, there are very few studies in the literature dealing with missing strings after such insertion.2–6 We therefore conducted a prospective observational study of a large cohort of women who received PPIUDs in a tertiary care centre in Northern India. The study endeavoured to find possible solutions to some of the questions raised. The aims of the study were:
To assess the cumulative incidence of visible IUD strings after postplacental insertion following vaginal or caesarean delivery
To assess procedures performed to locate IUDs in cases of missing strings at follow-up visits
To assess women's perceptions about non-visibility of strings
To establish management protocols for this situation.
Methods
Study design
The study was conducted at Safdarjung Hospital, which is a tertiary care and teaching hospital in New Delhi, India, providing medical services free of cost. There are approximately 24 000 deliveries annually with a caesarean rate of 20%. Between 1 January and 28 February 2013, 348 women undergoing postplacental insertion of a Copper-T 380A IUD following vaginal or caesarean delivery were enrolled and followed up in a prospective cohort study. Approval for the study was given by the institutional review board of Vardhman Mahavir Medical College and Safdarjung Hospital.
Study participants
The study was carried out on women who delivered at our hospital and underwent PPIUD insertion. All pregnant women who attended our antenatal clinic or were admitted to the labour ward were counselled regarding postpartum family planning methods. Those women who desired PPIUD were informed regarding its advantages, limitations and effectiveness and were screened as per World Health Organization (WHO) medical eligibility criteria7 in the antenatal period, as well as immediately prior to IUD insertion following delivery.
Inclusion criteria for PPIUD insertion comprised women who met the WHO Standard Medical Criteria for IUD insertion and who did not have a complicated pregnancy, operative vaginal delivery or complications arising during caesarean delivery.7 Women were recruited if they met the following criteria: (a) Age ≥18 years, (b) desired IUD as a postpartum contraception, (c) willing to come for follow-up for at least 12 months and (d) able to give informed consent. Women who fulfilled the criteria were enrolled and had postplacental insertion (i.e. within 10 minutes of placental delivery) of a Copper-T 380A IUD if there was no evidence of chorioamnionitis or antenatal leakage of amniotic fluid for more than 18 hours, postpartum haemorrhage (PPH) or extensive birth trauma.
We enrolled 400 subjects during the antenatal period, based on approximately 4000 deliveries occurring at our institute during 2 months of recruitment period and on the proportion (10%) of women we anticipated would desire an IUD for contraception postpartum and who were willing to come for follow-up for 1 year. We assumed that 3% would be ineligible for an IUD due to labour-related factors and another 10% would either refuse IUD insertion at delivery or not deliver at our centre.
Study procedures
Women were enrolled from 1 January to 28 February 2013, with follow-up to February 2014. Copper-T 380A IUDs were loaded by ‘no touch’ technique inside a sterile pack using Kelly (placental) forceps. Vaginal PPIUD insertion was done using Kelly forceps by a standardised technique.1 Fundal placement of the IUD was ensured and confirmed by abdominal ultrasonography. ICS postplacental insertion was done using ring forceps through the uterine incision, placing the IUD at the fundus. All the insertions were done by resident doctors who had received training in PPIUD insertion. Antibiotics were administered as per the hospital's protocol for caesarean section and women were observed for evidence of PPH or sepsis. IUDs were obtained through the Ministry of Health, India.
Follow-up
The women were asked to return for scheduled follow-up visits at 6 weeks and at 3, 6 and 12 months. They were instructed to report at any time if they experienced pelvic pain, discharge per vaginam, unusual bleeding or missed periods. If women failed to attend for follow-up at the specified time, they were contacted by telephone and if required were visited by a health worker at their home.
At each follow-up visit, women were interviewed and qualitative data such as bleeding, cramping, sexual activity, breastfeeding and symptoms of infection were ascertained. Physical and pelvic examinations were performed to verify the presence of the IUD. Strings were cut short at the 6-week follow-up visit or earlier if they protruded from the vaginal introitus. In the case of missing strings, the cervix was probed with a cervical cytology brush to locate curled strings in the cervical canal with minimal risk of displacement of the device. Ultrasonography was done only in cases where strings were not visible even after probing the cervix. Women with accidental pregnancy, IUD expulsion or any other complications were treated accordingly. Women in whom IUD strings were not visible even at their 6 months follow-up visit were asked about their most perceived fear of non-visualisation of IUD strings.
Data analysis
Study parameters included string visibility at each follow-up, ultrasonography to rule out IUD expulsion and to localise the position of the IUD in case of non-visualisation of strings, mode of IUD removal if requested, and women's perception of non-visibility of strings and its effect on continuation of this contraceptive method. Statistical analysis was performed using SPSS computer software (V.20, SPSS Inc., Chicago, IL, USA). Descriptive data were summarised as percentages or means. The Chi-square (χ2) test was used to measure the strength of associations between the variables (a p value <0.05 was considered statistically significant).
Results
A total of 348 women fulfilling the inclusion criteria were included in the present study. There were 63 vaginal (Figure 1) and 285 ICS PPIUD insertions (Figure 2). There were no cases of PPH or puerperal sepsis. Over half (56.7%) of those who accepted PPIUD were aged 21–25 years (56.7%), with just under one-third (31.9%) aged 26–30 years. Primiparous women accepted PPIUD more often in comparison to others. Nearly half (45.1%) of the acceptors had at least higher secondary education with about a quarter (25.2%) having secondary education and no further (Table 1).
Demographic characteristics of the study participants; women who received a postplacental intrauterine contraceptive device
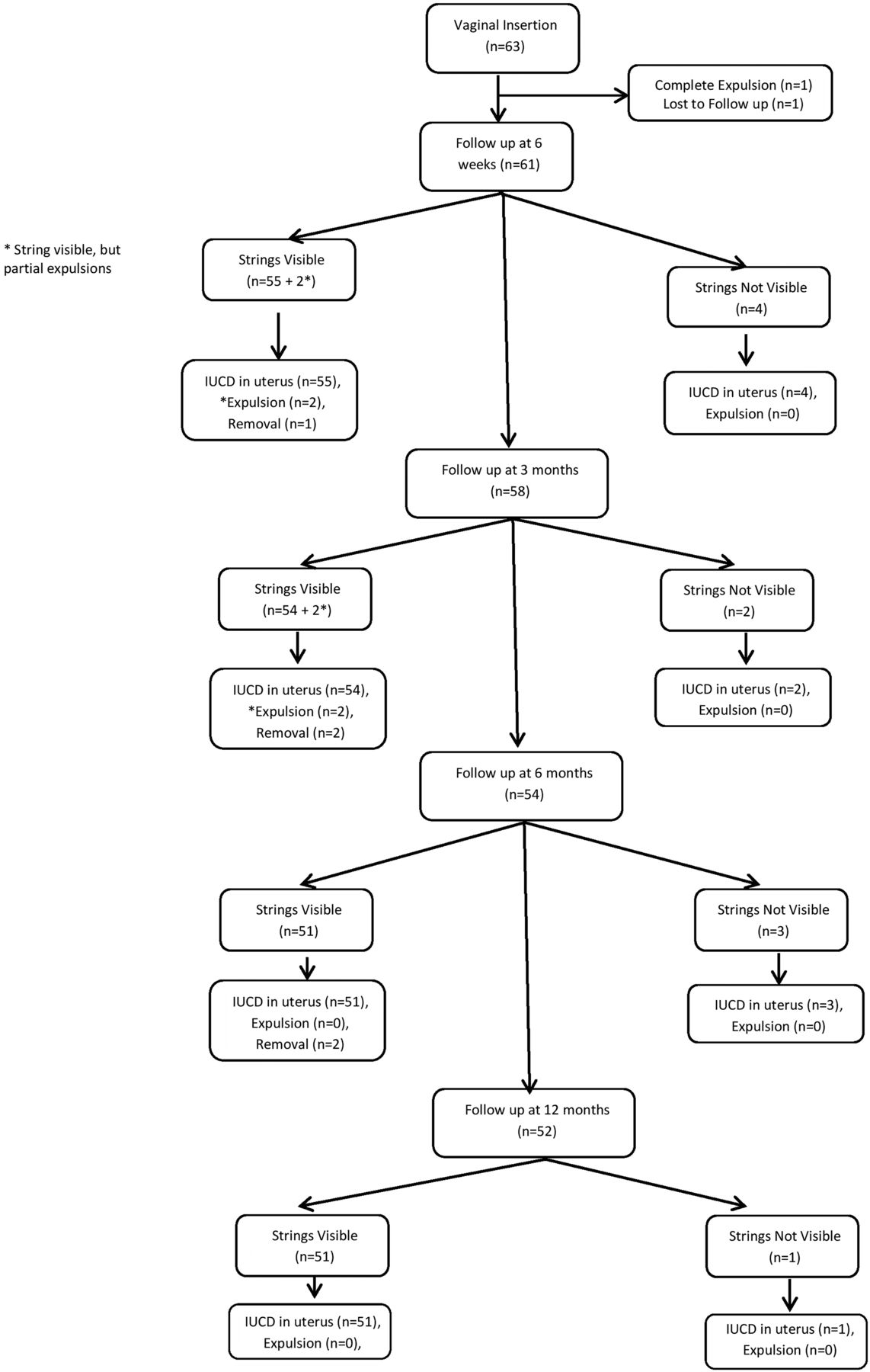
Flow chart of patients undergoing vaginal insertion of postplacental intrauterine contraceptive device (PPIUD). IUCD, intrauterine contraceptive device.
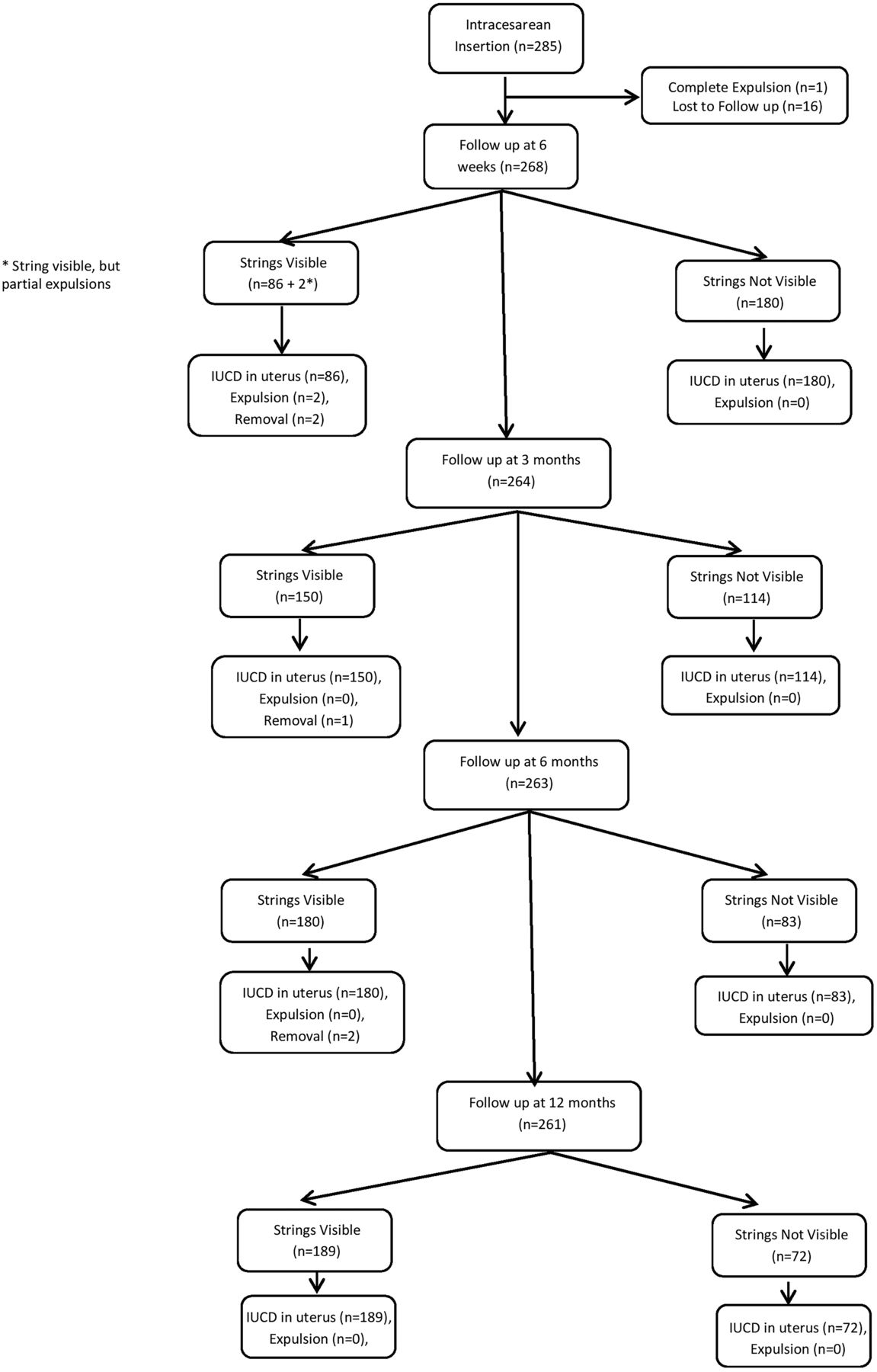
Flow chart of patients undergoing intra-caesarean insertion of postplacental intrauterine contraceptive device (PPIUD). IUCD, intrauterine contraceptive device.
Three hundred and twenty-nine (94.5%) women attended the first follow-up visit at 6 weeks. Seventeen women did not attend any scheduled follow-up visits and were lost to follow-up of the investigators. Three women had their IUDs removed, of which two removals were done outside the hospital. Strings were visible in 141/329 (42.9%) cases at 6 weeks. Non-visible strings were retrieved from the cervical canal using a cervical cytology brush in 10 cases of vaginal insertion. String visibility at the first follow-up was more frequent after vaginal insertion than after ICS insertion (90.2% vs 32.1%; p<0.05). With each successive follow-up visit, strings became visible more frequently (93.1% vs 56.8%; p<0.05 at 3 months, 94.4% vs 68.5%; p<0.05 at 6 months, 98.1% vs 72.4%; p<0.05 at 12 months for vaginal and ICS insertions, respectively) (Table 2).
Visualisation of strings at discharge and follow-up visits
The reason for non-visibility of the IUD strings was non-descent in all cases. Transvaginal sonography confirmed the presence of the IUD in the uterus. There were no cases of IUD misplaced outside the uterus (perforation). A total of eight expulsions were seen during the entire follow-up period, the majority of which occurred following vaginal insertions as opposed to ICS insertions. There were two complete expulsions detected by women themselves and six partial expulsions detected during pelvic examination at follow-up visits (Table 2).
Fifteen (4.3%) women requested removal of their IUDs (Table 3). The strings were not visible in 6/15 (40%) women who requested IUD removal and all these were ICS insertions. In 4/6 cases with non-visible strings the IUD was removed using alligator forceps. Hysteroscopy-guided removal was required in two cases as the IUD was partially embedded in the myometrium. There was one case of uterine perforation while removing an IUD. No case of pelvic inflammatory disease following IUD removal was noted.
Methods of removal of postplacental intrauterine contraceptive device
Women with non-visible strings at the 6-month follow-up visit were interviewed about their perception of non-visibility of IUD strings. They expressed apprehension over non-visibility with regard to the need for further follow-up to detect expulsion, the risk of becoming pregnant if unnoticed expulsion occurred, and the majority were worried about the possibility of the IUD having perforated into the abdominal cavity. A few women expressed concern about the need for surgical intervention if removal was required (Table 4). None of the women requested IUD removal for the reason of non-visualisation of strings. There was one case of a pregnancy reported with the IUD at the uterine fundus at the 12 months follow-up visit. This woman was in the ICS insertion group. She opted for medical termination of the pregnancy.
Women's perceptions of non-visualisation of strings at 6 months follow-up visit
Discussion
Recent experience of postplacental insertion of Copper-T 380A IUDs in India has demonstrated increased utilisation of this long-acting and effective contraceptive device by eligible couples. Previously, concerns about PPIUD focused on high expulsion rates, but lower expulsion rates have been reported more recently with improvements in insertion technique and experience of service providers.8 However, the issue of non-visualisation of strings after postplacental Copper-T 380A IUD insertion, especially with ICS insertions, is a major deterrent to optimal utilisation of this effective family planning method and needs to be addressed.
During the 2-month recruitment period in the present study there were more ICS IUD insertions than vaginal insertions. Women undergoing caesarean section were keener to use the IUD as a postpartum contraceptive than those delivering vaginally. Immediately after both vaginal and ICS postplacental insertion of Copper-T 380A IUDs, the strings were not visible in all the women (Table 2). The length of the threads of the Copper-T 380A is 11.5 cm. This is likely to be the reason for the non-visibility of the strings in the majority of subjects. Immediately after expulsion of the placenta the uterine size corresponds to 5 months of pregnancy, hence the IUD strings are not visible. Non-visibility of the strings of the Copper-T 380A at the time of insertion in fact reassures the provider about fundal placement of the IUD.
The first follow-up visit was planned for 6 weeks as this coincided with postnatal visits. We hypothesised that by this time, due to uterine involution, descent of IUD strings and expulsions if any would have occurred.
Our follow-up rate of nearly 90% is adequate as our counsellors were in regular telephone contact with the women. Visibility of the strings increased at successive follow-up visits as the uterus involuted (Table 2). Resumption of menstruation may also be a contributing factor for increased string visibility with the passage of time. However, in many cases threads may become curled up and not be seen at the cervical os. Pelvic ultrasound was performed in women in whom the strings could not be visualised at the external os at any given follow-up visit, even after attempting the manoeuvre of sweeping the strings down from the cervical canal using a cervical cytology brush.
In our study, 89.9% (313/348) women returned for follow-up during the study period. Among women with an IUD in situ, the strings were visible in 76.7% (n=240/313) women at 12 months follow-up, whereas Lara et al. visualised strings in 90.2% women 1 year after Copper-T 380 IUD insertion. This disparity could be due to higher proportion of ICS insertions compared to vaginal insertions in our study. String visualisation was significantly more frequent after vaginal than after ICS insertion at all follow-up visits (p<0.05). Other studies have also reported missing strings more frequently after ICS insertion than after vaginal insertion.2–4 ,6
The inability to visualise strings in nearly one-quarter of women at 12 months follow-up following IUD insertion at the time of caesarean delivery is of concern to us and is perhaps the one potential disadvantage of ICS insertion. Levi et al.4 and Sucak et al.9 examined patients at 6 weeks post-caesarean delivery and found that they could visualise the strings in 28% and 30% of women, respectively, similar to the 32% we visualised at 6 weeks, and less than the 64% that we visualised at 6 months.
Missing strings after IUD insertion is clinically relevant as this may indicate IUD expulsion, malposition or uterine perforation, or simply that the strings are in the uterine cavity without any significance. Non-visualisation of strings may be a source of apprehension for women as well as providers. Interviews with women whose strings were not visible at 6 months showed that their main concern was about possible perforation of their IUD into the abdominal cavity followed by the need for a surgical procedure when removal is required (Table 4). Counselling women regarding the later visibility of strings in a significant proportion of cases (98.1% of vaginal and 72.4% of ICS insertions at 12 months) is helpful in alleviating their fears.
Visibility of strings is important as it aids the removal of IUDs and non-visibility may therefore pose a problem for service providers when removal of an IUD is required. We were able to remove the IUDs using alligator forceps in 4/6 cases of non-visualisation of strings following ICS insertion. However, invasive methods including hysteroscopic removal were needed in two cases where the IUD was partially embedded in the myometrium and in one case there was a uterine perforation while attempting removal of the IUD.
Alligator forceps may be used for removal of IUDs with missing strings. Hysteroscopic removal of IUD may be required if an IUD is embedded in the myometrium. Ultrasound guided removal of IUD is another option that needs to be evaluated further. Invasive procedures to remove IUDs may increase the risk of uterine perforation.
In our study, Copper-T 380A IUD strings were visible in more than 90% women by 6 weeks after vaginal insertion. There were no cases of missing strings due to unnoticed expulsion or perforation; all were due to non-descent of the strings. In view of the observed higher expulsion rates (5/63, 7.9%) after vaginal insertion, one must ensure that the IUD is in place. With ICS insertions, expulsions were infrequent (3/285, 1.1%) and were observed within the first 6 weeks. None of the expulsions were observed after 6 months in either group. Our findings are in accordance with other studies that have reported that expulsion is more frequent after immediate postplacental vaginal IUD insertion as compared to ICS insertions.4 ,9–11
All the complete expulsions were detected by the women themselves and partial expulsions were detected during pelvic examination at follow-up visits. These women were advised to use alternative contraception. No pregnancies were observed in women in whom expulsion occurred; all these women were breastfeeding and had lactational amenorrhoea.
Often the missing strings can be located by probing the cervical canal with a cervical brush. Ultrasonography may be required to rule out complete expulsion in the case of non-visualisation of strings at follow-up visits in the first 6 months. As expulsions are infrequent after this period, frequent sonography is not recommended. Our findings are in keeping with other reports where a significant proportion of expulsions occurred in the first 3 months after IUD insertion.9 ,11 Marchi et al.12 recommended an ultrasound scan to verify appropriate intrauterine positioning for women with persistent missing IUD strings and suggested repeating the ultrasound (if available) on at least one additional visit, as they found a 2.4% likelihood that expulsion may have occurred at the time of subsequent visits.
Lester et al.3 expressed concern over the inability to visualise strings in 56% of women who had Copper-T 380A IUDs inserted at the time of caesarean delivery and regarded this as perhaps the one potential disadvantage of ICS insertion. Nelson et al.5 studied the feasibility of a novel technique of increasing the length of the tail strings of a Copper-T 380A by tying on suture material and guiding the strings out through the cervix at the time of intraoperative placement, so that if a complication developed during uterine involution, the device could be removed easily. Grover and Singh13 observed that the strings of vaginal PPIUDs only become visible at the cervical os immediately after insertion if the length of string is around 16±2 cm. They suggested that IUDs for postplacental insertion should be manufactured with inbuilt increased string length (approximately 18 cm). In their study, the IUD string was extended by knotting on 2–0 Prolene suture material immediately before insertion. Designing an IUD with long strings and guiding the strings down through the cervical canal during ICS insertion is a possible solution to the problem of non-visualisation of strings after that procedure.
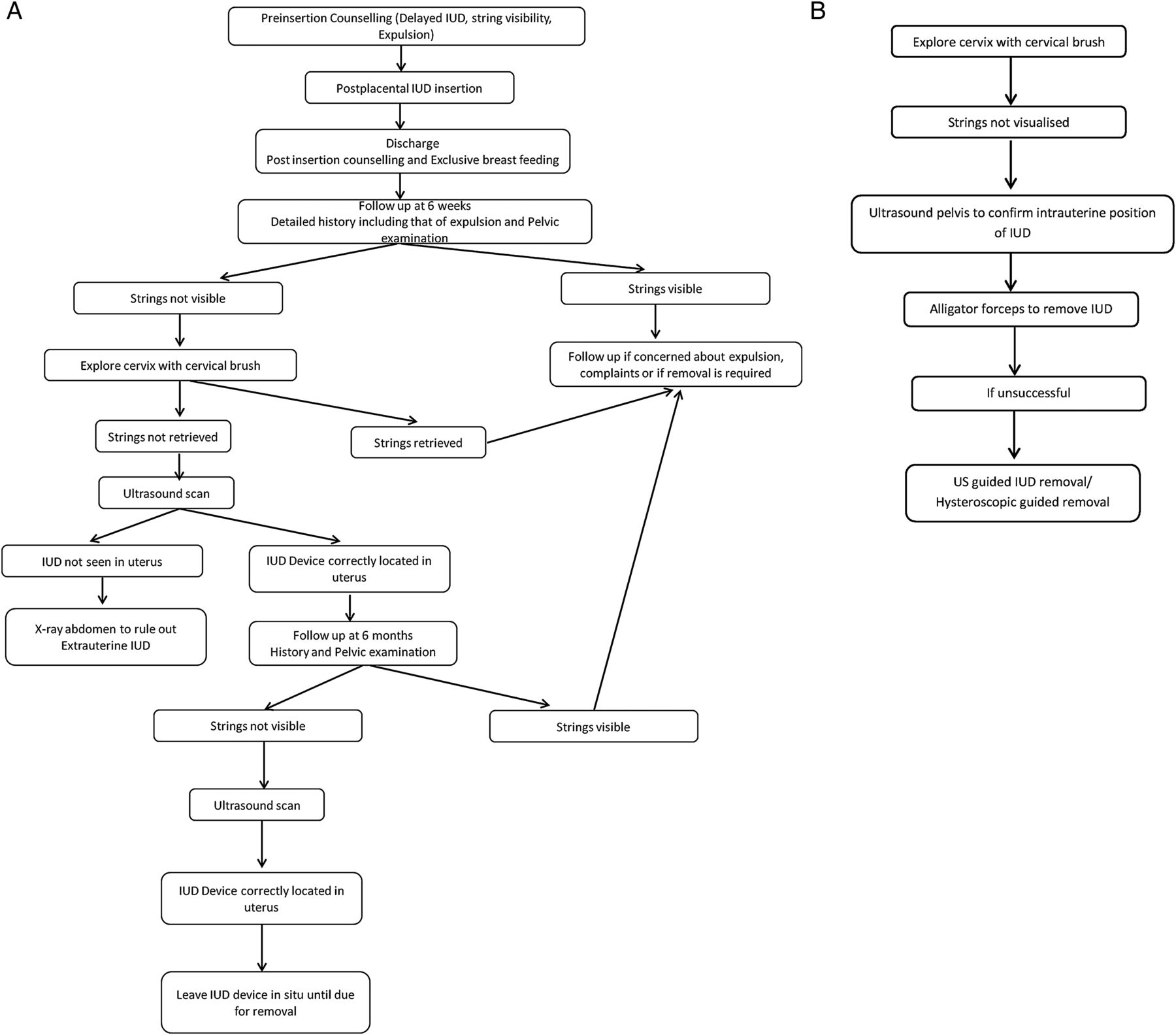
All the women in whom strings were not visible were counselled carefully; hence they decided to continue with the method. IUD removal or replacement is not warranted in the case of non-visible strings. There is a need to train service providers about the potential problems of missing strings following PPIUD insertion, especially ICS insertion, to avoid frequent sonographies and hospital visits and thus to improve PPIUD acceptance and continuation rates. Based on the findings of our study, we recommend a simplified management protocol for IUDs with missing strings (Figure 3A, B).
{kind=link}
{kind=link}
{kind=link}
(A) Management protocol for missing intrauterine contraceptive device (IUD) strings. (B) Removal protocol for IUD with missing strings. US, ultrasonography.
Strengths and limitations of this study
A strength of this study is the high follow-up rate, despite the large sample size, which was achievable due to constant contact between the counsellor and study participants. However, limitations of the study include its non-randomised nature in comparing string visibility in ICS and vaginal insertions and the fact that ultrasound was not done for cases in which strings were visible, so some cases of partial expulsion may have been missed.
Conclusions
Missing strings at follow-up visits are commonly observed following postplacental ICS Copper-T 380A IUD insertions. Pre-insertion counselling of women regarding non-visualisation of strings after PPIUD insertion and ultrasonography done twice during follow-up, at 6 weeks and 6 months, is sufficient to rule out expulsions and thus to alleviate anxiety and improve continuation rates. A pelvic ultrasound scan should be the initial procedure and is usually sufficient to locate IUDs whose strings are not visible. Alligator forceps may be used to remove IUDs with missing strings.
Footnotes
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institute Ethics Committee, Safdarjung Hospital and Vardhman Mahavir Medical College, Delhi.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue