Article Text

Statistics from Altmetric.com
Background
The ‘My Body Back’ (MBB) Clinic at St Bartholomew’s Hospital in London, UK was awarded the 2016 Faculty of Sexual & Reproductive Health Care (FSRH) David Bromham Annual Memorial Award for work that has furthered the practice of sexual and reproductive healthcare through inspiration, innovation and energy. This article is adapted from the authors’ presentation delivered at the FSRH Current Choices Conference 2016 and describes the clinic and its rationale. Further articles describing the service evaluation and clinical outcomes are in preparation.
The My Body Back Project helps women who have experienced sexual violence. These women often feel isolated, traumatised and unable to access healthcare.1 Founded in August 2015, the MBB Clinic is a unique cervical screening clinic designed for such women.
Why is there a need for a special cervical smear clinic for women who have been sexually abused?
One in five women does not attend for cervical screening; among these are those who have experienced sexual violence.2–4 There is evidence to suggest that sexually abused women may be at increased risk of cervical cancer and avoid healthcare, including cervical screening.5–8 Pavan Amara set up the MBB Project as a result of her own experiences following rape. Pavan, a freelance journalist, interviewed women who had experienced sexual violence, and research nurse Louise Cadman separately carried out a study in this group of women, researching access and uptake of cervical screening. Informed by the women themselves, they both reached similar conclusions regarding the need for specialised care around cervical screening for women who have experienced sexual violence. As a consequence this collaborative clinic was set up to offer these women the opportunity for equal access to healthcare.
Listening to Pavan and Louise at the 2014 FSRH Current Choices Conference in London describing the difficulties for these women and highlighting the need for specialised clinical services to enable them to have their often long-overdue smears, Jill Zelin was inspired to say “I can do that”. Jill was already running a similar service for women with vaginismus and genito-pelvic pain alongside a consultant psychologist and believed that they might have the expertise and experience to facilitate an MBB cervical screening clinic.
The MBB Clinic was launched in August 2015 after 8 months of meetings and preparation. The clinic offers a package of care in partnership with the MBB Project. Practical issues included lack of funding, establishing a cohort of volunteers, and obtaining honorary contracts. An appropriate ‘safe’ clinical space and design also had to be found .
Demand has been such that the clinic has continued beyond the initial 6-month pilot and is now an established (though not commissioned) component of Barts Health Sexual Health service. Of the first 50 women seen, 45 had a smear at their first visit, two at their second, two declined screening and one was an inappropriate referral.
The clinic team consists of Pavan Amara, administrator and advocate, Louise Cadman, smear taker and data manager, Jane Vosper, whose input as the clinical psychologist is key to this unique clinic, and Jill Zelin, a sexual health consultant and smear taker. A group of MBB volunteers organise appointments and attend the clinic to welcome women, offer refreshments and generally provide the normality and care to help bring these women back to a safe mental space.
What did women want?
Women’s needs were grouped into five overarching themes:3
Disclosure of sexual violence
Safety, trust, respect and shared control
Communication related to sensitivity and understanding of common terms which potentially trigger negative reactions
The procedure and the clinic environment, which commonly parallel the situation during the sexual violence or subsequent medical examinations
Time and space
How have we tried to meet these needs?
The patient pathway (Figure 1) has been informed by both the women and the MBB team.
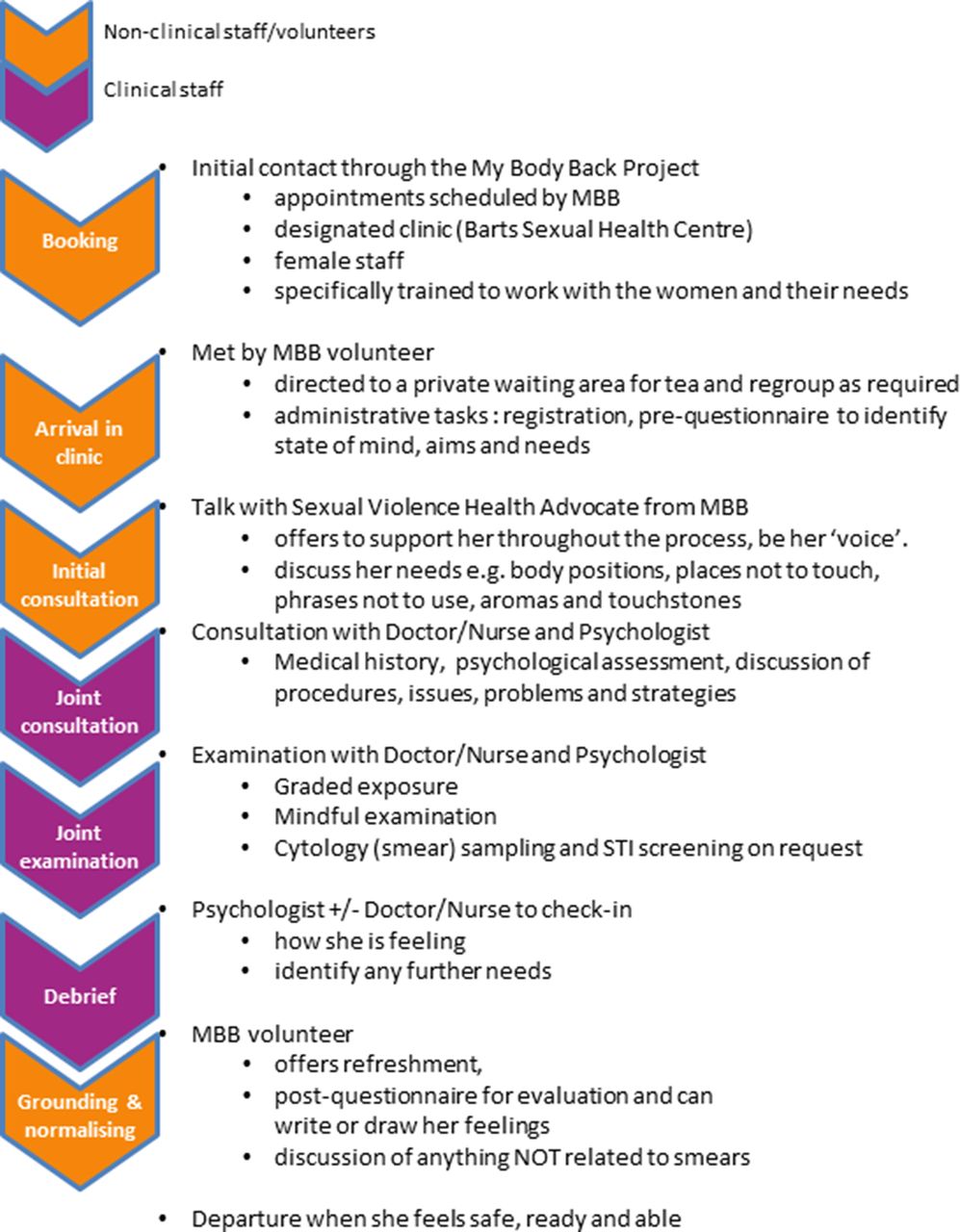
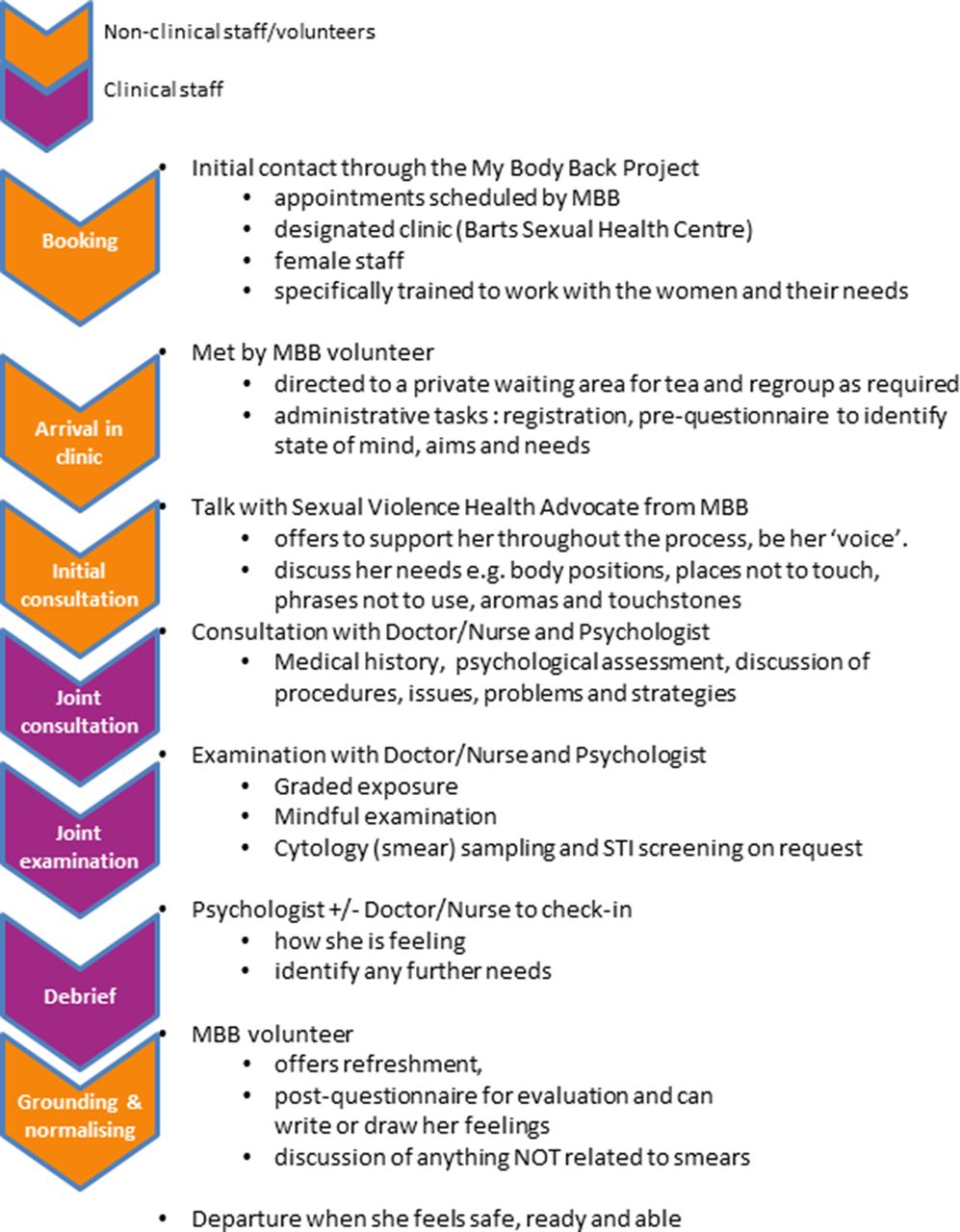{kind=link}
Patient pathway.
The clinic aims to meet the specific needs of the women by ensuring a collaborative experience rather than one where the smear taker has control over them; there is no need for them to disclose any information around the sexual violence unless they choose to do so. Mere attendance at the clinic is sufficient to identify their past experiences and so remove the burden of disclosure. We offer support before, during and after the consultation in the form of volunteers and refreshments, as well as the expertise of specialist psychologists and other clinical staff.
Beyond this pathway we have ensured good contacts with the colposcopy service for women requiring ongoing investigation, supported by a member of the team if required.
It is the small things that count – good signage, written information, refreshments, safe space, non-judgmental, no need to disclose abuse, reactions are understood and that the team, especially volunteers, are supported so they can continue to give their time. The specialist support offered by the trained psychologist helps to identify which strategies may help the woman through the process and to signpost her to other services specific to her needs such as trauma counselling or the management of vaginismus. Such needs are often extremely complex and difficult to manage, and the particular expertise within the field of mental health of the psychologists in the MBB Clinic is invaluable.
What quality indicators have we used to track progress?
Women complete questionnaires before and after their appointment. Prior to the appointment we endeavour to ascertain their expectations from the clinic visit, anxiety levels and confidence in their ability to undergo a smear test. We identify any specific needs we can try and meet.
Cytology results are monitored and women given the contact details of a member of the clinical team in case they need advice.
How has the clinic been received?
The clinic elicited much positive media interest and the significant number of enquiries received by the MBB Project from women wanting to use the service demonstrates its need. A similar model has been used to establish a clinic for male survivors of sexual assault and a maternity clinic. Our group has run workshops and given presentations to other services that may wish to set up MBB services of their own.
What are the pitfalls?
The main pitfall of this clinic is ensuring its sustainability. A service cannot run on goodwill alone. Our wish list includes more specially trained people (clinicians and volunteers) to staff and run more clinics, a clear funding stream and, very importantly, our own guaranteed clinical space.
This cohort of women frequently present with complex needs. Some are prompted to attend because of concerning physical symptoms; others report significant mental health difficulties. These need to be considered during and after the appointment.
Another pitfall is the demand from other services keen to include a similar model within their specialty. Advising on this requires more administration time than anticipated as we develop training packages and share best practice.
Advice to others considering setting up a similar service - the ‘non-negotiables’ of the MBB Clinic package
There has been much discussion among our team and others about what makes the MBB Clinic unique, which aspects could be adapted or dropped by others setting up an MBB Clinic, and which are essential to the model (Box 1). We would expect these ‘non-negotiables’ to be included in any service specification using the name ‘My Body Back’.
List of ‘non-negotiables’ to be included in any service specification using the name ‘My Body Back’ (MBB)
Access to the service via the MBB website
Contact and support from non-clinical MBB volunteers before the appointment
Use of MBB branded/approved:
Signage
Stationery
Handbook
Questionnaires/evaluations
Training for all staff from MBB-approved trainers or MBB training package
MBB-trained:
Volunteer(s)
Advocate(s)
Experienced smear taker(s)
The clinic:
Dedicated space, including waiting area
Appointments of minimum 1-hour duration
Facilitated/streamlined registration
Provision of refreshments, art materials, sensory stimulation (e.g. aromatherapy oils, pebbles)
Psychology input:
Team supervision by a psychologist trained and experienced in sexual health/trauma
Preference for a joint clinical consultation with doctor/nurse and clinical psychologist
If no appropriate clinical psychologist is available:
A psychologist trained and experienced in sexual health/trauma to see women with complex needs
Counsellors or other professionals with appropriate specialist training in sexual health and sexual trauma may be used but training and supervision must be provided by a psychologist trained and experienced in sexual health/trauma
Other advice:
Set up your patient pathways first
Honorary contracts for the volunteers and advocates may be required
Raise awareness in your service and trust
Establish clear referral criteria and boundaries
Conclusions
The MBB Clinic offers an opportunity to women who are unable to access cervical screening to achieve parity with those who can. It requires significant financial outlay but it could be argued that it may prove cost effective in the long term in terms of cervical cancer prevention. In a cash-strapped National Health Service, departments wishing to run an MBB Clinic could explore creative solutions to funding such as fundraising or financial support from charities.
Acknowledgments
The authors would like to thank all the women who took part in interviews and responded to surveys to help the authors understand what was wanted and needed. Also to all the MBB volunteers who generously give their time to provide the ‘normality’ and support women require. Thanks to Amanda O’Donovan who was instrumental in the setting up of the clinic and to all colleagues who have supported this innovative service including Anna Parberry (Nurse Colposcopist), Stuart Gibson, Pauline Inglis and Penny Thexton.
Footnotes
Contributors JZ, LC, PA, JV SM all helped to set up and run the clinic. JZ & LC were responsible for writing the article. P.A, J.V. and S.M. reviewed and commented on the draft.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement N/A.
Linked Articles
- Highlights from this issue