Article Text

Abstract
Objective To assess postpartum contraceptive choices of women participating in group versus traditional prenatal care.
Methods This is a retrospective cohort study assessing postpartum contraceptive choices of women participating in group versus traditional prenatal care. Patients were derived from a database of all deliveries from 1 January 2009 to 31 December 2014 at Christiana Hospital in Newark, Delaware, USA. Within this database, group prenatal care patients were identified and a two-to-one matched set of similar traditional prenatal care patients was created. Contraceptive methods utilised by these women were ascertained via chart review. The proportion of women using each method in each care model was calculated. Multinomial logistic regression was carried out for statistical analysis.
Results Included in the final analysis were 867 patients: 289 group and 587 traditional prenatal care participants. Groups were similar in selection of sterilisation, condoms, injection, and other short-acting hormonal contraceptive methods (a composite of patch, vaginal ring, and pills). Group prenatal care patients were more likely to utilise contraception postpartum (as measured by use of no method with AOR 0.50, 95% CI 0.32 to 0.78, P=0.002), particularly long-acting reversible contraceptives (LARCs) (OR 1.67, 95% CI 1.16 to 2.40, P=0.005). This difference was most pronounced for women aged 20–24 years (AOR 1.98, 95% CI 1.10 to 3.56).
Conclusion Participation in group prenatal care as opposed to traditional prenatal care increases use of postpartum contraception and increases uptake of LARCs. The association of group prenatal care participation with LARC use is particularly apparent for women aged 20–24 years.
- counselling
- health education
- long-acting reversible contraception
- hormonal contraception
- service delivery
Statistics from Altmetric.com
- counselling
- health education
- long-acting reversible contraception
- hormonal contraception
- service delivery
Key messages
Women participating in ‘Centering group’ prenatal care are more likely to utilise postpartum contraception than similar women participating in traditional prenatal care.
Women participating in Centering group prenatal care utilise more efficacious methods of postpartum contraception than their counterparts in traditional prenatal care.
Among Centering group prenatal care patients, increased long-acting reversible contraceptive (LARC) use is most pronounced for women at high risk for unintended pregnancy, based on age group.
Introduction
According to 2011 data, 45% of pregnancies in the USA are unintended. Rates of unintended pregnancy are highest among low-income women, women aged 18–24 years, and minority women.1 Delaware consistently ranks among states with the highest rates of unintended pregnancy. This is a public health concern as unintended pregnancy leads to higher rates of adverse pregnancy outcomes for both mothers and babies, negatively impacts women’s personal and professional lives, and costs the government billions of dollars annually.2–4
Prevention of unintended or mistimed pregnancies lies in appropriate use of contraception. Maximum benefit is gained from the most efficacious methods, such as long-acting reversible contraceptives (LARCs).5 The postpartum period is a crucial time for women to initiate effective contraception plans so that subsequent pregnancies may be appropriately timed or future pregnancies may be prevented altogether. In order to achieve this, it is important to incorporate thorough education regarding postpartum contraceptive methods as a priority aspect in prenatal care. Unfortunately, many patients do not develop or adhere to postpartum contraception plans. In studies of low-income women, approximately 80% report receiving postpartum contraception counselling during the prenatal period.6 In a traditional prenatal care practice, however, such counselling is often incomplete, rushed, or an afterthought given the time constraints for an obstetric provider in a traditional office setting.
’Centering Pregnancy' is a model of patient-centred group prenatal care that exists as an alternative to traditional prenatal care at many obstetric sites throughout the USA. Pregnant women of similar gestational ages meet in a consistent group with a women’s healthcare provider, who may be a nurse practitioner, certified midwife or physician, for ten 90–120 min sessions throughout pregnancy and the early postpartum period. There is a set curriculum, with each session focusing on a particular small set of pregnancy healthcare topics.7
Session 4 of the Centering curriculum addresses family planning and sexuality. A study in 2013 showed that women involved in group prenatal care were more likely to utilise family planning services (defined as initiating well-woman care, attending an annual checkup, receiving contraception, or participating in family planning counselling) within their first postpartum year.8 However, differing postpartum contraceptive choices of participants in group prenatal care versus traditional prenatal care is a topic that has not been specifically addressed.
This study sought to compare postpartum contraception methods selected by women participating in these two prenatal care models. It was hypothesised that women participating in group prenatal care would be more likely to utilise more efficacious methods of postpartum contraception than their counterparts who had participated in traditional prenatal care.
Methods
Approval for this retrospective cohort study was obtained from the Christiana Care Health System Institutional Review Board. A compiled database of all patients who delivered infants at Christiana Care Health System in Newark, Delaware, USA from 1 January 2009 to 31 December 2014 was utilised. Women in the initial database were excluded from analysis if they did not fit the following inclusion criteria: residency service patient (ie, not patients of private practice physicians), singleton pregnancy, full-term delivery, clear documentation of previous pregnancy outcomes in prenatal record, received prenatal care in current pregnancy, and demographic data available. All patients who had participated in group prenatal care via the Centering programme were identified within the patients remaining in this database. A two-to one set of traditional prenatal care patients matched to those in the Centering group using Excel search and exclusion functions was created from those patients remaining in the overall database. These traditional prenatal care patients were matched to the Centering prenatal care patients based on the following criteria: age (±2years), race (Black, White, Hispanic, Asian), gravidity (± 1, ie, number of total pregnancies accepted within one pregnancy of the index patient), parity, history of a prior pregnancy termination (yes/no), induction of labour (yes/no), mode of delivery (Caesarean versus vaginal), and year of delivery (± 2 years). Women from the Centering prenatal care group for whom similar patients could not be identified from the traditional prenatal care patient set by these criteria were excluded. Chart review via Citrix electronic medical records was employed to determine the postpartum contraception method utilised by each of the women participating in both of the prenatal care models. Methods of tubal ligation, tubal occlusion, and vasectomy were identified as sterilisation. Women who received depot injections immediately postpartum during hospitalisation as a bridge to a long-term method selected at their postpartum visit were categorised by their long-term method. Women were classified in the implant or intrauterine device (IUD) groups only if insertion was documented. Women were categorised into prescription hormonal contraception groups if documentation indicated discussion of the method and provision of a prescription to the patient. As condoms do not require a prescription, women were placed in this group if they had indicated a desire to use this method in discussion with their healthcare provider. The proportion of women using each contraceptive method (none, condoms, patch, pills, vaginal ring, injection, implant, IUD, sterilisation) was calculated for the two prenatal care models overall as well as by age range subcategories (15–19, 20–24, 25–29, 30–34, 35–40 years – no women over the age of 40 years had participated in Centering prenatal care during this time period) in order to determine if postpartum contraceptive choices were more significantly affected by the prenatal care model for a particular age group, in order to help direct future practice. Odds ratios were calculated via multinomial logistic regression with P values derived from Chi-square testing.
Results
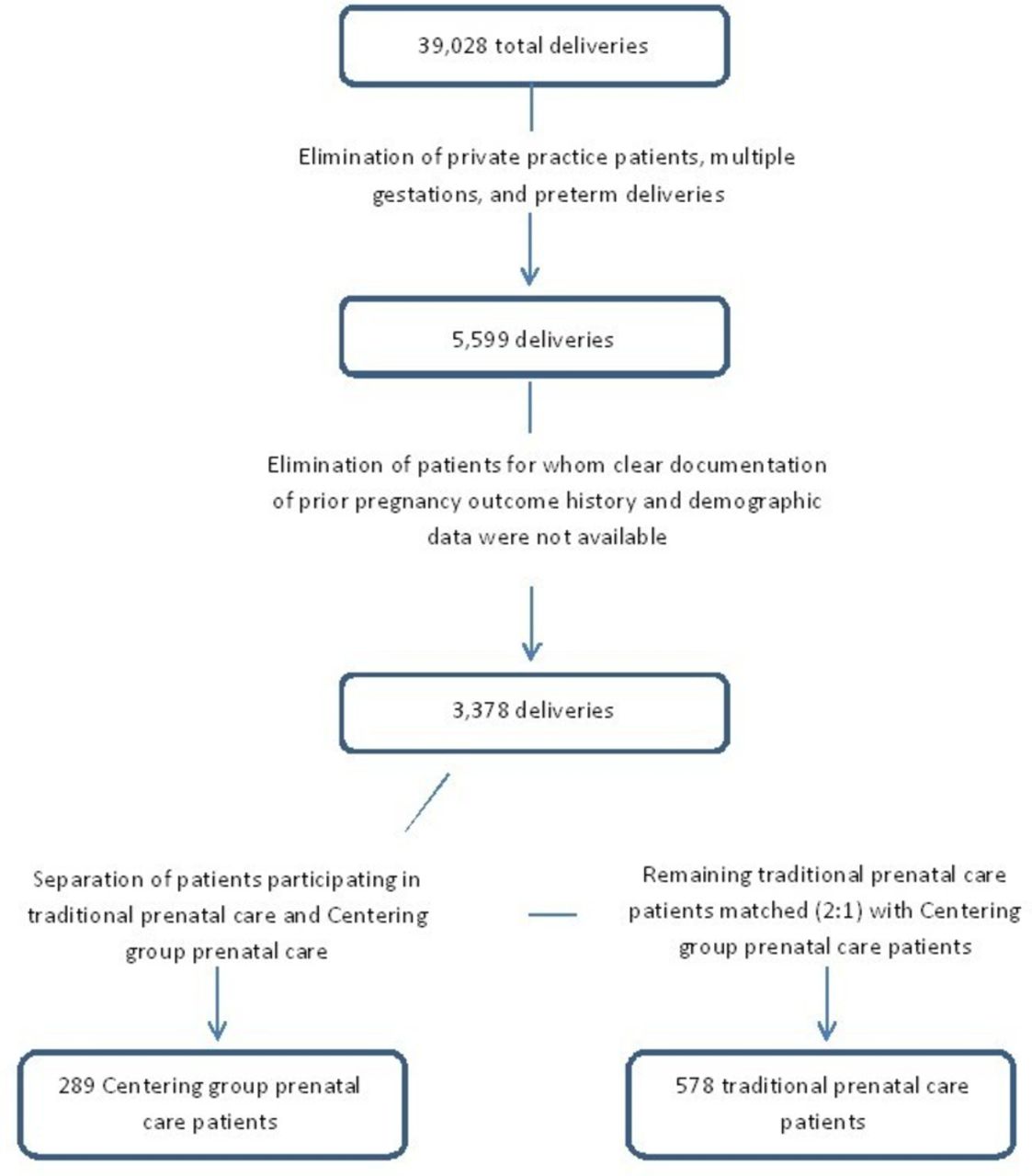
The 39 028 deliveries between 1 January 2009 and 31 December 2014 at Christiana Care Health System in Newark, Delaware, USA were included in the initial database. After elimination of private practice patients, multiple gestations, and preterm deliveries, 5599 patients remained. Of the Centering group prenatal care participants identified within this group, 289 had clear documentation of outcomes of prior pregnancies and demographic data available within the prenatal record. These patients were matched one-to-two to women who participated in traditional prenatal care by age, gravidity, parity, history of termination, pregnancy induction, mode of delivery, and year of delivery. A flow diagram of the patient selection process is shown in figure 1. Overall demographic data are indicated in table 1. The 289 selected Centering group prenatal care participants and 578 matched traditional prenatal care patients were used in the final analysis.
Patient demographics
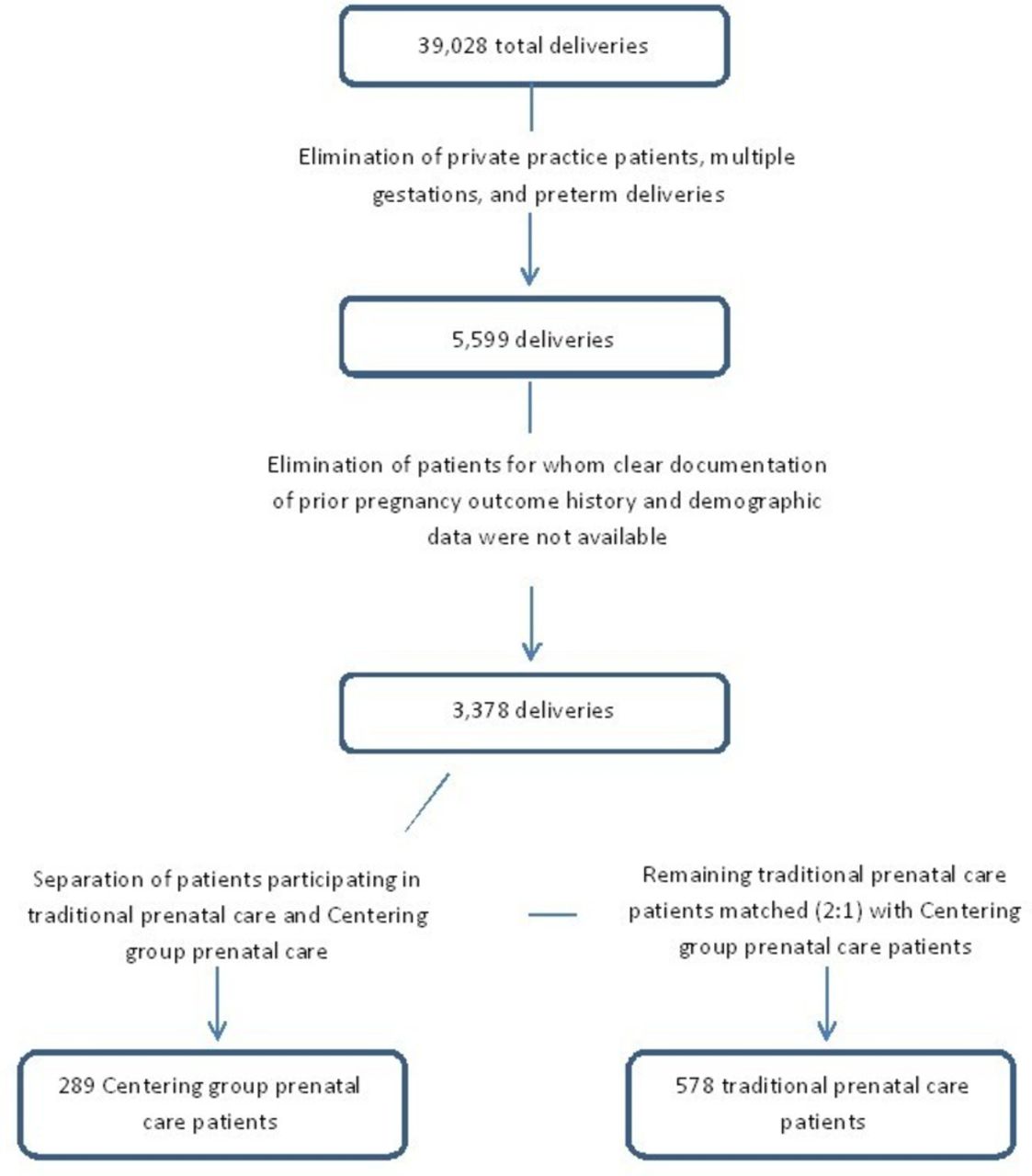
Patient selection – flow chart indicating process of selecting patients from the overall delivery database.
Of all study subjects, 15.1% did not use postpartum contraception and 3.23%, 7.73%, 23.3%, and 33.22% of women chose condoms, sterilisation, short-acting hormonal contraceptives, and injection, respectively. Approximately 17.4% used LARC methods postpartum (table 2). Across all study subjects, sterilisation was correlated with each increase in parity by 1 (AOR 2.02, 95% CI 1.94 to 2.66, P≤0.0001) and with history of pregnancy termination (AOR 2.81, 95% CI 1.505.27, P≤0.0001). Also regardless of prenatal care method, women aged 35+ years were more likely to use either sterilisation or condoms (AOR 3.37 and 11.79, 95% CI 1.03 to 10.99 and 2.5 to 55.71, P≤0.0001 and P=0.0001, respectively).
Adjusted odds ratios by multivariable logistic regression for use of contraceptive methods by Centering group prenatal care patients
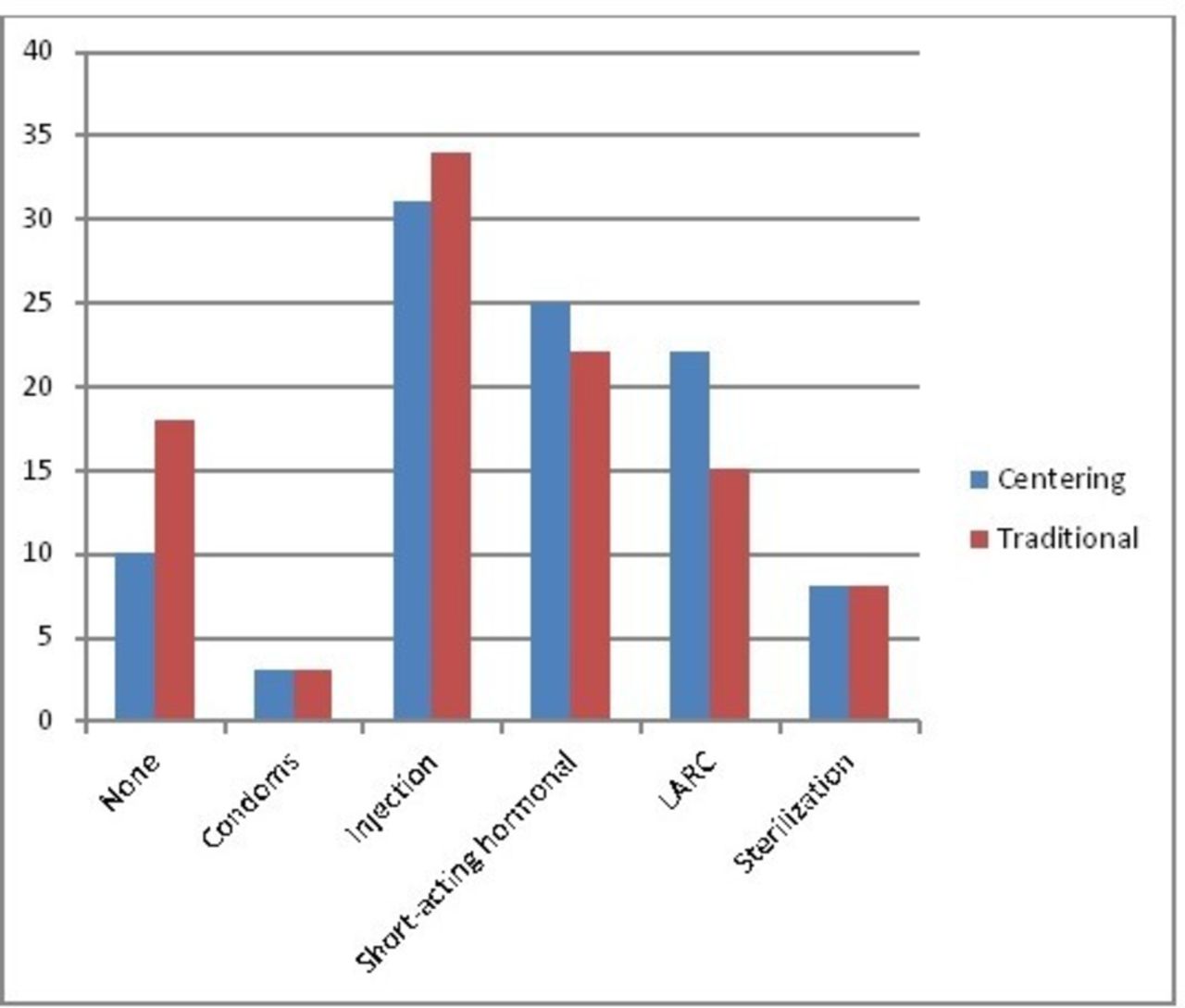
Women participating in group prenatal care were significantly less likely to not use postpartum contraception (AOR 0.50, P=0.002, 95% CI 0.32 to 0.78) when compared with those participating in traditional prenatal care (table 2). Selection of condoms, sterilisation, short-acting hormonal contraceptives, and injection were similar when comparing prenatal care models. Those in group prenatal care were significantly more likely to choose LARCs (AOR 1.67, 95% CI 1.16 to 2.40, P=0.005) than traditional prenatal care participants (table 2). The overall probability of using LARCs was 0.225 for group prenatal care patients and 0.149 for traditional prenatal care patients. Overall rates of contraceptive method use within the group prenatal care and traditional prenatal care groups are reflected in figure 2.
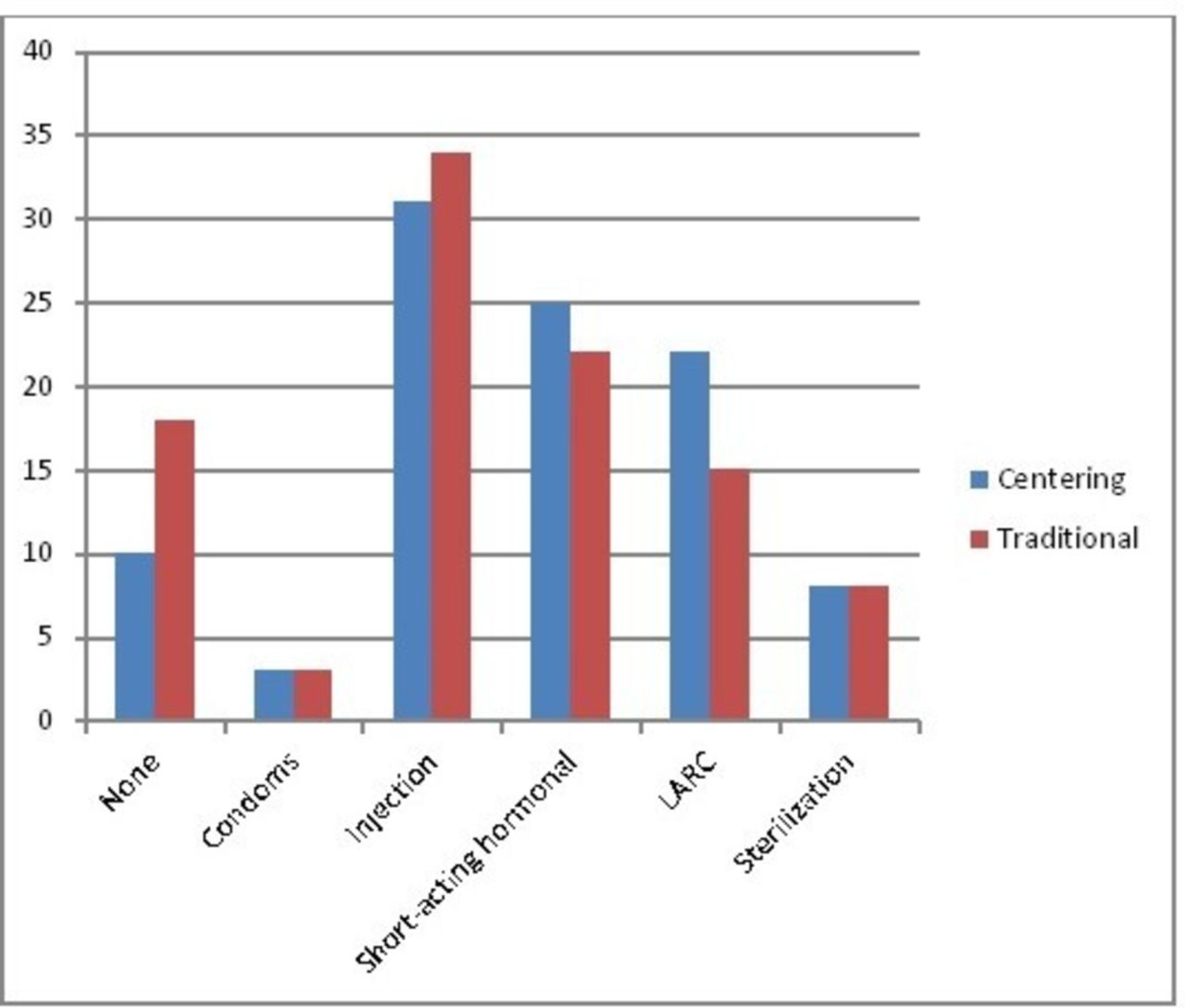
Rates (by percent of total cohort) of contraception method selection by prenatal care model. LARC, long-acting reversible contraceptive.
There was no statistical significance for any of the age group subcategories with regard to not using any method of contraception or using short-acting hormonal contraceptives. The trend toward LARC selection was most pronounced for women aged 20–24 years (AOR 1.98, 95% CI 1.10 to 3.56, P=0.023). Rates of use of each contraceptive type by age group are depicted in figure 3.

{kind=link}
{kind=link}
{kind=link}
Rates (by percent of total cohort) of no use of contraception and use of long-acting reversible contraceptive (LARC) methods by prenatal care model stratified by age group in years.
Discussion
This retrospective cohort study assessing postpartum contraceptive methods suggests that women at our institution in Newark, Delaware – a state with high unintended pregnancy rates – participating in Centering group prenatal care were more likely not only to use postpartum contraception but also to use LARCs, when compared with similar women participating in traditional prenatal care. This effect was apparent across age groups but the propensity for LARC method selection was most pronounced for women aged 20–24 years, which has been identified as an age group at high risk of unintended pregnancy.
According to the Guttmacher Institute, the 32% of sexually active, reproductive-aged women who do not use contraception consistently or correctly or who have gaps of more than a month in contraceptive use account for 95% of all unintended pregnancies.1 Postpartum women are at a high risk of inconsistent use or gaps in use. Increased postpartum contraception use by women participating in Centering group prenatal care is likely to prevent unintended pregnancies, particularly rapid repeat pregnancies.
The increased postpartum use of LARC methods by Centering group prenatal care participants is an important finding. The best way to prevent unintended pregnancy is through use of effective contraception. LARCs are the most effective forms of contraception currently available that are not permanent and do not require an operation. Women who choose LARCs tend to have high satisfaction and continuation rates.9 10 This equates to increased duration of use of very effective contraception and avoidance of unintended pregnancy, including pregnancies with short interpregnancy intervals.
There are certain aspects of the Centering model that are likely to have contributed to the findings of this study. Contraception education is incorporated into the Centering curriculum, with dedicated time for this topic included in each Centering group’s schedule. At the session including family planning, women are not only able to speak to providers about contraceptive methods but to also hear from other women like themselves who may have used certain methods in the past and/or who present important questions about other methods. It allows an open forum of communication with multiple perspectives and ideas about contraception. A majority of traditional prenatal care patients certainly do receive contraceptive counselling, but there is no consistency of content and thoroughness for all methods by all providers to all patients, and the perspectives of other women who have utilised certain methods previously are not available.
The group setting and patient-centred model of Centering group prenatal care create an atmosphere geared toward active participation. This motivates women to take a heightened interest in their pregnancy education. Active learning has long been shown in psychiatry and education research to increase the ability of learners to process and retain knowledge.11 A traditional prenatal care setting does not always allow adequate time for active patient participation in lengthy or deep discussions of educational information.
A postpartum follow-up visit is integrated into the Centering programme. This reunion time with friends made throughout the prenatal sessions is an incentive for women to return to see their healthcare provider. At that time, birth control plans can either be realised or solidified for future follow-up. In publicly insured patient populations, rates of postpartum follow-up are noted to range between just 50%–60%.12
The enhanced effects of Centering group prenatal care for women in the 20–24-year-old age group are worth noting. There are some possibilities behind this finding. There have been shifts in care provision to increasingly patient-centred models over time, making younger women more accustomed to such a style of care. Centering aligns with a patient-centred philosophy by allowing for more focus on the patients rather than physician scheduling and constraints. This age group is also culturally more inclined toward seeking out social networks through all aspects of life as social media and access to information have grown. This may make participation in group prenatal care more appealing. Younger women are also likely to have more flexible schedules and lifestyles that allow for the extended time commitment required for Centering group prenatal care appointments as compared with the short office visits generally scheduled for traditional prenatal care.
Certainly, all patients who are willing and able to take part in group prenatal care should be facilitated to do so. However, when considering the results of this study one should not assume that every patient should participate in group prenatal care. Patients with high-risk medical problems require a higher level of individualised attention. Some women would not thrive in a group setting, and it may in fact restrict their willingness to share with their provider and for that provider to garner appropriate information. The time commitment required for each session may not be practical for many pregnant women.
Rather, women’s healthcare providers should consider modifying practice to incorporate some of the beneficial aspects of group prenatal care when it comes to postpartum contraception counselling. Perhaps one prenatal care visit in each patient’s pregnancy course could be dedicated to contraception education with a standardised format. Efforts could be made to more actively engage patients in their learning. Patients could be directed to interactive contraception method education websites which include videos of everyday people who use each method. Visual and tangible examples of contraceptive methods (particularly implants and IUDs, which are less familiar to most patients) could be provided to patients. Postpartum follow-up could be incentivised to ensure adherence.
It must be considered that women who choose to participate in group prenatal care would make similar choices regardless of prenatal care model actually experienced. It is likely that such women have a heightened focus on their health, are more prone to engage in counselling in general, and have a greater tendency to comply with provider recommendations. Thus they may be more apt to not only choose to use postpartum contraception but to use more efficacious methods with or without the influence of group prenatal care.
One limitation of this study is its retrospective design. It is difficult to know what counselling practices existed, what advertisements and litigation warnings had been available to the public, and what was available during inpatient hospitalisation and in the office setting with regard to each type of contraceptive method at all time points throughout the course of the study. Extracting data from retrospective chart review is also dependent on accurate documentation. Optimally, such a study should be carried out in a prospective manner, with awareness of changing healthcare practices that may influence results and vigilance toward thorough and accurate documentation.
At our institution, leaders of group prenatal care sessions also provide traditional prenatal care. It is therefore possible that these providers already incorporated aspects of the Centering curriculum into their care of patients in the traditional office setting.
A prospective study could eliminate this crossover and more keenly identify the effects of group prenatal care. An additional benefit to a future study would be randomisation of subjects to traditional or group prenatal care. This could not be done in a blinded manner, but randomisation may be feasible in a large academic setting with a flexible patient population.
In summary, participation in group prenatal care appears to lead to higher rates of postpartum contraception use, particularly the most effective reversible methods. The propensity toward LARC use in the group prenatal care population is especially apparent for women aged 20–24 years, a high-risk group for unintended pregnancy. Future studies performed in a prospective manner – with randomisation if possible – may better define the strength of these findings.
Footnotes
Competing interests None declared.
Ethics approval Christiana Care Health System Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are on a secure database accessible by the author and Dana Thompson (data analyst).
Linked Articles
- Highlights from this issue