Article Text

Abstract
Background One in six pregnancies in Britain are unplanned. An understanding of influences on contraceptive method choice is essential to provision compatible with users’ lifestyles. This study describes contraceptive method use by age, and relationship status and duration, among women in Britain.
Methods Data from women participating in the third British National Survey of Sexual Attitudes and Lifestyles were used to describe contraceptive use grouped as: unreliable method or none; barrier methods; oral/injectable hormonal methods; and long-acting reversible contraception. A total of 4456 women at risk of pregnancy were used to examine associations between contraception use, age, relationship type and duration. Age-stratified odds ratios for contraceptive use by relationship type and duration were estimated using binary logistic regression.
Results Some 26.0% of 16–49-year-olds used hormonal contraception as their usual method. Use of hormonal and barrier methods was highest in the youngest age group and decreased with age; the reverse was true for use of unreliable methods or none. Barrier method use was higher in short-term relationships among younger participants; this was not seen among older respondents. Duration was more strongly associated with usual contraceptive method than relationship type; this pattern was more marked among younger participants.
Conclusions Asking about relationship status and duration may help providers support women’s contraceptive use by considering their priorities and preferences at different life stages. Interactions between relationship characteristics, age and contraception are complex, and bear closer scrutiny both in research and in policy and practice.
- contraception
- Britain
- relationship duration
- age
- unintended pregnancy
- relationship status
- national survey
This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Key messages
Use of barrier methods was higher in short-term relationships among younger participants, but this was not seen among the oldest respondents.
Relationship duration was more strongly associated with the contraceptive method used than was self-defined status of relationship, and this pattern was more obvious among younger participants.
Asking about partnership characteristics may help providers support women in their use of contraception by considering their priorities and preferences at different life stages.
Background
An estimated 16% of pregnancies in Britain are unplanned.1 Since contraception is available free of charge under National Health Service provision, and the prevalence of contraceptive use is high, efforts to reduce this number need to extend beyond addressing non-use. The risk of unplanned pregnancy resulting from method discontinuation has been shown to be almost as high as that resulting from no method use.2 Consequently, an understanding of influences on method choice is essential to contraceptive provision compatible with users’ lifestyles, and so less likely to be discontinued.
Studies in the United States (US) have shown both age3 4 and relationship characteristics to be more strongly associated with contraceptive method than other demographic factors.5 Contraceptive use has been associated with the number of sexual partners in Australia and Europe,6–9 the quality and level of trust in relationships,5 10 and type of relationship in Britain and the US.11–16 Other US studies and one in Britain have shown that condom use decreases with the relationship duration,11–14 17 18 while hormonal method use increases.13–16 19 Other studies have shown use of any method increases with relationship duration.10 15 18
To date, no studies using large, representative samples of women have examined how associations between method use and relationship characteristics differ by age group, or have distinguished between relationship duration and type. Further, few have taken account of fertility intentions.13 20 21 The aim of this study was twofold: first, to describe contraceptive method use among women in Britain in 2010–2012 by age group, and second, to examine associations in different age groups between type of partnership, duration of relationship, and contraceptive method use by women (reporting in 2010–2012) at risk of unintended pregnancy. The study uses data from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3).
Methods
Study design and setting
Data were analysed from Natsal-3, a cross-sectional survey of 15 162 16–74-year-old men and women living in Britain, interviewed between September 2010 and August 2012 (response rate 57.7%). The survey used a multistage, clustered and stratified probability sample. Natsal-3 data were weighted to adjust for the unequal probabilities of selection and a non-response post-stratification weight was applied.22
Natsal-3 was approved by the Oxfordshire Research Ethics Committee A (reference: 09/H0604/27).
Participants
Female Natsal-3 participants of ‘reproductive age’ (aged 16 to 49 years),23 were included in initial analyses of contraceptive method use (and stratified by age group) for whom usual contraceptive method was reported (n=5857). To explore patterns of method use by relationship type and duration by age group, we excluded those currently pregnant, trying to conceive or menopausal (n=802), those who had not had heterosexual sex in the recent time period (n=89), and participants who relied on sterilisation (n=379) (as few such women existed in the two younger age groups). We also excluded women who did not report year of both first and most recent occasions of sex with their most recent partner (n=129), or relationship status with their most recent partner (n=2). After applying these criteria, the analysis included 4456 women (online supplementary files 1 and 2).
Measures
Outcomes
The primary outcome was the contraceptive method usually used. Responses to the question ‘Which would you say is your most usual (contraceptive) method these days?’ were grouped into four categories (indicating type of method, as opposed to grouping based on effectiveness): unreliable or no usual method; barrier methods; oral/injectable hormonal; and long-acting reversible contraceptives (LARC) (figure 1). Participants were allowed to select up to three usual methods. For the 261 women who indicated use of more than one method, the most effective method reported was coded as their usual method.
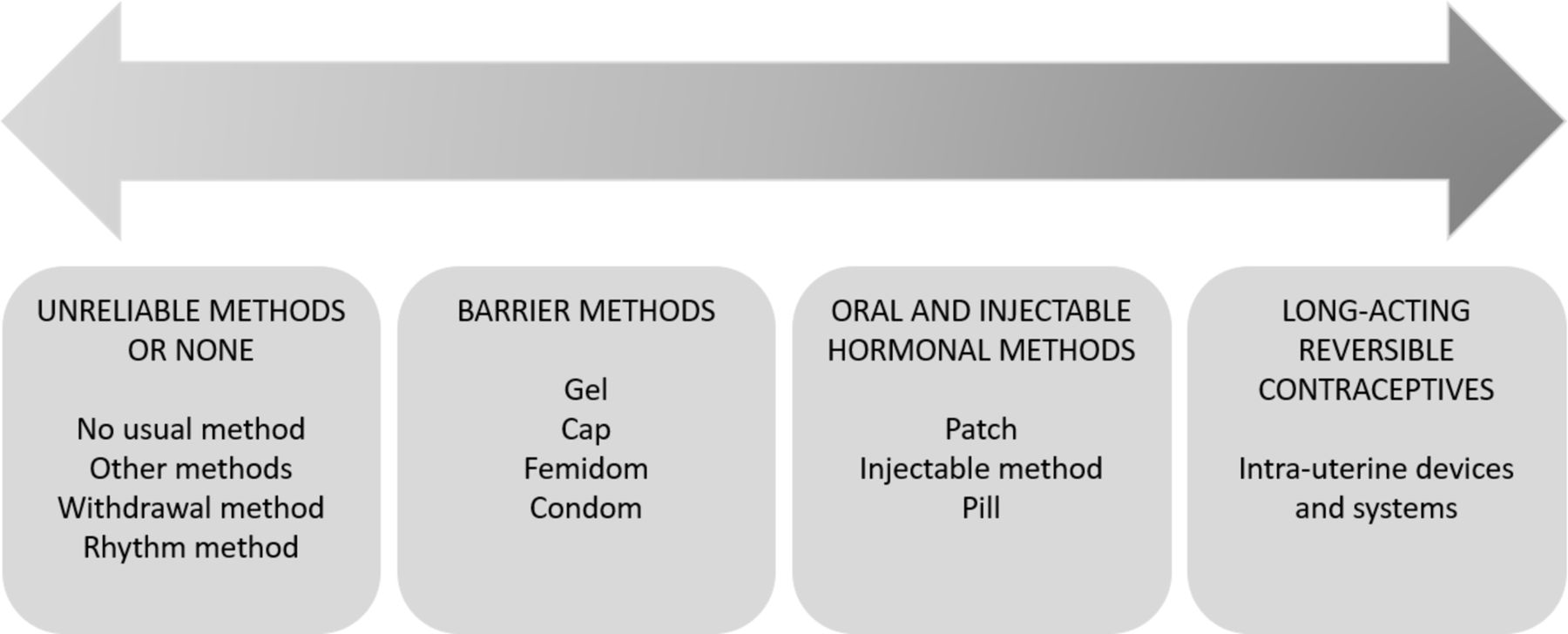
Contraceptive methods grouped by type.
Exposure variables
Relationship duration was calculated from the dates of first and most recent occasion of sex with the most recent sexual partner and grouped into mutually exclusive categories: 1 day (where the dates of first and last sex were the same); more than 1 day to 6 months; 6 months to 1 year; 1 to 3 years; 3 to 5 years; and 5 years or more.
Relationship status was derived from the question ‘Which one of these descriptions applies best to you and [that person/name] at the time you most recently had sex?’ Responses were grouped into four mutually exclusive categories: recently met, not steady, steady but non-cohabiting, married/cohabiting.
Statistical analyses
Initial analyses described the association between contraceptive method group usually used and age group (16–24, 25–34 and 35–49 years), including those with limited recent heterosexual sexual experience and those currently pregnant. From this point, further analyses were restricted to women at risk of unplanned pregnancy (those not answering ‘I would definitely like (more) children and am currently trying’ to a fertility intention question, those pre-menopausal, and those with recent heterosexual activity). A cross-tabulation of contraceptive method type usually used and relationship status and duration showed trends in method use by relationship characteristics in different age groups.
Use of each category of contraceptive method was indicated in four dichotomous variables whereby usual use of the method of interest was coded ‘1’, else ‘0’. These dichotomous variables were the dependent variables in binary logistic regression models. Initially each binary logistic regression model predicted the crude (univariable) odds of use of the method of interest by relationship status and duration, followed by mutual adjustment for both partnership characteristic variables.
Statistical analyses were performed using Stata/SE 15 (StataCorp LP) taking into account the survey’s sample design, using the svy function.
Results
Contraceptive method use among all women, by age
Table 1 shows usual contraceptive method, sexual activity and pregnancy status among all women aged 16–49 years, stratified by age group. Only 6.2% had not had sex with a man in the year prior to interview, and 15.0% were either currently pregnant, trying to conceive or menopausal, totalling 21.2% unlikely to have been at risk of unintended pregnancy. The methods most commonly used by those at risk were oral/injectable hormonal methods (26.0%), barrier methods (16.4%), and unreliable methods or none (14.8%). Use of hormonal methods was highest in the youngest age group, decreasing with successive age group. The reverse was true for unreliable and no method use, which increased with age group. Reliance on sterilisation also increased with age group and was reported by almost one in five 35–49-year-olds, but by virtually no 16–24-year-olds.
‘Usual’ contraceptive method use among women aged 16–49 years, stratified by age (column percentages)
Contraceptive method use by age and relationship characteristics among women at risk of unintended pregnancy
Online supplementary file 3 gives the distribution of women by partnership characteristics. Table 2 shows contraceptive method group use by partnership characteristics by age group (online supplementary file 4 provides the crude odds ratios and online supplementary file 5 gives additional descriptive analyses of condom use by partnership characteristics).
Supplementary file 3
Supplementary file 4
Supplementary file 5
Distribution of ‘usual’ contraceptive method use by relationship duration and relationship status, stratified by age
16–24-year-olds
Unreliable and no method(s)
Less than 10% of 16–24-year-olds at risk of unintended pregnancy were using an unreliable or no contraceptive method. This proportion did not vary consistently by relationship status but decreased significantly with duration. After adjustment for relationship status and duration, the association between use of an unreliable method or none and relationship duration remained significant, but the association with relationship status was weakened (figure 2A and online supplementary file 6).
Supplementary file 6

{kind=link}
{kind=link}
Forest plots of adjusted odds ratios for use of each group of contraceptive methods, by relationship duration and relationship status. A: 16–24 years; B: 25–34 years; C: 35–49 years.
Barrier methods
Barrier method use was reported by one in four women at risk of unintended pregnancy, but decreased significantly as relationships increased in length and became more established. After adjustment, the odds of barrier method use were only significantly lower for women in relationships lasting 1 to 3 years' duration, and among women in steady or married/cohabiting relationships.
Oral and injectable methods
Hormonal method use accounted for over half of usual use by women at risk of unintended pregnancy. Use was highest among women in relationships of 1 to 3 years' duration and those in ‘steady’ relationships. Adjusted odds showed significant increased use of oral/injectable methods in relationships lasting between 6 months and 3 years, as well as among steady, non-cohabiting couples.
LARC
The proportion of women using LARC did not vary with relationship duration nor status in this age group, and this was confirmed in the adjusted logistic regression results.
25–34-year-olds
Unreliable and no method(s)
Almost one-fifth of women in this age group used an unreliable or no method. This proportion increased with relationship duration but not status. Adjusted results showed a significant decrease in use of unreliable methods or none for all relationships lasting longer than 1 day (with the exception of relationships of 6 months to 1 year) (figure 2B).
Barrier methods
Almost one-quarter of women at risk of unintended pregnancy usually used a barrier method. This proportion did not vary significantly by relationship characteristics. After adjustment, only women whose most recent relationship lasted between 3 and 5 years were less likely to report use of barrier methods.
Oral and injectable methods
The proportion of women reporting oral/injectable method use increased with relationship duration but did not vary significantly by status. After adjustment, use of these methods significantly increased with relationship duration, but notably, decreased with relationship stability. Women whose most recent relationship had lasted only 1 day were less likely than other women to use hormonal methods, but women who said they had recently met their partner were more likely than married/cohabiting women to have used such methods.
LARC
There were no significant associations between use of LARC and relationship duration or status.
35–49-year-olds
Unreliable and no method(s)
Some 38.1% of women in this age group reported usual use of an unreliable or no method. This proportion varied by relationship status but not duration. Adjusted odds ratios showed women who had recently met their partner were less likely to use an unreliable or no method (figure 2C).
Barrier methods
Use of barrier methods varied with neither relationship status nor duration.
Oral and injectable methods
The adjusted odds of using an oral or injectable method were not significantly associated with relationship status nor duration.
LARC
Use of LARC varied significantly by relationship status, but not duration. After adjustment, women who had recently met their partner were significantly more likely to use LARC than women in other types of relationship.
Discussion
Principal findings
These data from a nationally-representative survey of sexually-active women in Britain illustrate differences in method use by the nature and duration of the relationship with the most recent sexual partner and how the extent of these differences varies with age. Use of barrier methods was appreciably higher in short-term than longer-term relationships among younger participants, but this pattern was not seen among respondents in the oldest age group. While there was considerable correspondence between the duration and type of relationships and their association with contraceptive method use, some differences were observed. Relationship duration was marginally more strongly associated with the contraceptive method used than was relationship type, and this pattern was more obvious among younger participants. Moreover, relationship type and duration operated differentially in their influence on hormonal method use among 25–34-year-old women.
Comparison of our findings to those of other studies is difficult because of differences in methodology, in the definition of relationship types and in the categorisation of contraceptive methods. Typically, studies that have compared contraceptive method use in different age groups,4 24 have not taken relationship characteristics into account and, conversely, studies that compared contraceptive method use by relationship characteristics have not done so in different age groups.6–10 13 14 16 25 These differences in study design are likely to partially explain the equivocal nature of findings of many previous studies14 and also apparent anomalies between other studies and our own. At the aggregate level, we did not find higher levels of LARC use among younger participants than older ones, as others have.26 27 Nevertheless, their use increased markedly among 16–24-year-old women whose relationship had lasted 5 or more years; equivalent to the prevalence among 35–49-year-olds.
Study strengths and weaknesses
Our large population-based dataset enabled us to estimate the prevalence of contraceptive use in different age groups by relationship type and duration, and to exclude women not apparently at risk of unplanned pregnancy. The study also has limitations. For multi-partnered participants, cross-sectional data are unsuited to tracing pathways of use and consequently we have made several assumptions in this article. First, we have assumed that respondents used their ‘usual’ method of contraception with their most recent sexual partner. When respondents reported several usual methods, the most effective may not have been the method used for the most recent sex. Second, the most recent sexual partner may not have been the main sexual partner during the previous year. Relationship duration was calculated objectively as the time between first and most recent sex with the respondent’s most recent sexual partner. This measure might not truly reflect relationship duration as it would be defined by the participant. We restricted our analyses to women, as misreporting of usual contraceptive method may be more common by men, since the majority of the methods are operationalised by women. We were limited to use of data generated by the questions asked in Natsal-3, which did not probe affective attributes of the relationship which others have linked to contraceptive method use.5 10 Finally, while we have no reason to believe contraceptive practices might have changed in the time since interview, these analyses are based on data reported by participants up to 8 years ago.
Implications for policy and practice
Our data should be interpreted in the context of women’s lives, and their evolving priorities and preoccupations through the life course. Younger women, and those in more transient relationships, may be more motivated to avoid pregnancy than those who are older and in more stable relationships. Thus, the fact that one in six 16–24-year-olds uses an unreliable/no method of contraception with a partner they have just met is of concern. So, also, is the relatively low prevalence of reliable method use in shorter-term relationships among older participants. Alternatively, it is likely that although not explicitly trying to conceive, for some women a pregnancy would not be unwelcome, resulting in some ambivalence in relation to contraceptive use.28 An acknowledgement of pregnancy intention as a continuum is important to further understand women’s contraceptive needs. To date, sexual health policy remains focused on younger adults, but evidence that the majority of unplanned pregnancies occur among women aged 25 years and over,1 has prompted pleas for age-specific health promotion strategies.29 30
The independent associations of relationship type and duration with method use, and the suggestion that duration might be the stronger influence, has implications for policy and practice. Conventionally in clinical record-taking, data are collected on relationship type. Our findings suggest that there are benefits to be gained from asking about relationship duration in helping support women in their use of contraception, to help them consider their priorities and preferences at different life stages. Our findings highlight the complex nature of associations between age, partnership characteristics and method use, and signify that every woman needs to be assessed individually.
Future research
Future research should recognise that the associations between relationship characteristics and contraceptive method use are more complex than might be suggested from aggregate data often used to assess the need for health promotional messages and public health interventions. Studies need to take account of both age and the nature of the relationships in which women use contraception.
Supplementary file 1
Supplementary file 2
Acknowledgments
Natsal-3 was a collaboration between University College London (London, UK), the London School of Hygiene and Tropical Medicine (London, UK), NatCen Social Research, Public Health England (formerly the Health Protection Agency), and the University of Manchester (Manchester, UK). The authors thank the study participants; the team of interviewers from NatCen Social Research; Heather Wardle, Vicki Hawkins, Cathy Coshall, and operations and computing staff from NatCen Social Research; and Professor Carol Dezateux at UCL GOS ICH for writing assistance.
References
Footnotes
Contributors NF analysed and interpreted the data. NF, MJP, IMT and KW were major contributors in writing the manuscript. All authors read and approved the final manuscript.
Funding Natsal-3 was supported by grants from the Medical Research Council (G0701757) and the Wellcome Trust (084840), with contributions from the Economic and Social Research Council and Department of Health. NF was supported by a UK/EU Fees Studentship Award for her MSc in Demography & Health at LSHTM. All research at Great Ormond Street Hospital NHS Foundation Trust and UCL Great Ormond Street Institute of Child Health is made possible by the NIHR Great Ormond Street Hospital Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests None declared.
Patient consent Not required.
Ethics approval The Natsal-3 study was approved by the Oxfordshire Research Ethics Committee A (reference: 09/H0604/27). Participants provided oral informed consent for interviews.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data that support the findings of this study are available from the Natsal research team but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the Natsal research team.
Linked Articles
- Highlights from this issue