Article Text

Abstract
Background Health professionals are challenged by a growing number of young long-term cancer survivors with their specific needs with regard to family planning. This study aimed at assessing decisional conflict (DC) in young female cancer patients regarding fertility preservation, identifying demographic, fertility and fertility preservation related factors, which may affect DC, and assessing the helpfulness of various decision-supports.
Methods A retrospective, cross-sectional, web-based survey via an online questionnaire available in three languages with specific items concerning cancer, fertility, fertility preservation and the validated Decisional Conflict Scale targeted at current or former female cancer patients aged 18–45 years, with cancer types or treatment potentially affecting reproductive function.
Results The 155 participating women showed considerable DC, especially with regard to missing information and support. DC was significantly lower in patients when the risk of infertility was discussed with a health professional, when they had undergone any procedure to preserve fertility, and when they had a university education. A longer time interval since cancer diagnosis was associated with higher DC. The most helpful decision-support tools were specialised websites and leaflets.
Conclusions Young female cancer patients’ DC with regard to fertility preservation is very high. Information and support seem to be deficient. More information through standardised information tools might be an effective strategy to lower their DC at the time when treatment decisions need to be taken, and to improve their reproductive health after they have overcome cancer in the future.
- fertility preservation
- decisional conflict
- decision-making
- cancer survivor
- reproductive health
Statistics from Altmetric.com
Key messages
Decisional conflict (DC) in young female cancer patients on whether or not to undergo any fertility preservation procedures is high.
Lower DC was associated with having discussed the risk of infertility with health professionals, with having undergone a fertility preservation procedure and with having attended university.
In addition to discussion with partners and physicians, leaflets and specific websites were considered as helpful sources of support for decision-making.
Introduction
Advances in cancer detection and treatment have led to a significant increase in survival of young cancer patients so that maintaining a high quality of life after successful therapy is of great importance.1 Fertility and the ability to give birth are important factors determining good quality of life of young female cancer survivors.2 3 However, cancer treatment often compromises fertility and debars cancer survivors from childbearing. In order to meet these individuals' needs and rights with regard to planning for a family, women of reproductive age facing gonadotoxic treatment require comprehensive care that takes their future fertility into consideration. Currently available methods to preserve fertility before gonadotoxic therapy are essentially based on suppression of ovarian function, cryopreservation of gametes or ovarian tissue, and fertility-sparing surgery.4 In particular, cryopreservation of oocytes and embryos are well-established methods. For both options, ovarian stimulation is required which may lead to a delay in cancer treatment. For those who require urgent initiation of cancer therapy, ovarian tissue cryopreservation is increasingly being offered as an alternative or in addition.5 6
The choice of the best method to preserve fertility and the estimation of risk and benefit is a complex process and confronts young female cancer patients with additional decisions that have to be made.1 7 Furthermore, these decisions have to be made in the short time period after cancer diagnosis and before the start of therapy. As a consequence, decisional conflict (DC) may occur.
DC is a state of uncertainty about an action.8 Uncertainty is more common in decisions which involve risks, unclear outcomes, significant potential benefit or damage.8 Decisions about whether or not to undergo a fertility preservation procedure before cancer treatment are very complex, and in order to reduce DC for future patients, more information is required. The objectives of the present study were therefore (1) to assess DC regarding fertility preservation in young female cancer patients, (2) to identify demographic, cancer, fertility and fertility preservation related factors affecting DC and (3) to weigh the relative helpfulness of various options for support in decision-making.
Methods
Study design
We conducted a retrospective, cross-sectional, web-based survey investigating issues around fertility and fertility preservation. The present data were collected as part of a larger research project about fertility issues in cancer patients based at a Swiss and a British study centre.7 9 10
Participants
The target group were current or former female cancer patients meeting the following inclusion criteria: 18 years or older at the time of the study participation, experience of a cancer diagnosis in their fertile lifespan (under the age of 45 years) and a cancer treatment having the potential to affect reproductive function.
Recruitment procedure
Participants were recruited online via several cancer and fertility websites. In a first phase conducted by the British study centre, the survey was published on 12 English language websites. In a second phase, a German and French version of the survey was developed at the Swiss study centre and published on a total of six websites. All participants signed an electronic informed consent before starting the questionnaire and before submitting the answers. All personal identifiers were removed or disguised so that the persons described were not identifiable and were not to be identified through the details of their story.
Measures
The Cancer and Fertility Survey (CFS) is a questionnaire that was developed specifically for this project and is described in detail elsewhere.9 To guarantee congruence of the questions in all languages, the English version was translated and retranslated into German and French according to standardised criteria. The web survey was produced using the online tools ’SurveyTracker'11 in the UK and '2ask'12 in Switzerland, respectively.
Cancer, fertility and fertility preservation related data
Participants stated their expectation of their chances of being cured of their cancer on a 10-point Likert scale that had been developed especially for this survey and that ranged from 1 (not at all hopeful) to 10 (extremely hopeful). The need for parenthood was assessed using the three-item need for parenthood scale,13 of which the items were rated on a five-point response scale ranging from 1 (strongly agree) to 5 (strongly disagree).
Decisional Conflict Scale
DC about fertility preservation was measured with the validated Decisional Conflict Scale (DCS).14 Four items concerning ‘effective decision’ of the original 16-item scale were excluded because not all participants had yet made a decision about fertility preservation. The modified version of the DCS thus consisted of the four subscales ‘uncertainty’, ‘informed’, ‘value clarity’ and ‘support’. Higher scores indicated a higher DC with a range from 0 (no DC) to 100 (extremely high DC). A score >37.5 indicates high DC, while scores between 25 and 37.5 indicate moderate DC and scores <25 low DC.14
Decision-support
Participants were asked to indicate from a list of decision-supports which type they used and with which persons they discussed their decision. On a five-point response scale from 1 (not at all helpful) to 5 (extremely helpful), participants indicated how helpful the support of a distinct tool or person was.
Data analysis and statistics
Statistical Package for Social Science (SPSS, version 22.0.0. Armonk, New York, USA: IBM Corp.) was used for all analyses. Associations between DC scores and demographics, cancer and fertility factors, as well as fertility preservation characteristics, were calculated. The items concerning decision-support were weighted by calculating a weighted helpfulness index (percent used x helpfulness rating). The two subsamples (British and Swiss) did not differ significantly with regard to demographic and medical variables (data not shown). Therefore, data were merged for statistical analysis. Missing data from unanswered questions of individual participants (8.26%) was not replaced. For the purpose of analyses, the direction of the need for parenthood scale was reversed in order to range from 1 (strongly disagree) to 5 (strongly agree). Descriptive statistics were calculated as frequency and percentage for categorical data, means and SD for continuous data. The Kolmogorov-Smirnov test was used to check normal distribution of the interval scaled data of the DCS. Analysis of Variance (ANOVA) and Pearson correlation were used for calculation of differences or associations between DC scores and variables listed in table 1. For analysis of differences between DC scores and DC subscales or between decision supports ANOVA was used. Multiple linear regressions were conducted. A value of P<0.05 was considered as statistically significant.
Associations between decisional conflict and demographic, cancer, fertility or fertility preservation characteristics
Results
Demographic, cancer, fertility and fertility preservation related data
A total of 155 women took part in the online survey. The mean age at diagnosis was 31.27 (SD 6.94) years and 73.6% (89) of the participants were younger than 35 years. Education was high, with a university degree in 53.0% (79) of the participants. The majority of the participants (78.2%, 115) were living in a relationship and 69.5% (105) had not given birth yet. On average, women answered the questionnaire 4.47 (SD 4.69) years after diagnosis. With 44.0% (66) of all participants, breast cancer was the most frequent cancer diagnosis. Participants rated their hopefulness to be cured with 7.33 (SD 2.09) points on the 10-point scale. The need for parenthood was strong, with a mean of 4.30 (SD 0.89) points on the five-point scale. In total, 74.7% (109) of the participants indicated that a health professional had spoken to them about how cancer or its treatment would affect their fertility and 29.9% (44) had undergone a fertility preservation procedure.
Decisional conflict
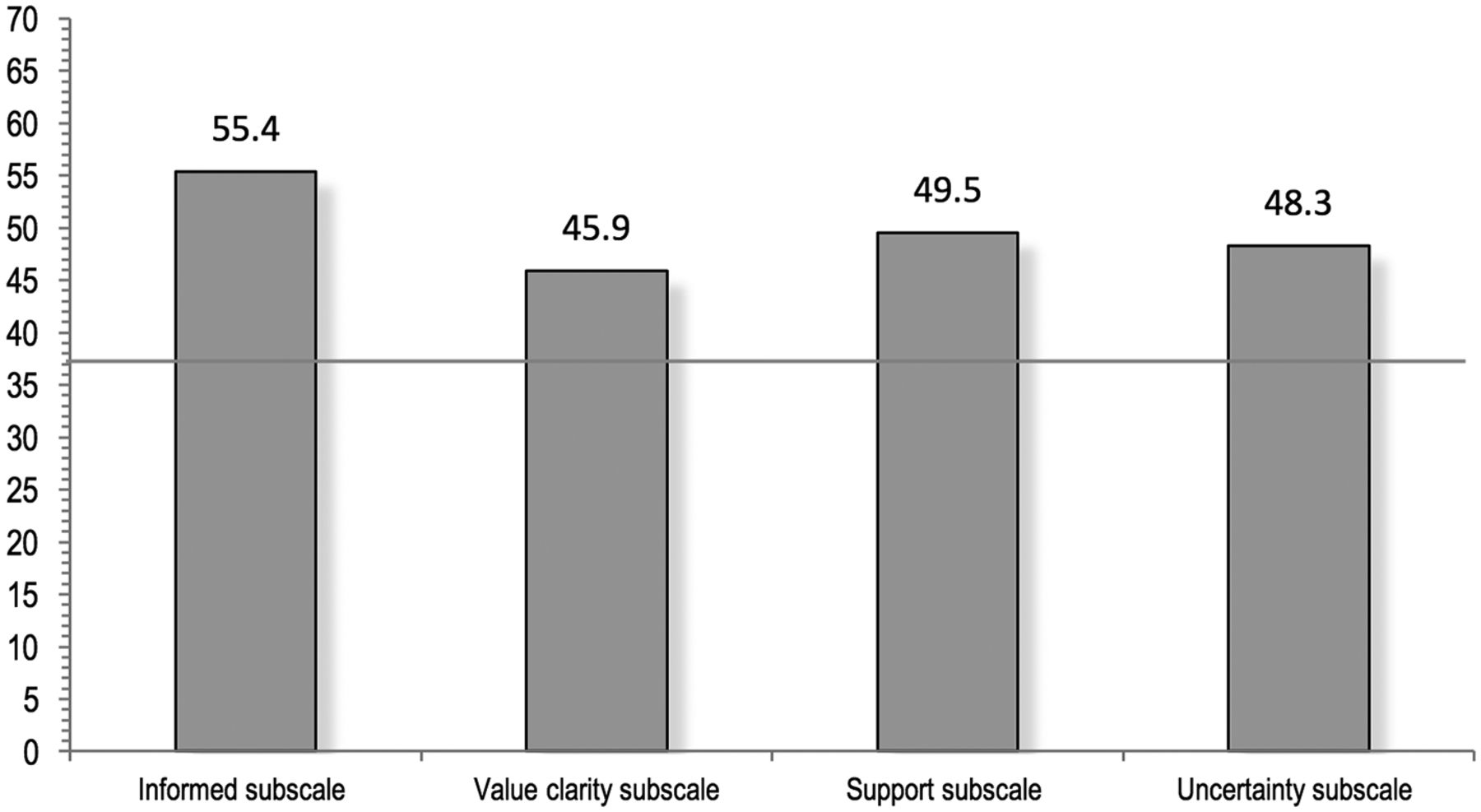
Mean DC was 50.13 (SD 30.73) out of 100 possible points. In total, 62.7% (89) of the participants showed a high DC by definition. DC subscale scores are shown in figure 1. In within-subject ANOVA, the between DC subscales were not significant.
{kind=link}
Mean subscale scores of the Decisional Conflict Scale (DCS). Range from 0 (no DC) to 100 (extremely high DC). Scores >37.5 indicate a high DC.
Associations with decisional conflict
Associations between DC and demographic, cancer, fertility and fertility preservation characteristics are shown in table 1. In the final linear regression model, the significant associations in the initial analysis remained significant (fertility preservation undergone (P<0.001), health professional informed about cancer or treatment affecting fertility (P<0.004), university education (P<0.020), years since diagnosis (P<0.024)).
Decision-support
Participants most frequently approached their physicians (n=85, 53.8%) or partners (n=79, 50.0%) for support during the decision-making process. From the given choice of supportive media, specialised websites were indicated most often (n=47, 29.7%). A detailed list of all decision-supports is presented in table 2. Discussion with partner showed the highest weighted helpfulness index, but according to statistical analysis (ANOVA) there was no difference compared with discussion with family or physician and there was no significant difference between weighted helpfulness of leaflets and websites either.
Percentage of women who used each decision-support, helpfulness rating and weighted helpfulness of each decision-support
Discussion
In this study we investigated DC in young female cancer patients concerning whether or not to opt for fertility preservation before cancer treatment. We could demonstrate that women in our sample had significantly high DC regarding their decision. Higher DC was associated with more years of survivorship, while lower DC was seen in women who had been informed about the possibility to preserve fertility by a health professional and who had undergone such a procedure. Furthermore, it was shown that online material and leaflets were the most frequently used decision-support tools.
Decisional conflict concerning fertility preservation
With an average DC of 50.13 (SD 30.73) and a majority of women showing characteristics of a high DC (62.7%), our findings are consistent with previously published results. Peate et al examined a decision-aid in breast cancer patients and showed an average DC of 48.3 with 63.1% of participants having a high DC.15 Mersereau et al determined a DC of 41.1, and 55.3% of their sample of female cancer survivors had a high DC.16
Examination of DC subscale scores indicates that patients have a strong feeling of being uninformed (subscale score of 55.4) and not being supported (subscale score of 49.5) at the time of decision-making. In contrast, the sample examined by Peate et al showed high uncertainty and lack of value clarity.15 However, in their study the feeling of being supported was stronger with a subscale score of 35.9. That participants felt better informed and supported might be due to the fact that Peate et al were evaluating a decision-aid in this study.15
Associations with decisional conflict
Our retrospectively evaluated data showed a higher DC at time of diagnosis in women with longer duration of survivorship. Considering the recent advances in various methods to preserve fertility we might assume that patients with a longer interval since cancer diagnosis had fewer options and there was less focus on this issue in the context of cancer therapy. Over time, priorities may shift from treating the cancer to fertility and the ability to give birth. This would be in line with a study that suggests that after some years there is a stronger consideration of late effects of the treatment and priorities shift from cancer treatment to quality of life in a long-term survivorship.16
Additionally, we found significantly lower DC in patients who had had a discussion about risk of infertility with a health professional, supporting research that showed that referral to a specialist in reproductive medicine is associated with a significantly lower DC.16 In general, specific information provision and thus an increase in knowledge suggest reduction of DC.15 17 Young female cancer patients in particular would like to have as much information as possible15 and many of them actively ask for information.18 Thus, irrespective of the individual situation and circumstances, healthcare professionals should not refrain from informing all patients about the negative consequences of cancer treatment on fertility and the possibilities to mitigate those consequences.
Moreover, participants who underwent a procedure to preserve fertility had a significantly lower DC compared with those who did not. This is consistent with recent studies with a similar focus.16 19 It is likely that women who had had such interventions will have had specialist consultations beforehand, which would have enabled them to make a more satisfying choice.
Even if it is repeatedly highlighted that being informed is crucial for decisional satisfaction, 25.3% of our sample had not discussed the risk of infertility with any health professional. Another study showed that more than half of the referrals to a fertility specialist were actively requested by patients and not suggested by oncologists.19 These data suggest that women still do not receive appropriate support around future fertility.
Helpful strategies to lower decisional conflict
Regarding helpful media for decision-support, the participants preferred specialised websites (29.7%) and leaflets (24.7%). These were considered to be moderately to very helpful. In the study of Kim et al, cancer patients rated hand-outs as very much or somewhat helpful and the internet was the most frequently used resource before fertility preservation consultation.19 Furthermore, a study showed that participants had improved knowledge after having used specialised websites.17 A Cochrane review showed high-quality evidence that support-tools, namely decision-aids, improve patients’ involvement and realistic perception of outcomes.20 Since many studies were able to show a decrease in DC with the use of decision-aids,15 20 an effort towards improved information provision through appropriate decision-support tools seems to be indicated. The results of the pilot phase of a German decision-aid currently under evaluation are promising.21
Study limitations
Some limitations need to be taken into account. We asked women retrospectively about their experience concerning decision-making, but these were recollections of the cancer experience because not all women were in the midst of making that decision. In our study, the time period in question — directly after diagnosis — was about 4 years back for most of participants. This might introduce a recall bias. Due to the fact that the online recruitment was based on self-registration by interested participants, selection bias might not be negligible. The level of uncertainty about decision might be higher in women searching for information online. Moreover, online acquisition typically appeals to a better-educated population.9 22 23 The accuracy of medical data could not be checked as it was uniquely based on information provided by the participants. However, despite these biases our results were similar to those of other studies.
Conclusions
In summary, fertility is important for young cancer survivors and has a long-term impact on their quality of life. Years after cancer diagnosis, DC concerning fertility preservation was high and might even be higher than directly after diagnosis when cancer treatment is the pressing concern. Health professionals can lower DC of female patients with adequate information about options to preserve fertility. Appropriate information to all women diagnosed with cancer in their fertile lifespan regardless of age, partnership status or parity is warranted so that every cancer patient is able to make an informed decision. In addition, informative and helpful decision-support tools are needed. The identified factors modifying DC should be taken into account when developing decision-aids for young female cancer patients.
References
Footnotes
Funding This study is financially supported by the Swiss Cancer League (KFS 3584-02-2015) and by the Swiss Bridge Foundation (Swiss Bridge Award 2013).
Competing interests None declared.
Ethics approval The ethical committee of the School of Psychology Cardiff gave approval for the first part of the survey and the ethical committee of Northwest and Central Switzerland (EKNZ) for the second part.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue