Article Text

Abstract
Aim This review summarises the available data on the disadvantages of the 7-day contraceptive-free interval (CFI) of combined oral contraceptives (COCs), in contrast to shorter CFIs or continuous use – including flexible regimens – and provides recommendations for practice.
Methods Relevant papers were identified by Medline and PubMed. The final reference list was generated on the basis of relevance to the review, with priority given to systematic reviews and randomised controlled trials.
Results There is considerable inter- and intra-individual variation in the absorption and metabolism of COCs. Even with perfect use, the loss of endocrine suppression during the standard 7-day CFI allows follicular development with the risk of escape ovulation in a vulnerable minority. This risk increases in typical users whenever the CFI is prolonged: late restarts are a common reason for pill omissions. Shortening or eliminating the CFI improves contraceptive efficacy using the lowest doses available, without evidence to date of compromised safety.
Conclusions There is no scientific evidence to support a 7-day CFI and it should be replaced either by a continuous flexible regimen, or extended regimens with a shortened CFI, prescribed first-line. In women preferring a monthly ‘bleed’, a 4-day CFI similarly provides a greater safety margin when pills are omitted.
- hormone-free interval
- continuous regimen
- extended regimen
- flexible regimen
- combined oral contraceptives
- hormonal contraception
Statistics from Altmetric.com
- hormone-free interval
- continuous regimen
- extended regimen
- flexible regimen
- combined oral contraceptives
- hormonal contraception
Key messages
Extension of the contraceptive-free interval (CFI) because of pill omissions is the most likely reason for the order-of-magnitude difference in efficacy between ‘perfect’ and ‘typical’ combined oral contraceptive (COC) users.
Continuous/flexible regimens, with short discretionary pill-breaks to alleviate unwanted bleeding, increase the safety margin for common pill omissions yet permit the lowest available dosage.
Eliminating or reducing CFIs has demonstrable advantages including fewer days of bleeding per year and reduction of menstrual pain, headaches, and the possible need for emergency contraception.
Introduction
The combined oral contraceptive pill (COC), devised in the 1950s by Gregory Pincus together with the gynaecologist John Rock and other pioneers, was initially approved for menstrual regulation. But it was also a unique contraceptive, using synthetic versions of women’s own sex hormones to inhibit ovulation. To make the method seem as ‘natural’ as possible, women were instructed to stop the hormones for one week out of every four to create a withdrawal bleed. This 7-day interruption in ovarian suppression was not based on scientific evidence but primarily on the belief that women would find a monthly bleed reassuring. Indeed, Pincus recognised that “in view of the ability of this compound to prevent menstrual bleeding as long as it is taken, a cycle of any desired length could presumably be produced".1
The subsequent reduction in daily dose of ethinylestradiol (EE) from 150 µg to 10–35 µg has significantly reduced the frequency of adverse events, especially thromboembolism. But the potential downside is an increased risk of contraceptive failure,2 particularly as a consequence of that 7-day contraceptive-free interval (CFI), a term we prefer to ’pill-free interval' (PFI) since it highlights this as comprising the days when the woman is instructed to omit her contraceptives.
The objective of this review is to summarise the data on the benefits and risks of shorter CFI and continuous-use regimens, compared with the 7-day CFI, and to provide recommendations for practice. The rarity of true method-failures of the 21/7 COC means that they are of little public health importance, but that is not the case for ‘user-failures’ which are experienced by up to 9% of ‘typical’ COC users in the first year compared with 0.3% of ‘perfect’ users.3 Here we review ovarian activity and follicular development in the CFI as surrogate measures of pregnancy risk, and go on to argue for continuous/extended regimens to replace the 21/7 regimens.
Methods
Publications for this review were identified by searches of Medline and PubMed between 1 January 1955 and 1 December 2017. The search terms ‘oral contraceptives’, ‘oral contraception’, ‘continuous regimen’, ‘extended regimen’, ‘flexible regimen’, ’missed pills’ and ‘pill-free interval’ were used. The final reference list was generated on the basis of relevance to the review, with priority given to systematic reviews and randomised controlled trials (RCTs).
Contraceptive regimens currently used
A number of regimens for marketed COCs are currently in use, with or without placebos during the CFIs. The standard 28-day cycle of 21 active pills followed by a 7-day CFI (21/7) is by far the most common regimen, followed by a 28-day cycle with shortened CFI (typically 24/4). Other regimens that are licensed in some countries, but not as yet in the UK, include extended cycle (typically 84/7) and continuous use (365/0).
The commonly used regimens that are unlicensed in the UK include extended cycle (typically 63/7 or 84/7) and continuous flexible (or ‘tailored’) use, in which there is the option for a continuous COC user to take a 3- to 4-day break, usually triggered by, and to manage, unacceptable bleeding.
Contraceptive effectiveness
Effectiveness of the different regimens can be evaluated by pregnancy rates as well as by surrogate measures including ovarian activity, risk of escape ovulation and cervical mucus quality.
Contraceptive failure and pregnancy rates
There have been few RCTs of COCs with pregnancy as an endpoint and they have been underpowered,4 due to the high efficacy of all COC regimens in research volunteers who are, in general, correct and consistent users. Exceptionally, there is one RCT of a 50 µg EE/250 µg levonorgestrel (LNG) COC, administered vaginally, comparing a 21/7 regimen (n=454) with continuous use (n=446), which reported four pregnancies (1.04%) in the cyclical group and none in the continuous use group (OR 0.1, 95% CI 0.02 to 0.97).4 5
Observational studies are more representative of ‘typical’ users. They concur that non-compliance risks pregnancy,6–8 yet no study has obtained the data to link that risk to the timing of tablet omissions in relation to the 7-day CFI. Moreover, there are no reports to date that confirm, or refute, that the risk due to non-compliance is any lower with 84/7 extended regimens. In the one open-label parallel RCT comparing the efficacy and safety of 30 EE/150 LNG, the Pearl Index based on method failure for the 84/7 regimen (n=456) was 0.60, which was lower than the Pearl Index of 1.78 for the 21/7 regimen (n=226), but the authors did not include tests for statistical significance.6 Prospective observational studies of conception rates for the standard 21/7 regimen versus the 365/0 continuous flexible regimen described below are likewise still awaited.
With respect to regimens with a shorter (4-day) CFI, contraceptive effectiveness comparing progestogens and regimens in ‘typical’ users was specifically addressed in a subgroup analysis of outcome data from a prospective cohort study of 52 218 US women who were using 24/4 and 21/7 regimens of COCs containing differing doses and types of progestogens and differing doses of EE.9 During 73 269 woman-years there were 1634 pregnancies of which 1405 (86%) were associated with non-compliance. The analysis specifically focused on the effect of the 24/4 versus 21/7 regimen, particularly comparing drospirenone (DRSP) with other progestogens, on the basis that drospirenone has a longer half-life. The overall Pearl Index was 1.6 (95%CI 1.4 to 1.9) for a 20 EE/3000 DRSP 24/4 regimen, 2.2 (95%CI 1.8 to 2.6) for a 30 EE/3000 DRSP 21/7 regimen, and 2.6 (95%CI 2.4 to 2.7) for all other pills. Direct comparisons within the DRSP and norethisterone acetate (NETA) groups (excluding pills with other progestogens) showed significantly lower contraceptive failure rates for 24/4 versus 21/7 regimens, and significantly lower contraceptive failure rates for DRSP versus NETA: life-table estimates of the rates of contraceptive failure for the first year of pill use were 2.1% for the 20 EE/3000 DSRP 24/4 regimen, 2.8% for the 30 EE/3000 DRSP 21/7 regimen, 3.5% for an EE/NETA 24/4 regimen, and 4.7% for an EE/NETA 21/7 regimen. While interpretation of these results is subject to the limitations of observational research, the trend is in line with the greater efficacy associated with the 24/4 regimen versus 21/7, despite the lower EE dose. The benefits of the 24/4 regimen were more pronounced and statistically significant in adolescents. In a subgroup analysis of 228 unintended pregnancies in adolescent participants using any 20 EE pills in the same study, the Pearl Index was 2.5 (95%CI 2.1 to 2.9) for the 24/4 regimen and 5.1 (95%CI 3.7 to 6.8) for the 21/7 regimen.10
Ovarian activity and risk of escape ovulation
Smith et al 11 showed that ovarian estradiol levels are routinely suppressed once seven COC tablets have been taken. Yet in their Group 1 subjects, who discontinued for 7 days after taking seven daily tablets, one woman out of 12 showed luteinisation, with a rise in plasma progesterone level to 6.8 nmol/L. This would suggest that the risk of ovulation would only arise in mid-packet by omission of seven tablets. Indeed, after prior ingestion of seven pills there appear to be no documented ovulations in the literature, nor pill-failure conceptions established as occurring through omissions of fewer than seven tablets. In the systematic review by Zapata et al,12 missing up to four consecutive pills on days not adjacent to the pill-free interval resulted in little follicular activity and low risk of ovulation.
A review of 29 studies evaluated pituitary-ovarian activity in women using 20–40 µg EE COCs.13 In 20 studies, follicles ≥10 mm diameter were identified by Day 7 of the CFI on ultrasound, the cut-off during natural menstrual cycles for selection for preferential growth and ovulation. Although most dominant follicles regress when COC are restarted, 10 studies reported ovulation. In two RCTs of 21/7 regimens, one pregnancy was reported as method failure in a woman taking 20 EE/150 DSG14 and another in a woman taking 30 EE/1500 NETA.15
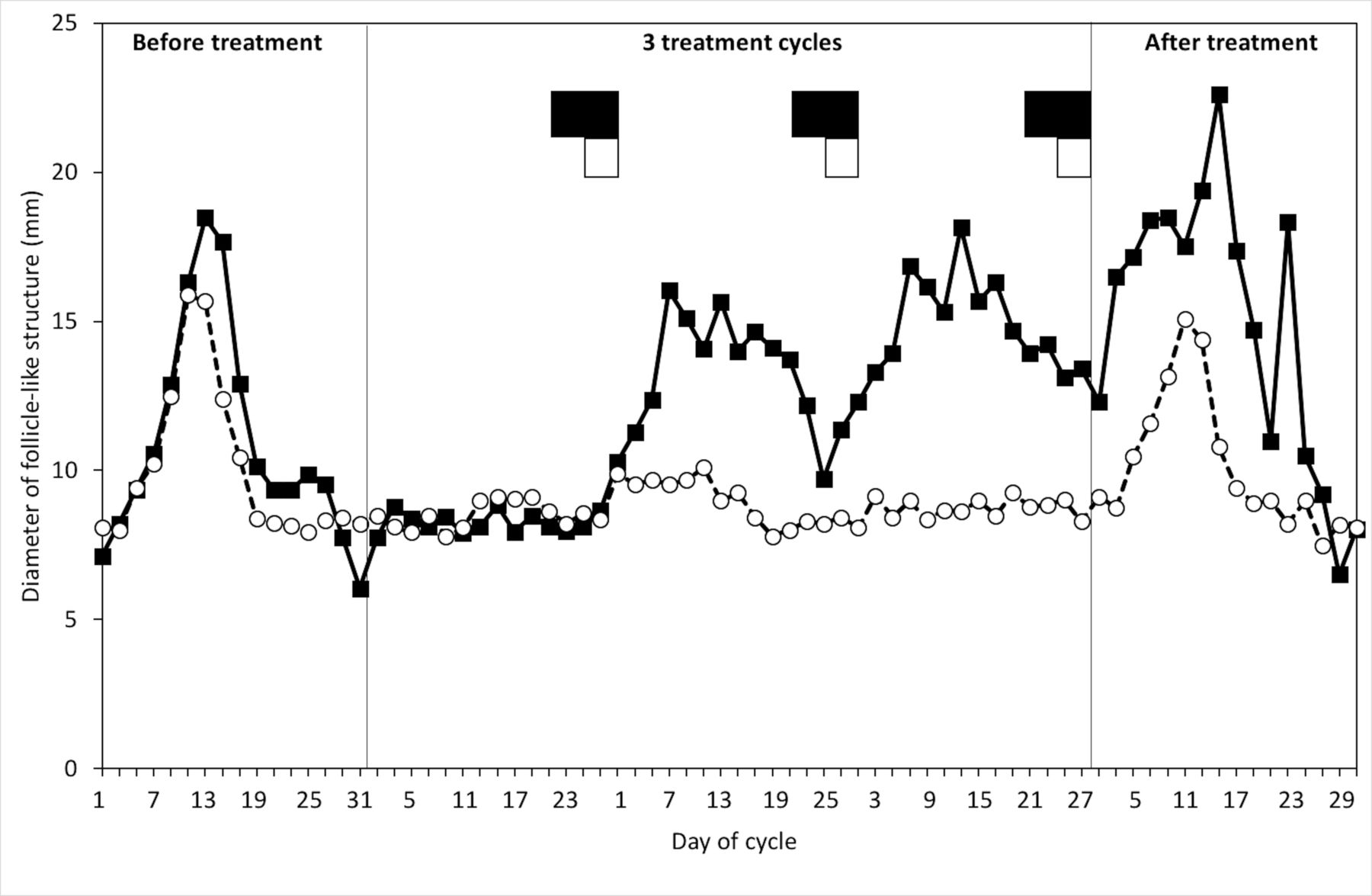
The size of follicles appears to be inversely related to the dose of EE.12 13 However if the CFI is shortened, ovulation must be less likely to occur if tablets are subsequently missed. In an open-label comparative study of a 24/4 versus 21/7 regimen of a 15 EE/60 gestodene (GSD) COC, ovarian activity was monitored with ultrasound scans and blood samples every other day over five cycles.16 The 24/4 regimen inhibited ovarian activity more effectively than the 21/7 regimen (figure 1), with a greater increase in serum estradiol with the 21/7 regimen (figure 2).

Mean diameter of the largest follicle-like structure with 21- and 24-dayregimens. ◼, 7-day pill-free interval; ◻, 4-day placebo-pill interval; –◼–, 21-day; --○--, 24-day. Adapted from Ref,16 with permission from Elsevier.

{kind=link}
{kind=link}
Mean serum estradiol (17β-E2) concentration with 21- and 24-day regimens. ◼, 7-day pill-free interval; ◻, 4-day placebo-pill interval; –◼–, 21-day; --○--, 24-day. Adapted from Ref,16 with permission from Elsevier.
Similarly, in a double-blind RCT of 20 EE/3000 DRSP,17 there were two parallel treatment cycles of either a 24/4 (n=49) or a 21/7 (n=50) regimen. Ovarian activity was monitored by vaginal ultrasound scans and hormone measurements every 3 days for the duration of the study. In the second cycle, one woman in the 21/7 group ovulated following the 7-day CFI and another woman had a luteinized unruptured follicle (LUF). This was followed by a third treatment cycle for both groups, with the initial three active pills replaced by placebos. The ovarian activity scores were significantly greater in both groups. In the 21/7+3 group there were four apparently normal ovulations. Of potentially greater interest, one woman ovulated in the other group taking 24 active tablets followed by a CFI of 4+3 days. The deliberate dosing error, which only lengthened her CFI to the ‘normal’ 7 days, permitted one ovulation, just as among the 21/7 group in the earlier control cycle. Comparing 24/4 and 21/7 cycles, the researchers reported a significant 6-fold greater ovarian suppression by Hoogland scoring, with neither ovulation nor LUF, when the CFI was restricted to 4 days.
A systematic review of the effect of extending the CFI to between 8 and 14 days found wide variability in the amount of follicular development and incidence of ovulation.12 In one study of a 9-day pill-free interval, presumptive ovulation as indicated by serum progesterone levels ≥3 ng/mL occurred in 3/34 women taking 20 EE/100 LNG and in 2/35 women using triphasic 35 EE/180–250 norgestimate (NGT).18 Yet in a study of a 10-day CFI, 12/30 women taking 20 EE/150 DSG and 8/34 women in each of the 30 EE/75 GSD or phasic 30–40 EE/50–100 GSD groups developed follicles greater than 18 mm, but no normal ovulations were reported in either group after resumption of COC-taking.19
Zapata et al 12 also note that when escape ovulation has occurred, the cycles are usually abnormal. However, given individual variation in responses, as described below, risk of pregnancy cannot be excluded. While a shortened 3–4-day CFI provides greater ovarian suppression,16 20 eliminating the CFI completely is even more effective.21 22
Cervical mucus
The suggestion that the cervical mucus effect may provide adjunctive contraceptive protection following 7-day or even longer CFIs12 should be considered with caution. Although a study examining cervical mucus in 28 women throughout 7-, 9- and 11-day CFIs in four cycles reported that cervical mucus remained unfavourable to sperm penetration, the authors remark on the individual variation in response.23 A recent review found the existing evidence base to be very limited for the contribution of progestogen-affected mucus to contraceptive efficacy.24 Furthermore, any such effect of the progestogen component of COCs must be at its lowest if a fertile ovulation is pending, whether due to a true ‘pill-failure’ after a 7-day CFI or after a lengthened CFI, as it will be at least 168 hours since the progestogen was last ingested. Indeed, users of all marketed progestogen-only pills (POPs) are advised to assume loss of the contraceptive effect on their cervical mucus much earlier when a tablet is taken late.
Effects of individual variation
This applies at several levels, including individual responsiveness of the woman taking the hormone and variation in hormone absorption and metabolism,23 25 which are also affected by weight and age.26 In a randomised crossover study, 24 women were given a single dose of each of three bioequivalent 35 EE/1000 NET formulations and 27 women received a single dose of three bioequivalent 50 EE/1000 NET formulations. The large intra-individual variation in blood levels of both EE and NET was found to be of the same order of magnitude as inter-individual variation, suggesting that differences in the effects of any given pill cannot be attributed solely to difference in the doses.27
Few studies have addressed the effect of ethnicity, despite evidence of substantial differences, with the lowest plasma levels of EE consistently observed in Nigerian women and the highest in Thai women, even when corrected for body surface area.28
All these differences become more significant as doses of contraceptive hormones decrease: contraceptive efficacy in the 21/7 regimen with its regular week of lost ovarian suppression is likely to be lower in women with low bioavailability of EE and a short elimination half-life than in women with a high EE bioavailability and a high elimination half-life.29
Adherence
In a cohort study of 3316 women in France, 23% of women using COCs reported missing a pill at least once during a 28-day cycle, of whom 42% missed a pill during the week following the CFI.30 In a follow-up to the same study, pill omissions were fewer with regimens where placebo tablets were taken during the CFI.31 Similarly, an observational study of 402 women recording COC use over 6 months compared the 29% of participants taking placebo tablets during the CFI with 71% using COCs with a tablet-free CFI and found that the latter group were significantly more likely to self-report delayed restarting of active pills (P=0.0002).32
But self-reports of pill omissions underestimate actual omissions. In an RCT of pill-taking tracked by an electronic monitoring device for three cycles in 82 women, the mean number of tracked missed pills was 4.7±3.2 per cycle compared with 1.2±1.5 recorded in patient diaries.33 The authors comment that their findings may overestimate adherence in the general population since participants knew that pill-taking was being tracked.
A common reason for missing pills is unavailability. One prospective study found that combining ‘no new pack’ (10.5%) with ‘late start’ (4.03%) made tablet omissions lengthening the CFI the most common category in the analysis.34 Further, unavailability of pills was significantly associated with consecutive pill omissions, though these were infrequently of more than three tablets.
Effect of regimens on bleeding
A systematic review of 11 RCTs reported either no major difference in bleeding between cyclical and continuous/extended regimens, or fewer bleeding/spotting days with continuous/extended regimens.4 The continuous flexible regimen is associated with significantly fewer total days of bleeding per year than either continuous or cyclical regimens.35–37
There are few data comparing unscheduled bleeding rates with different COC formulations. A double-blind RCT of 136 women randomised to four combinations of EE, LNG and NETA taken continuously found that after 6 months 20 EE/1000 NETA was associated with the best bleeding profile, followed by 30 EE/1000 NETA, 20 EE/100 LNG and 30 EE/100 LNG. With each progestogen the lower 20 EE dose was better than 30 EE for that endpoint, but using the less potent type of progestogen (NETA) was also apparently beneficial.38 There are no comparative data with other progestogens.
Effect of regimens on hormone withdrawal symptoms
Continuous/extended regimens can significantly reduce symptoms resulting from hormonal withdrawal during the CFI, typically menstrual pain, headache, bloating or swelling, and breast tenderness.39 40 Further, they have the potential to reduce the incidence of other medical conditions associated with the changing levels of hormones during the luteal phase of the natural menstrual cycle, including migraine and epilepsy.40
Hormone withdrawal symptoms when taking active pills following the usual 7-day CFI have been attributed to recruited follicles undergoing atresia, resulting in a drop in endogenous estradiol levels.13 16 17 20 22 41 42
Safety implications of continuous/extended regimens
For women on a 20 µg EE pill switching from a 21/7 to a continuous regimen there will be an increase in the total annual dose of EE from 5460 µg to 7300 µg. However, this is still less than the total annual dose of 8190 µg EE from the more usual 21/7 use of a 30 µg EE pill.
COC use, for any duration, results in an inactive endometrium. There is no evidence of greater risk of endometrial hyperplasia or malignancy with continuous use than with a 21/7 regimen.4 41 Limited data also confirm no clinically significant differences between regimens with respect to lipid and carbohydrate profiles, bone markers, or haemostatic variables.43 Such metabolic data are reassuring, but possible circulatory risks (or benefits) of continuous or extended regimens using 20 µg EE pills will need full epidemiological evaluation.
Acceptability of continuous/extended regimens
Even in the absence of typical menstrual disorders, menstrual periods can still have an adverse effect on women’s lives. In a questionnaire study of 270 women of reproductive age, after excluding women with menstrual symptoms such as headache, dysmenorrhea, menorrhagia or premenstrual syndrome, 75.6% reported that their normal menstrual periods interfered with their sex lives, 28.8% preferred not having their period when at work and 48.4% reported that periods interfered with sport.44 Overall, 56.3% of the women stated that they would prefer amenorrhoea or reduced menstrual frequency, among whom almost three-quarters would be prepared to use medication to achieve this.
Of 220 women who selected their own regimen following trials of extended cycles, 60% continued the extended cycle for more than 2 years and 88% of 121 such women chose to use a continuous flexible regimen, Option 1 as described below.45
In a questionnaire survey of 1001 women attending family planning clinics and 290 contraceptive providers in China, South Africa, Nigeria and Scotland, only among black women in Africa did the majority ‘like’ having periods. In all other groups, most women disliked periods, which were ‘inconvenient’ and associated with menstrual problems. In all except the Chinese centres, the majority of women would be willing to try a contraceptive that induced amenorrhea.46
Conclusions
We believe that it is time to follow the evidence and consign the 7-day contraceptive hormone-free interval to history, changing COC packaging and guidance accordingly. Through eliminated or infrequent and short CFIs, the continuous/extended regimens are associated with numerous non-contraceptive as well as contraceptive benefits,47 with no differential safety concerns, although more data will be needed to confirm this.
Failure of 21/7 COCs has always been attributed primarily to failure of patient adherence to pill-taking rather than to the intrinsic weakness of the method. Given the 0.3% failure rate in the first year for ‘perfect’ use,3 it is counter-intuitive that the equivalent failure rate of 9% for ‘typical’ use,3 in which a small number of pills is not taken correctly, should be as great as an order of magnitude higher. The data reviewed here explain that anomaly. The excessive duration of the CFI makes the method unforgiving of user-errors in the (clinically unidentifiable) vulnerable subgroup who develop the most follicular activity during the CFI.12 17 In continuous use the safety margin for errors is much greater, to up to seven tablets at any time.47 Users' increased confidence if some pills are omitted should greatly reduce the demand for emergency contraception.
Although laboratory and some observational studies indicate that whenever a 7-day break is taken, even in extended regimens, there must be an increased conception risk, to date no studies have actually established lower pregnancy rates in oral regimens with shorter or absent CFIs. We maintain that this is because in clinical trials of all COC regimens, including 21/7 regimens, contraceptive efficacy can be expected to be generally well-maintained, as recruitment criteria include women who are likely to adhere to trial instructions. The frequency with which tablets are omitted in the real world, coupled with significant inter- and intra-individual variation in absorption and metabolism of contraceptive steroids, promotes failure of any regimen with a 7-day CFI in a small, but unfortunately not clinically identifiable, subgroup of the general population.
Recommendations for practice
We therefore recommend that, based primarily on efficacy grounds, the first-line regimens offered for COCs should be those in which the CFIs are eliminated or infrequent, and not longer than 4 days, as outlined in the options below. These regimens are data-led and fully supported by the WHO and the UK Faculty of Sexual & Reproductive Healthcare. However, despite ‘running-on’ packets for indications such as postponement of bleeding already being present in the Summaries of Product Characteristics of many COCs, if CFIs are eliminated altogether that regimen must be prescribed on the basis of being an unlicensed use of a licensed product. Such use is clearly permitted by the UK General Medical Council with criteria that must be followed carefully.48 Until ‘official’ printed leaflets are available, such off-licence prescription must include provision of a dedicated patient information leaflet. This is valued by patients and optimises counselling during routine consultations.49 An example is included in the online supplementary text.
Supplemental material
Options for prescription of continuous/extended COC regimens
Option 1. Continuous flexible (or tailored) regimen
The continuous flexible regimen comprises uninterrupted daily pill-taking, with the user option of a 3–4-day pill break to manage excessive unscheduled bleeding, but always preceded by at least 7 days of pills.11 This is associated with significantly fewer annual days of bleeding than other regimens.35–37 A 20 µg EE formulation should be the first-line choice, given the lower annual hormone dose compared with formulations with 30 or 35 µg EE and a favourable bleeding profile.
Option 2. ’Tricycling' with shortened CFIs
These extended-use options of a fixed duration of pill-taking before a shortened CFI have similar potential to minimise user failures. A common version is 84/4 for women who favour quarterly withdrawal bleeds, but since in the UK COCs usually come in packs of three cycles, a satisfactory variant is 63/4. A 20 µg EE product should be first-line, taken as three or four consecutive packets, followed by a 4-day CFI.
Option 3. For women preferring monthly bleeds
Women who prefer a monthly bleed may still benefit from improved contraceptive efficacy and margin for error with the COC of their choice if their CFI is no longer than 4 days. Correct intervals between packets can now easily be achieved by using apps that permit the user to alter the number of days on which she is reminded either to take or not to take tablets. Not all apps incorporate appropriate safeguards to minimise the risks of missing a reminder.50 We recommend ’myPill Birth Control Reminder', an app that is available free on both Android and iOS platforms.
Additional educational resources
References
Footnotes
Contributors Professor MacGregor undertook the literature search and wrote the first draft. Professor Guillebaud revised the draft and both authors approved the final version. Both authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Professor MacGregor reports personal fees from Consilient, Bayer and Elsevier, outside the submitted work. Professor Guillebaud reports personal fees from the Wellcome Trust and from Bayer HealthCare, outside the submitted work.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue