Article Text

Abstract
Objective The Massachusetts Access Program is a statewide, centralised referral and case management program created to address barriers to later second-trimester abortions. This study outlines the scope of, describes provider experiences with, and evaluates provider acceptability of the Program.
Study design We invited physicians, nurses and staff working in hospitals within the later abortion provider referral network to participate in a mixed-methods study that included a web-based quantitative survey and/or a semi-structured qualitative interview. We used descriptive statistics to analyse survey data and inductive coding methods to analyse interview data.
Results From 2007–2012, 15–28% of abortions performed in Massachusetts at 19 weeks or greater gestational age annually were scheduled through the Access Program. We received 16 completed surveys and conducted seven interviews with providers who routinely receive referrals for later abortions through the Program. Providers overall reported positive experiences with the Program and found it highly acceptable. They described that the transportation, accommodation and financial assistance enabled patients access to care. The specialised and updated knowledge of the Access Coordinator in regards to abortion care also allowed her to act as a resource for providers.
Conclusions The Access Program, through its referral and case management network, was a valuable resource both to patients seeking later second-trimester abortions and providers involved in abortion care. It acts as one example of an effective, highly acceptable and potentially replicable intervention to reduce barriers to obtaining later second-trimester abortions.
- abortion
- qualitative research
- reproductive health politics
Statistics from Altmetric.com
Key messages
Women seeking later abortions face many barriers to care. A centralised referral network of abortion providers can improve patient access to abortion care.
A case manager who stays abreast of local and national abortion resources, policies and regulations is a valuable resource to both providers and patients.
Introduction
A long-term trend in declining abortion access has accelerated in the United States over the past few years, as states are passing an unprecedented number of restrictive abortion laws.1 Due to these restrictions, the number of clinical sites and providers offering second-trimester abortions is decreasing, making second-trimester abortions increasingly difficult to access logistically.2–4 Structural barriers known to delay abortion include difficulty finding an appropriate provider, incorrect referrals, transportation issues, and financial costs.5 6 Overall, these challenges disproportionately affect low-income and Medicaid-eligible women, who on average present for abortion services later than their wealthier counterparts.7–9 While abortion at any gestational age is a low-risk procedure10 and safer than childbirth,11 abortion care remains a time-sensitive issue as medical risks12 and costs13 increase the later an abortion is performed. Moreover, second-trimester abortion can be more complicated, often requiring serial cervical dilation, two-visit procedures, brief hospital admissions, and/or heavier sedation. As a result, accessing, undergoing and recovering from care requires greater patient time and social or logistical support.14
Massachusetts is one of 17 US states in which public Medicaid insurance covers abortion care, and private insurance is legally permitted to and often reimburses abortion services, resulting in relatively few financial barriers for most residents.15 However, in 2003, Massachusetts enforced a state-level Medicaid regulation stipulating that all abortions after 19 weeks’ gestation must be performed in a hospital setting to be funded by Medicaid.16 Due to concern that this law would increase barriers for patients, abortion providers and allies created the Massachusetts Access Program (hereafter, ‘the Program’). In 2012, the Program expanded to include women earlier in pregnancy with medical or social needs requiring more complex abortion care. In 2014, Massachusetts eliminated site-of-service limitations on payment of abortion services, allowing Medicaid-insured patients to receive later second-trimester abortion at their choice of provider.17 This study includes Program data from 2007 to 2012 and provider experiences up to 2014.
The Program is a statewide referral and case management program partnered with a network of hospitals whose abortion providers and scheduling staff agreed on joining to provide expedited abortion appointments. These institutions are large-volume hospitals with established gynaecology departments that provide abortion care up to the state gestational limit of 24 weeks’ gestation. They are located throughout Massachusetts, including facilities in the central and western regions of the state, though the majority are in eastern Massachusetts. During the study period, the Program served Massachusetts residents who (1) sought abortion at >19 weeks’ gestational age and (2) were Medicaid insured, uninsured or required hospital-based abortion care for medical reasons. Patients typically learn about the Program when they seek abortion care from a community-based abortion provider unable to care for them due to advanced gestational age or complex medical needs.
Patients are referred to the Access Coordinator (hereafter, ‘the Coordinator’), the primary contact of the Program. The Coordinator role is one full-time position, which was held by two separate individuals over the study period. The Coordinator is not a clinical provider, but rather an unlicensed lay worker experienced in abortion care. In addition to scheduling appointments with appropriate providers, the Coordinator provides individualised pregnancy options counselling and triages pre-procedure medical and social needs. The Coordinator also obtains support from local and national charitable funds for procedure costs for the few patients who lack insurance coverage for the abortion itself. Additionally, the Program directly funds associated non-medical costs such as patient transportation or lodging needed to access care. Figure 1 depicts the typical Access Program referral process.

Steps and components of an Massachusetts Access Program referral.
Prior studies have identified obstacles to obtaining abortions, but literature on interventions to ameliorate these structural barriers has been limited. This study uses Program and state-level public health data in addition to provider surveys and interviews to describe the patient population, provider experiences, and acceptability of a unique statewide, centralised referral and case management program for advanced gestation second-trimester abortions.
Methods
We reviewed internal program data, including patient volume, demographics, and outcomes of referrals, and then compared them to statewide abortion data from the Massachusetts Department of Public Health. We assumed that the population of women seeking abortion services on a calendar year was roughly comparable to those on a fiscal year (ie, January–December 2010 to July 2010–June 2011).
We utilised a mixed-methods approach to assess acceptability of the Program to providers, including a web-based quantitative survey and semi-structured qualitative interviews. Providers were defined as physicians, nurses or clinic staff from an institution within the Program provider network. In 2014, we emailed providers identified by the Coordinator as having had at least three points of contact with the Program in the previous year. In the email, we described the purpose of the study with a survey link and encouraged participants to forward the link to other known Program providers.
The survey included questions with Likert-scale response options. We administered and managed the survey using REDCap, a web-based, secure survey tool.18 The last survey question asked for interview volunteers. One-on-one interviews were semi-structured and audio-recorded. We did not collect personal identifying information or offer compensation to participants. The survey and interviews addressed perceived impact of the Program on quality of patient care and provider workload, as well as overall acceptability of and satisfaction with the Program. They also explored areas for improvement and motivations for continued participation.
Results from the survey are presented as descriptive statistics. Each interview was transcribed, then coded by two investigators independently using Atlas.ti software (Berlin, v.7, 2015). Analysis utilised an inductive coding technique and an interrater consensus method to resolve any discrepancies.19 Common themes and responses were identified and described.
This study was exempted from review by the Office of Human Research Administration at the Harvard T.H. Chan School of Public Health.
Patient and public involvement
This study aimed to describe provider experiences with the Program. Given the retrospective nature of the study and the sensitivity of patient information, patients were not directly contacted or involved, though we attempted to capture some component of patient experience through providers’ descriptions of interactions with patients. Potential study participants, including a physician and a nurse, assisted with and piloted both survey instruments for clarity and thoroughness prior to recruitment.
Results
Program population and scope
Between 357 and 518 women contacted the Program annually during the study period; approximately half were eligible. The vast majority of eligible women were scheduled for an abortion procedure. Reasons women were not scheduled or did not complete a procedure included loss to follow-up or the patient choosing to continue the pregnancy (table 1). Patients scheduled for abortion care through the Program were offered an appointment within 1–5 business days. The largest determinant of time from initial contact to appointment was the day of the week when contact was made; for example, those who called on Friday often waited until the following week. Patients undergoing second-trimester procedures also needed to be able to access care on two consecutive business days.
Outcomes of women who contacted the Massachusetts Access Program during the period 2007–2012*
Demographic characteristics of people who sought assistance from the Program remained relatively similar over time (table 2). Cumulatively, patients were young, with teenagers accounting for 26% (611/2392) of all patients and over 60% of all patients under the age of 24 years (1453/2392). Patients came from many different racial and ethnic backgrounds, with more black and Hispanic patients obtaining abortions through the Program compared with the general population of Massachusetts and women who obtained abortion in Massachusetts overall (table 3). The majority was insured through MassHealth, Massachusetts’ Medicaid program, prior to receiving care. Privately insured patients accounted for 19% of all contacts (444/2348), while 14% were uninsured (325/2348). Although insurance coverage for abortion is legal in Massachusetts, some insured patients likely did not have abortion coverage and would have required funding assistance for the procedure; these numbers were not separately tracked in Program data.
Massachusetts Access Program patient characteristics during the study years 2007–2012*
Massachusetts Access Program patient race/ethnicity characteristics over the study years 2007–2012 compared with the overall population of Massachusetts and patients obtaining abortions in Massachusetts
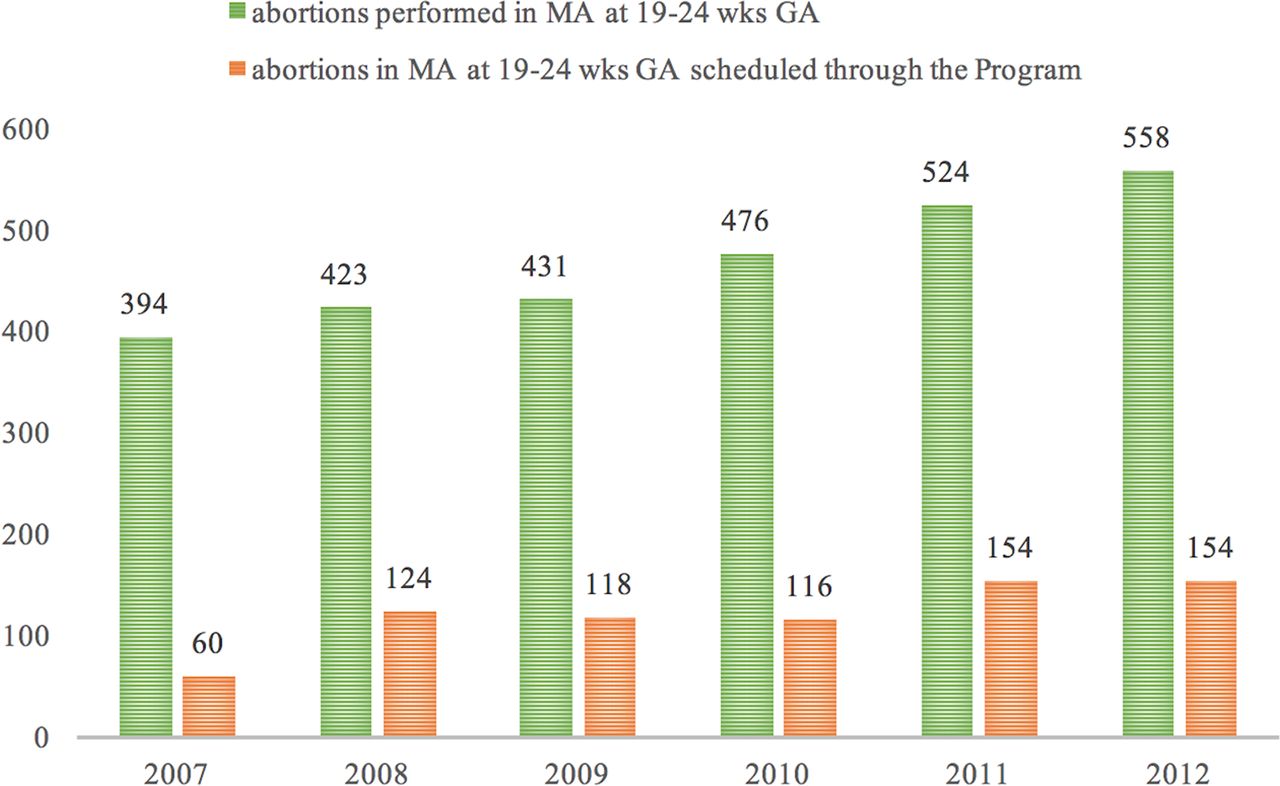
A notable proportion of patients who received later second-trimester abortions in Massachusetts were referred through the Program. From 2007–2012, the Access Coordinator scheduled between 15% (60/394) and 29% (154/524) of all abortions performed at a gestational age >19 weeks in the state (figure 2).
{kind=link}
{kind=link}
Second-trimester abortions >19 weeks obtained through the Massachusetts Access Program in relation to the total number of abortions provided in Massachusetts, calendar year 2007–2012.
Provider experiences
We identified 33 providers for initial recruitment. Twelve physicians, three nurses and an office manager completed 16 surveys. The self-reported number of 19+ week abortions spanned 10–300 per year for the entire practice or facility, with 5–75% of these referred through the Program. We also conducted seven interviews, six with physicians and one with a nurse. This sample represents four of seven institutions within the Program network over the entire study period, including two facilities that together receive about half of the referrals annually. Four additional institutions joined after 2012; two are represented in the interview population.
Program acceptability and perceived impact
The survey assessed overarching attitudes and beliefs about the perceived impact and acceptability of the Program with a five-point Likert scale. Table 4 presents detailed survey results. Providers indicated that they received appropriate and complete referrals that helped them manage patient care. They reported high satisfaction with the referral process and a willingness to continue participation in the Program.
Provider responses to survey questions regarding Massachusetts Access Program experiences and overall acceptability (n=16)
Interview responses were consistent with survey data. Participants described the Coordinator as accessible, professional and dedicated. They consistently reported positive interactions with the Program and stated that their patients also reported positive experiences (table 5a). Some providers felt their Program-referred patients were better informed compared with other second-trimester abortion patients due to comprehensive counselling from the Coordinator about pregnancy options and the abortion process (table 5b). Every provider interviewed indicated that they planned to stay active within the referral network, with many citing their belief that the Program fulfils a key role in addressing barriers to care as a motivating factor (table 5c).
Subthemes and illustrative quotes from interviews with providers within the Massachusetts Access Program network
Key features of the Program
Providers identified Program characteristics that shaped their experiences, including the overall ease of referrals, available counselling, and logistical support. Many detailed the logistical assistance provided by the Coordinator in terms of scheduling, transportation, accommodation, and financial assistance, emphasising that these services addressed barriers that may otherwise prevent their patients from receiving care (table 5d).
Most providers emphasised the Coordinator’s comprehensive expertise relating to abortion care, including medical knowledge and insight into the process of navigating abortion services. The Coordinator had more up-to-date information on funding resources than clinical providers, as well as specific, localised understanding of the policies, schedules and limitations of each hospital within the referral network (table 5e). Providers noted that this specialised information was key to ensuring timely and appropriate care (table 5f).
All providers highlighted the unanticipated reciprocity of referrals between themselves and the Coordinator. Providers described the ability to not only accept referrals but actually refer patients back to the Coordinator for further management. This type of reciprocal referral was not an explicit function of the Program, but emerged as a valued aspect for providers, who used the Program as a resource for patients they could not personally manage due to scheduling issues, the gestational age limit allowed by their institutions, or complex social issues (table 5g).
Areas for improvement
In general, providers stated that awareness about the Program among participating institutions was high. However, some felt that non-participating local healthcare providers were not aware or had incomplete information about the Program and the extent of services offered. One provider described that she often received calls from community providers trying to refer patients or with questions regarding later abortion services, and that these calls were likely better triaged by the Coordinator.
Ease of follow-up was another area for potential improvement. Providers described that typically with referrals, they communicate with a referring physician for patient hand-offs regarding post-procedure care, debrief of complications, or longitudinal clinical concerns. Due to the indirect referral process through a third-party case manager (the Coordinator) and the sensitive nature of later abortion care, providers often lacked the ability to report back to a physician who provides long-term and ongoing care to the patient.
Providers were specifically questioned regarding referrals from the Coordinator that they were unable to accept. This was universally described as a rare occurrence. Reasons for being unable to accommodate a referral included advanced gestational age and insurance issues (eg, provider was out-of-network).
Discussion
In this mixed-methods study, we examined a unique, centralised statewide program providing referral and case management services for women seeking later second-trimester abortions. Women who sought Program services were young and primarily publicly insured. They were racially and ethnically diverse compared with the general population of Massachusetts, as well as the overall population of women obtaining abortions in the state. These findings are overall consistent with previous literature regarding the increased rates of abortion in general and at later gestational ages among women of colour.20 We used state data to demonstrate that during the study period, a significant proportion of women who received abortion at >19 weeks’ gestation in Massachusetts were scheduled through the Program.
Providers within the referral network overwhelmingly reported positive experiences and high satisfaction with the Program. All providers conveyed willingness to continue participation in the Program’s referral network, indicating a high level of acceptability among a core group whose buy-in is necessary for its continuation. Providers emphasised that they believed Program services improved access and health equity among the women of Massachusetts.
All providers highlighted the importance of the Access Coordinator, particularly their thorough knowledge regarding local scheduling particularities and ability to utilise connections, grants and Program funds to address transportation, lodging and financial barriers. Provider descriptions of patient experiences with the Coordinator mirror the functions of a patient navigator. Patient navigators guide patients with a difficult diagnosis, such as cancer, through barriers in a complex health system to facilitate timely screening, follow-up and treatment. Navigators have been shown to improve patient experiences and outcomes, particularly around reducing disparities in access to care.21 Similarly, abortion care is a unique field, a frequently changing landscape with very specific regulations and procedures to navigate along the course of receiving care – particularly in the later second trimester, when the difficulty of locating appropriate care is compounded by the need to do so more urgently. Laws and policies affecting the availability of care are constantly evolving, as are available resources such as abortion funds. Many providers suggested that they cannot stay abreast of this information. Having a case manager who stays up-to-date creates a resource readily accessible to both patients and providers. The ability to quickly tap into resources and plug the patient into appropriate care with an appropriate provider was crucial, particularly when working against gestational limits.
The importance of reciprocity stood out to investigators. Providers viewed the Program not only as a source of referrals, but also as a resource that could be utilised should their own patients experience difficulty accessing care. Providers emphasised the quick, streamlined process of handing off a referral to the Coordinator and described relief knowing the patient would be guided towards care. While not an original goal of the Program, it has evolved to become a two-way referral line, reinforcing the idea that the Access Program was a resource to not just women seeking abortions, but to providers themselves.
Some providers proposed enhanced post-procedure follow-up with the patient’s regular care team as an improvement to the Program’s current structure. This suggestion echoes the literature regarding best practices in referral systems, with the abortion provider taking on the role as a consultant or specialist.22 23 For many patients, closing the loop with a primary provider may not be feasible due to confidentiality concerns or stigma. However, improving referral communication when appropriate and desired by the patient allows for abortion care to be integrated into patients' overall reproductive healthcare.
A limitation of our study is selection bias, as providers with positive experiences may be more likely to respond and participate in our survey or interviews. Though the overall sample size is small, we felt there was broad representation of institutions in our respondent population, including the institutions that regularly receive a significant proportion of the referrals. It is difficult to predict how well the Program may translate into regions with fewer abortion resources than Massachusetts, as Massachusetts houses most later second-trimester abortion providers in New England. In 2013, the Program expanded its eligibility criteria to include patients residing outside of Massachusetts, including primarily northern New England (Vermont, New Hampshire and Maine) where later abortion access is overall limited, but also occasional clients from New York, Maryland and Washington DC, where access is mostly adequate.4 This programmatic expansion presents an opportunity to assess whether an intervention similar to the Program could maintain its effectiveness while serving a larger population and some areas with fewer providers. Massachusetts also allows for insurance coverage of abortions, so that while the Coordinator provided multiple services to clients each year, relatively few of these patients required fundraising for the abortion procedure itself. In other states where both Medicaid and private funding for abortion is prohibited, intensive fundraising may be required for clients if this model were replicated. Indeed, nationally only 47% of women used any insurance for their abortion care in 2014;24 staffing needs could therefore be greater in other states.
Addressing barriers to abortion access is increasingly important in the setting of rapid passage of new laws restricting abortion care. A multi-pronged approach is needed in the face of this public health crisis, including advocacy, policy change, support of current abortion services, and expansion where possible. With increasing challenges in access, patients seeking abortion care must be supported and connected to available resources and providers. Overall, the Access Program is an example of a highly acceptable, potentially replicable intervention that has shown some success in improving abortion access in Massachusetts after a Medicaid regulation imposed significant logistical obstacles to care disproportionately affecting lower-income women needing later abortions. Our study describes core program services as well as a patient navigator role identified by providers as key in sorting through the evolving abortion landscape. These findings can shape future interventions aimed at ameliorating barriers to abortion services and increasing abortion care access.
Acknowledgments
The authors thank the program staff at the Access Program for their assistance with obtaining program data and with identifying providers eligible for study participation. They also thank Souci Rollins and Alisa Goldberg for their assistance with study design and content.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was exempted from review by the Office of Human Research Administration at the Harvard T.H. Chan School of Public Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at Portions of the findings were described in posters presented at the National Abortion Federation Annual Meeting in Baltimore, Maryland, USA, April 2015 and the American Congress of Obstetricians and Gynecologists’ Annual Meeting in San Francisco, California, USA, May 2015.
Linked Articles
- Highlights from this issue