Article Text

Statistics from Altmetric.com
Mood changes during use of contraception are often reported as side effects and reasons for dissatisfaction and discontinuation of use. Recent register-based studies show associations between contraceptive use and risk of depression and attempted suicide, especially in adolescents and during the first months of use.1 2 We prospectively assessed the relationships between use of contraception, satisfaction with the method, sleep-related symptoms and psychological well-being.
Within the services offered by the City of Helsinki, all women planning or using subdermal contraceptive implants, all nulliparous women planning intrauterine contraception, or women with contraceptive problems are referred to a Centralized Family Planning Clinic. Our study included 182 women of at least 18 years of age attending this clinic. More than a third of them (37.4%) were planning either to change or to discontinue their contraceptive method. Of the remainder, 52 (28.6%) were starting contraception, and 62 (34%) were attending a follow-up visit and continuing with their present method. We divided the participants into three groups: starters, continuers and switchers/stoppers. All participants received a questionnaire at baseline and after 3 months. Questions covered sociodemographic factors, gynaecological history including contraception, possible substance abuse, and current or past history and treatment of psychiatric disorders. Also, the possible presence, timing and severity of sleep problems, depressive symptoms and suicidal ideation were asked with questions used previously in two large Finnish population-based studies.3 4
The mean age of the participants was 27.3 (±SD 8.7) years, starters being slightly younger (24.8±6.9 years), not significant (n.s.) and more likely to smoke (p<0.01). No statistical significance was found between the three groups regarding other baseline characteristics (ie, previous pregnancies, marital, employment or educational status, drug abuse, psychiatric symptoms). The questionnaire response rate at the 3-month follow-up was 70.1% (starters 75%, continuers 64.5%, switchers/stoppers 73.5%).
Satisfaction with the present method was high (95.1%) among women continuing with it; among women changing or stopping their method, only 18.3% were satisfied. Bleeding problems, pain and mood symptoms were the most commonly reported reasons for dissatisfaction. Bleeding irregularity, but not amenorrhea, was the only predictor for dissatisfaction irrespective of the contraceptive method (p<0.05).
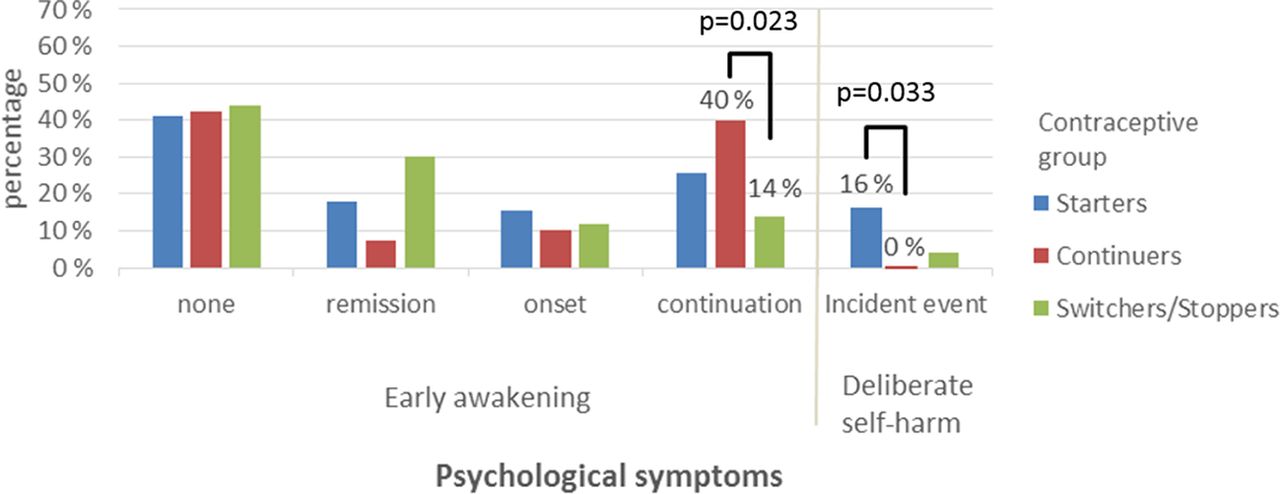
Compared with the group of switchers/stoppers, at follow-up persistency of early awakening was more likely in the group of continuers (OR 2.85, 95% CI 1.17 to 6.90), and insomnia symptoms among the starters (OR 2.55, 95% CI 1.07 to 6.07). Continuers showed a trend to tiredness (OR 2.17, 95% CI 0.91 to 5.15, p=0.052) at the time of follow-up. The difference became significant after controlling for the type of contraceptive method (hormonal vs. non-hormonal, p=0.05; or long-acting reversible contraceptive (LARC) vs. non-LARC, p=0.045). Six of the women starting contraception (16.2%), but none of the continuers, harmed themselves during the follow-up period (p=0.033) (figure 1). All of them reported psychological symptoms at baseline (tiredness, nervousness n=6; sleepiness n=5; early awakening, depressiveness n=4). Only two of them had a previous psychiatric diagnosis. Among all participants, reporting a symptom at baseline significantly predicted reporting the same symptom at follow-up (p<0.05 to p<0.001).

{kind=link}
Changes in psychological symptoms from baseline to follow-up.
The limitations of our study were the small number of participants, the variety of contraceptive methods used, short follow-up time, the lack of a structured psychiatric instrument, and the non-representativeness of the general contraception-using population. However, only minor associations between psychological symptoms and contraception were found. Women with pre-existing psychological distress were vulnerable to report psychological symptoms. Detecting and counselling women with psychological symptoms is important. Inconsistency with the use of contraception is increased in these women.5 Reducing the risk of unplanned pregnancies in this group of women through effective contraception is one problem less in their lives. Bleeding irregularities, but not psychological symptoms, predicted dissatisfaction with contraception. Thus, counselling about unpredictable bleeding patterns, especially when starting progestogen-only methods, is important. Moreover, ease of access to family planning services if there are questions or worries should be guaranteed.
Acknowledgments
The authors wish to thank all the women who participated in this study and nurses at the Family Planning Clinic.
Footnotes
Contributors All authors contributed to the study conception and design. SS contributed to data acquisition, ET performed statistical analyses, and SS and ET were major contributors in writing the manuscript. All authors contributed to interpreting the results, and reviewing and editing the manuscript. All authors read and approved the final manuscript.
Funding Funding for this study was provided in part by the National Graduate School for Clinical Investigation, the Finnish Cultural Foundation, the Jalmari and Rauha Ahokas Foundation and Helsinki University Hospital EVO grants (ET).
Competing interests OH serves occasionally on advisory boards for Bayer Healthcare, Gedeon Richter and MSD Finland (part of Merck & Co. Inc.) and has designed educational events with these companies. SS has been a consultant for Gedeon Richter and Exeltis and lectured at educational events of Bayer Healthcare and Sandoz Finland (part of Novartis Dimension).
Patient consent Not required.
Ethics approval The study was approved by the ethics committee of the City of Helsinki Health Centre.
Provenance and peer review Not commissioned; externally peer reviewed.