Article Text

Abstract
Background Many women find it difficult to choose and initiate a contraceptive method at the time of an abortion. There is a gap between regular clinical practice and existing evidence on motivational and person-centred counselling, as well as on use of long-acting reversible contraception (LARC). This study aims to describe and evaluate a Quality Improvement Collaborative (QIC) designed to enhance contraceptive services, with regard to changes in healthcare professionals’ (HCPs’) counselling in clinical practice, and in women’s subsequent choice of, and access to, contraception.
Methods Three multiprofessional teams working in abortion services from three hospitals in Sweden, and two women contributing with user experience, participated in a QIC during the period March–November 2017. Using a case study design, we collected and analysed both quantitative and qualitative data.
Results Teams agreed on QIC goals, including that ≥50% of women would start LARC within 30 days post-abortion, and tested multiple evidence-based changes, aided by the two women’s feedback. During the QIC, participating HCPs reported that they gained new knowledge and developed skills in contraceptive counselling at the time of an abortion. The teams welcomed the development of a performance feedback system regarding women’s post-abortion contraception. While the majority of women counselled during the QIC chose LARC, only 20%–40% received it within 30 days post-abortion.
Conclusion The QIC, incorporating user feedback, helped HCPs to develop capability in providing contraceptive services at the time of an abortion. Timely access to LARC remains a challenge in the present setting.
- accessibility
- long- acting reversible contraception
- pregnancy termination
- person-centred counselling
- user involvement
- quality improvement collaboratives
Statistics from Altmetric.com
- accessibility
- long- acting reversible contraception
- pregnancy termination
- person-centred counselling
- user involvement
- quality improvement collaboratives
Key messages
Clinical practice application of evidence on the effectiveness and feasibility of early access to long-acting reversible contraception post-abortion remains a challenge.
A Quality Improvement Collaborative (QIC) – drawing on person-centred counselling and user involvement – can promote changes and support healthcare professionals in providing contraceptive counselling.
Introduction
Many women struggle to find a contraceptive method that suits them,1 2 especially in the context of an abortion.3 This is reflected in a high proportion of repeat abortions, in Sweden as well as in other countries.4–6 Possible causes for repeat abortions include contraceptive failure,7 scepticism about contraceptive methods8 or inadequate trust in healthcare professionals (HCPs) in contraceptive decision-making, in the context of abortion counselling.3 9
Both women and HCPs find it feasible to include contraceptive counselling at the time of abortion counselling;10 for women it is important that the approach is respectful.8 At the same time, HCPs struggle to meet women’s needs in what is often a challenging consultation where emotional concerns regarding the abortion are common,10 11 as is scepticism about contraceptive methods.8 There is still insufficient understanding of how to design contraceptive counselling and services in clinical practice at the time of an abortion to prevent repeat unintended pregnancies (UPs).12 13
It is increasingly recognised that person-centred counselling and motivational interviewing (MI) can help clinicians counsel women regarding contraception.14 15 Likewise, the effectiveness of long-acting reversible contraception (LARC), defined as either subdermal implants, copper intrauterine devices (Cu-IUDs) or levonorgestrel intrauterine systems (LNG-IUSs), in preventing repeat abortions and the importance of easy access to LARC, for example, through 'fast track' services, is growing clearer.16–18 Overzealous LARC promotion may, however, limit women’s reproductive autonomy.19 20 Women have reported feeling pressured to choose LARC and may distrust HCPs’ advice when making such decisions, thus contradicting the intentions of person-centred care and MI.15 19 20
While there is evidence of how to prevent repeat UPs and abortions – including greater use of LARC,16 18 person-centred counselling and MI – such evidence is not consistently applied in practice.13 To improve services – including contraceptive counselling, and clinical practice more broadly, around the time of an abortion – one option is to use a quality improvement approach such as the Breakthrough Collaborative model21–23 and user involvement.24 25 While used extensively in health services,23 such Quality Improvement Collaboratives (QICs) and user involvement in abortion care are hard to find in the literature. In a QIC, several teams come together around a body of knowledge and seek to close the gap between existing evidence and regular clinical practice and, thereby, to improve health and healthcare.22
In Sweden, midwives and gynaecologists (subsequently jointly called healthcare professionals, HCPs) share in providing contraceptive services, including counselling, prescription of contraceptives and insertion of LARC.26 Specially trained midwives also provide services for early medical abortion independently, including counselling, examination, ultrasound evaluation and treatment.27 Several hormonal contraceptives, such as LNG-IUSs and subdermal implants, are subsidised for women up to the age of 25 years.28 If women choose to use LARC, insertion is usually offered 3–4 weeks after a medical abortion or often immediately after a surgical abortion.27 Despite these conditions, Sweden has one of the highest recorded rates (45%) of repeat abortions, that is, more than one pregnancy termination per woman, in Europe.4 In the otherwise rich data environment,29 there is no national data collection or system to evaluate or record contraceptive counselling post-abortion.11 30
As part of a broader research programme that has documented gaps between existing evidence and daily practice,8 11 18 we hypothesised that a QIC could help clinical teams improve contraceptive counselling and services at the time of an abortion in order to prevent repeat UPs and abortions. In this article, we describe and evaluate such a QIC designed to enhance contraceptive services, with regard to changes in HCPs’ counselling in clinical practice, and in women’s subsequent choice of, and access to contraception.
Methods
Setting
This study involved three departments of obstetrics and gynaecology in south-eastern Sweden; two in mid-sized county-level hospitals (Teams A and B) and one in a smaller district hospital (Team C). The mid-sized hospitals had gynaecologists and specially trained midwives who independently provided early medical abortion, whereas at the smaller hospital, gynaecologists only performed these tasks. The hospitals were situated in communities with historically different rates of repeat abortions.31 In 2016, 636 induced abortions were performed at Hospital A and 459 at Hospital B, whereas 215 induced abortions were performed at Hospital C. In the three hospitals, medical abortions before gestational week 12 represented 85%–100% of all abortions according to local statistics 2016. Nationally, medical abortions represented 93% of all abortions, thus only 7% were surgical.4
QIC design
The three departments were invited to join the QIC following their involvement in previous studies8 11 18 and all agreed to participate. The QIC started in March 2017 and ended in November 2017. Author HK guided participating departments to form multidisciplinary teams, preferably including four or five professionals involved in the abortion services, and including a midwife, a gynaecologist, an administrator, and a social worker, with one of them serving as the team’s QIC coordinator. The coordinator was asked to link the team with an external Improvement Advisor and with researcher HK during the QIC. The researchers (HK, JT, JB and SA) and the Improvement Advisor developed, supported and ran the QIC. One team member (AF) joined the researchers as a coauthor providing a participant perspective.
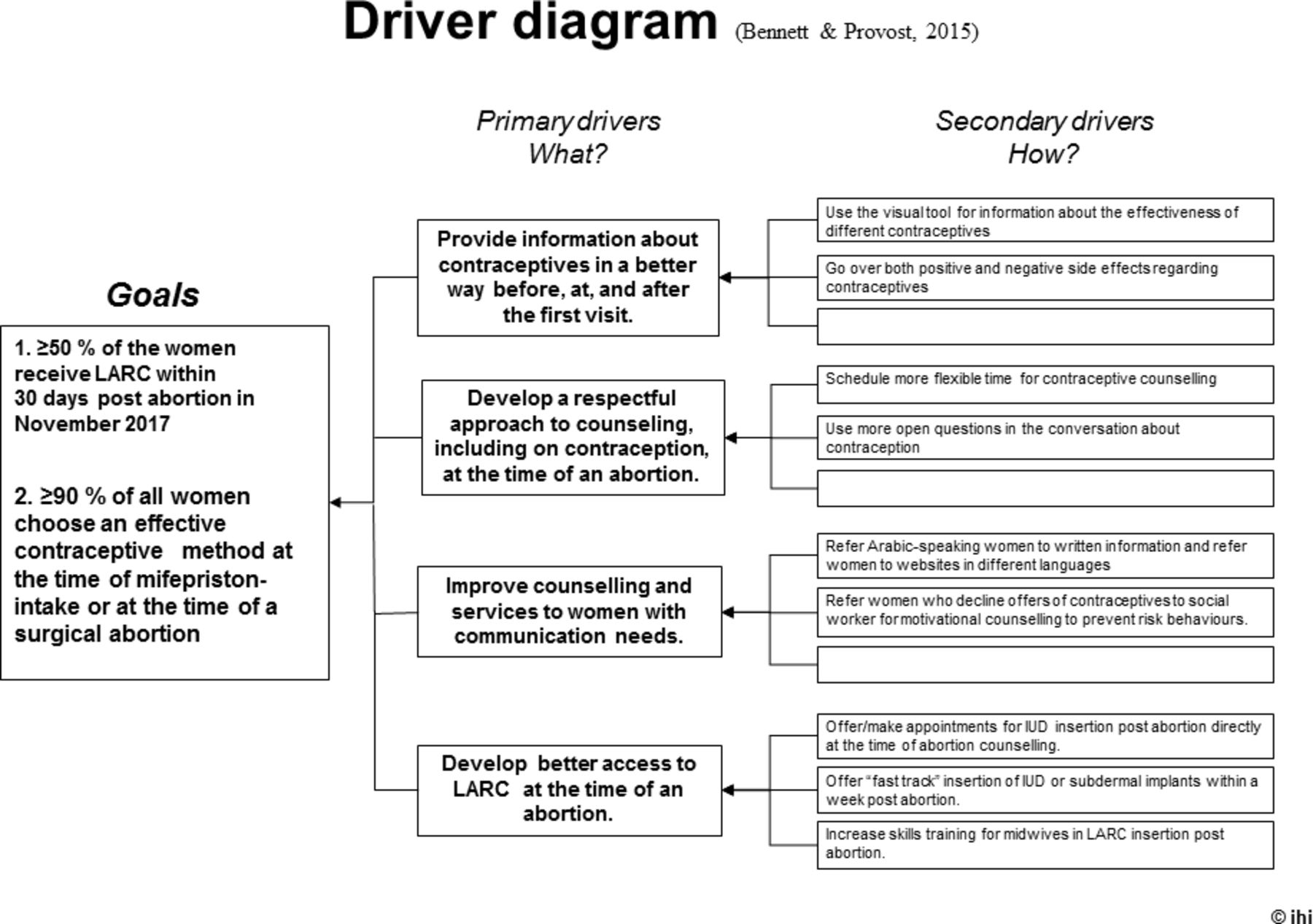
The QIC (figure 1) was based on the Breakthrough Collaborative model22 and involved improvement methods such as the PDSA (Plan, Do, Study, Act) cycle,32 with four learning sessions (LS) where teams met to exchange experiences and learn from the researchers. Using the structure and logic of a 'Driver' diagram,33 the teams were introduced to four primary drivers, or areas of change, based on research evidence from previous studies in the project8 11 18 and in the literature (figure 2). Changes according to these four drivers were expected to enable a greater proportion of women to choose effective contraceptives including LARC post-abortion, and thereby to better prevent repeat UPs.
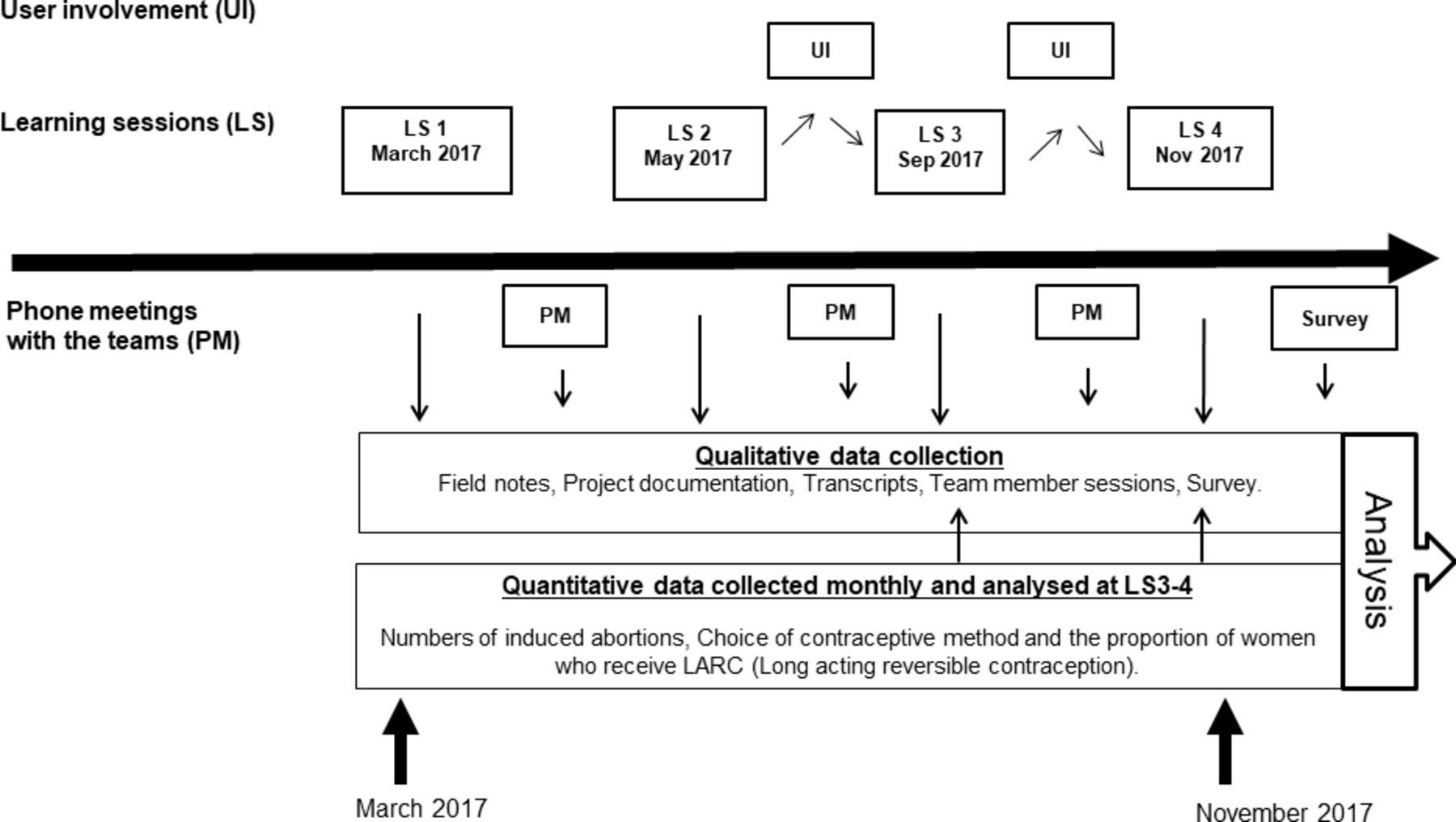
Timeline for the Quality Improvement Collaborative (QIC) and the case study data collection. LARC, long-acting reversible contraception; LS, learning session; PM, phone meeting; UI, user involvement.

The Quality Improvement Collaborative (QIC) Driver diagram, outlining the four main areas for evidence-based changes, for participating teams to introduce locally (Bennett and Provost, 2015).33 IUD, intrauterine device; LARC, long-acting reversible contraception. 'Effective contraceptive method' was defined as LARC or other hormonal contraceptive methods such as pills, rings and patch, and injection.
Patient and public involvement
To include user perspectives, two women with recent lived experience of the issue, and who had participated in a previous interview study within the project,8 agreed to support the QIC. To help the teams improve, they shared their views on the teams’ planned actions via author HK who reported those views in a de-identified way to the teams.25
Study design and data collection
Using a case study design, we combined quantitative and qualitative data collection and analysis to describe and evaluate the QIC and its impact (figure 1).34 35
Collection of qualitative data
Qualitative data included field notes, project documentation and verbatim transcripts from an audio-recorded team member group session during learning session 4 (LS4). Furthermore, data were collected through an anonymous electronic survey of participants to evaluate the QIC 2 weeks after LS4 (figure 1).
Analysis of qualitative data
We analysed qualitative data by content analysis.36 HK read through all qualitative data and highlighted data describing and evaluating the QIC, as well as data indicating changes in HCPs’ counselling and clinical practice at the time of an abortion.
Data regarding the QIC and changes in HCPs’ counselling and clinical practice were coded and sorted in a coding scheme, with categories and subcategories corresponding to the four primary drivers in the Driver diagram (figure 2). Data which did not fit in any of the four driver categories, but characterised the efforts to improve counselling and clinical practice in the QIC, and the effects of these efforts, were sorted and analysed in a separate fifth category. Two additional researchers (JT and SA) took part in the analysis by reading the field notes and the transcript separately. They discussed and reached consensus on the findings. The QIC team participant (AF) reviewed the summary of the findings in the manuscript, adding a form of participant validation.
Collection of quantitative data
Quantitative data included the monthly number of induced abortions, women’s choice of contraceptive method at the time of an abortion as recorded in the medical record, and the number of women who received LARC within 30 days post-abortion.
The ‘time of an abortion’ was defined as the day of mifepristone intake or the day of surgical abortion. Women who underwent abortion related to fetal malformations were excluded from the analyses. The administrator in each team collected de-identified data regarding numbers of abortions and women’s choice of contraceptive method at the time of an abortion manually from medical records each month. If no contraception was chosen, it was recorded as 'No chosen method'.
Data managers from both county health systems retrieved, de-identified and reported digital data regarding the number of abortions and the number of LARC insertions within 30 days post-abortion within the area of each hospital. One team had already measured insertion of LARC manually for several years before the QIC started.
Analysis of quantitative data
We used Statistical Process Control charts to display and analyse data over time and to identify statistically significant signs of change, known as special causes of variation.37–40 In this study, we analysed (i) the proportion of women who had undergone an abortion and chose an effective contraceptive method (defined as hormonal contraceptive methods or LARC methods) and (ii) the proportion of women who started to use LARC within 30 days post-abortion, in both cases per calendar month.
Ethical considerations
All HCPs, and the two participating women who provided feedback based on their experience, gave their informed consent to participate in the study. This study was approved by the Regional Ethical Review Board in Linköping (#2016/486–31; date of approval 22 February 2017).
Results
All three teams (A–C) participated in all four LSs. In each LS, 9–13 team members, 3–4 researchers and the Improvement Advisor participated. Team C participated via video in LS2.
Improvement activities and actions during the QIC
The teams worked on improving their services in the four LSs and the action periods in between the LSs. In LS1, the teams jointly agreed on measurable goals for the QIC regarding women’s choice and start of contraceptive use. The goals were based on what participants considered achievable, on women’s choice of LARC in a previous study in the project,18 and on local measurements in hospital/Team C (figure 2). In subsequent LSs, they helped analyse performance data reflecting their progress (table 1).
Programme for learning sessions during Quality Improvement Collaborative (QIC) 2017
The teams were introduced to two decision aids, aimed to facilitate the contraceptive counselling at the time of an abortion regarding the effectiveness and side effects of different contraceptive methods. The two user representatives in the QIC reviewed these aids and found them helpful in guiding contraceptive decision-making.
At LS2 and LS3, team members interacted in two LSs regarding how to develop a respectful conversation regarding contraceptives and how to handle challenging consultations (table 1). All of these improvement activities were informed by findings from previous studies in the project8 11 18 and by principles of person-centred and MI-based counselling.15 41 The researchers, and a participating social worker trained in MI, designed and led the sessions according to needs expressed by QIC participants.
All teams planned improvement actions in their own departments according to the primary drivers (figure 2). All teams subsequently reported testing and maintaining changes in local clinical practice during the QIC, although to varying degrees (table 2).
Changes and spin-off improvements in contraceptive counselling and services during the Quality Improvement Collaborative (QIC)
Developing contraceptive counselling
Participating HCPs reported having made changes during the QIC in counselling women about contraceptives at the time of abortion. They had started to focus more than before on contraceptive counselling and had started to use the two tools regarding effectiveness and side effects (table 2). They also reported that they tried to be more attentive to women’s needs and to include the women more than before in the contraceptive decision-making.
“I have changed my approach. I try to find a way in the meeting where I can connect with the woman. I feel strengthened in how to develop conversations now.” [A midwife in the QIC]
Developing access to LARC
All teams reported changes in services regarding access to LARC, identified early in the QIC as a barrier for women who want to initiate LARC. Two teams started to offer scheduled appointments for IUD insertion for women who chose IUD, inspired by the two women’s views and the third team in the QIC. Furthermore, they arranged practical training on IUD insertion to improve access to LARC, since only a few midwives in the departments had those skills (table 2).
“Our team has increased the number of appointments for insertion of LARC at the time of an abortion, but we need to provide earlier insertions for women who want LARC. ” [A Gynaecologist in the QIC]
The teams described that their departments had increased the number of available appointments for IUD insertion according to analyses of performance data on women’s choice of LARC at the time of an abortion. All teams identified obstacles in developing access to LARC within 10 days. Teams A and B described difficulties in offering appointments for LARC initiation within 10 days, after two midwives with these skills ended their employment. Team C had difficulties in providing IUD insertion within 10 days after medical abortion, since some gynaecologists declined insertion when ultrasound indicated retained products of conception in the uterus. The gynaecologists were concerned that complications would increase with early insertion.
Teams A and B reported receiving limited support for the work from their department heads and described difficulties in giving their colleagues information regarding the QIC and the proposed changes in practice. Team C, in contrast, received strong support from the department head. Having already started to improve access to LARC before the QIC, Team C discussed the QIC with colleagues at staff meetings every month.
Progress towards QIC goals
Nearly 90% of women (n=594 abortions performed at the three hospitals during the 6 months of the QIC) chose effective contraception (hormonal contraception or LARC) at the time of their abortion.
None of the teams reached Goal 1 (≥50% of women initiating LARC within 30 days post-abortion) by the end of the QIC (figure 3). The control charts revealed no indications of change in the participating departments’ process performance during the QIC compared with the pre-QIC baseline. In Team C, 40% of the women started using LARC within 30 days post-abortion. This team offered ‘fast-track’ IUD insertion and subdermal implant within 10 days post-abortion. Teams A and B discovered, during the QIC, that they faced obstacles to offer fast-track LARC insertion, even within 30 days post-abortion.

{kind=link}
{kind=link}
{kind=link}
P-charts for Teams A, B and C showing the monthly proportion of women who initiated LARC within 30 days post-abortion and its variability. Note that for Team B, the data recording was of uncertain reliability before the QIC. None of the control charts exhibit signals of special cause variation (eg, statistically significant improvement (or change) in performance). 'Initiating LARC' was defined as insertion of LARC noted in the medical record. Data for Teams A and B were drawn from existing electronic health information systems. For Team C, data drew on manual collection started prior to the QIC. LARC, long-acting reversible contraception; LCLp, lower control limit (for proportions); LS, learning session; p-bar, the average of all observations; UCLp, upper control limit (for proportions).
All teams identified gaps between women’s choice of LARC at the time of abortion and women’s actual start of LARC. Across the three participating departments, 60% of the women (n=594) chose LARC at the time of their abortion.
Performance data and information systems
Digital data regarding women’s choice of contraceptive and start of LARC were not available until LS3, due to difficulties experienced by data managers in retrieving the data from source information systems – an effort that had not been part of routine performance management before. Teams A and B expressed difficulties in improving access to LARC initially, as they had no performance feedback system regarding the start of LARC post-abortion. In contrast, Team C benefitted from the manual data collection and feedback system created locally prior to the QIC.
All the teams updated the classification in the electronic health record information system regarding the start of LARC at the time of abortion, since they believed that some procedures had previously been misclassified. Furthermore, Team B realised that they had not been classifying induced abortion accurately (figure 3). They received help from the other teams to develop their system for classification.
Participants’ experience of the QIC
At the concluding LS, team members reported that the QIC encouraged them to keep on improving contraceptive counselling and services at the time of an abortion in order to prevent repeat UPs. They valued interacting with other and different professionals and sharing experience.
"I learnt new things about my department and how we could improve services when we compared with the other teams. I realised that we meet the same kind of women but we have different capacities to meet their needs." [A team member]
Participating HCPs reported improved competence in counselling and described how they had gained more knowledge about contraceptives. Some midwives stated due to their participation in the QIC that they had resumed inserting IUDs. Furthermore, all teams described spin-off changes during the QIC in other parts of their services. HCPs described how they identified unmet needs for contraceptives in other consultations, not related to abortion (table 2).
Discussion
Our findings show how a QIC – drawing on current research evidence, on person-centred counselling and on user involvement – can promote changes and strengthen HCPs in providing contraceptive counselling in challenging consultations in the context of an abortion. They also demonstrate that evidence-based knowledge and user involvement do not automatically translate into performance improvement; participating teams found it challenging to provide LARC in a timely fashion even in the context of a QIC.
None of the teams reached the goal that ≥50% of women chose and received LARC within 30 days post-abortion, even though 60% of the women chose LARC at the time of abortion. This could be explained in part by scepticism among clinicians about early LARC initiation, despite evidence that subdermal implants can be inserted at the time of mifepristone intake42 43 and IUDs within 10 days post-abortion.17 Clearly, important research evidence on prevention of repeat UPs – for example, through early access to LARC – is not always readily applied in clinical practice. Another reason that the LARC insertion goal proved elusive was the delay until LS3 for two teams in getting performance data feedback on the start of LARC. Such a feedback system is of great importance for practitioners and managers to evaluate performance and efforts to improve healthcare generally, including contraceptive services in abortion care.11 38 44 While such data were available in local electronic information systems, it required significant efforts to make these data available in a timely and useful way in this QIC, signalling a paradox in contemporary data-rich health systems.
Members of all QIC teams also described barriers in providing access to IUD initiation.11 Team C reported fewer obstacles in offering appointments for LARC initiation within a week post-abortion, in part due to pre-QIC efforts, spurred on by enthusiastic support from their head of the department. Despite this, even in Team C’s department, only 40% of women had LARC initiated within 30 days post-abortion, during the QIC. Having initially believed that the goal was within easy reach, team members learnt through the QIC that this kind of change might be more challenging than they presumed.
Gaps in women’s choice and actual initiation of LARC may also be due to other factors affecting women’s motivation for contraceptive use, such as fear of negative side effects or pain from insertion of LARC.45–47 Furthermore, women may not fully appreciate the likelihood for a repeat UP,48 which may help explain why some women chose to use no contraceptives at the time of an abortion, even in this QIC.
Methodological considerations
A major strength of this study is that it reports the experience of real-world clinical teams trying to apply the best knowledge on contraception to prevent repeat UPs at the time of an abortion in regular clinical practice, beyond strictly controlled clinical trials. Key limitations include that we were not able to evaluate women’s actual use of other contraceptives apart from LARC or to explore women’s experience of counselling during the QIC. We had to rely on team members’ self-reports of changes in their counselling. Furthermore, the long-term sustainability of changes in practice due to the QIC, their spread to clinicians outside the QIC teams, or their impact on the incidence of repeat abortions could not be assessed, for feasibility reasons.
To strengthen the validity of the findings, we used data triangulation. We collected both quantitative and qualitative data.34 35 The teams in the QIC participated in the interpretation of quantitative performance data during LS3 and LS4, as a form of interactive validation.49 Furthermore, one team HCP validated the study results through co-authoring this manuscript.49 To strengthen the reliability, we described how the case was conducted and presented quotes to show the connexion between the material and the results.34 35
Implications for practice and/or policy
We found that evidence on the effectiveness and feasibility of early access to LARC post-abortion was not fully applied in clinical practice. Teams struggled to change accordingly and this deficit needs further attention to improve abortion services. Our findings also indicate the importance of having a performance feedback system to monitor women’s contraceptive choices and start of LARC in order to improve access to LARC and prevent repeat UPs.
Conclusions
A QIC with user involvement can promote changes in clinical practice and strengthen HCPs’ confidence in providing evidence-based contraceptive counselling at the time of an abortion. Despite the QIC teams’ efforts in the present setting, however, many women who chose to use LARC post-abortion could not receive it in a timely fashion. In many ways, the present study can be considered a feasibility study, where participating teams tested promising ideas to improve performance. How to disseminate effective practice more broadly remains an important topic, beyond the scope of the present article.
References
Footnotes
Contributors HK, JT, SA and JB participated in designing, planning and conducting the study. HK, JT and SA participated in data acquisition. HK, JT, SA, JB and AF participated in data analysis and interpretation. All authors participated in writing the manuscript.
Funding This study was funded by grants from Futurum, the Academy for Healthcare, in the Jönköping County Council, and the Medical Research Council of Southeast Sweden (FORSS).
Competing interests One of the coauthors (JB) has been reimbursed by Merck Sharpe & Dohme, Bayer AB Sweden and Actavis for running educational programmes and giving lectures. All the other coauthors have stated that they have no conflicts of interest in connection with this article.
Patient consent for publication Not required.
Ethics approval This study was approved by the Regional Ethical Review Board in Linköping.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No data are available.