Article Text

Abstract
Background Barriers to accessing abortion care continue to exist even in settings where abortion is legal. We aimed to determine current barriers faced by women seeking abortion, factors that facilitate access to care, and what future improvements women would like made to abortion care in Scotland.
Methods A self-administered anonymous questionnaire of women requesting abortion care at a community abortion service in Edinburgh. Women selected the top three options from predefined lists of barriers to seeking abortion, facilitators of care, and future service improvements.
Results 154/165 (93%) questionnaires were completed by women presenting for abortion. The most commonly ranked number one barrier to seeking an abortion (n = 49; 32%) was ‘being scared about what the abortion process involved’. The highest ranked facilitator of care was information provided to women via the abortion clinic website. The most commonly chosen number one response for potential improvement to abortion services was the option to get an early medical abortion from a general practitioner, which was chosen by 70 (45%) women.
Conclusions This study suggests that lack of knowledge and information surrounding the abortion process and the ease with which women can receive abortion care are areas of concern. Efforts are needed to reduce waiting times, to ensure that high-quality, standardised information is widely and publicly available regarding what women can expect during the abortion process, and to expand provision of early medical abortion within the community, in order to improve abortion care.
- abortion
- EMA
- medical abortion
- mifepristone
- misoprostol
- women views
- quality of abortion service
- stigma
- termination of pregnancy
Statistics from Altmetric.com
- abortion
- EMA
- medical abortion
- mifepristone
- misoprostol
- women views
- quality of abortion service
- stigma
- termination of pregnancy
Key messages
Women in Great Britain still experience personal and logistical barriers to accessing abortion services through the formal healthcare system.
A major barrier in seeking abortion is fear of what abortion involves.
Women would like shorter waiting times to access abortion care and to be able to receive it from a greater range of community providers, including general practitioners.
Introduction
It is now more than 50 years since abortion was legalised in Great Britain under the 1967 Abortion Act. In that time, there have been numerous clinical developments in abortion care, including the introduction of surgical abortion under local anaesthesia1 and medical abortion using mifepristone and misoprostol.2 Additionally, there have been refinements in service delivery for medical abortion in the first 9 weeks of pregnancy, with more self-management of the process, including home administration of misoprostol3 and simplified follow-up methods such as self-assessment of the procedure’s success using low-sensitivity urine pregnancy tests at home.4 Nevertheless, a qualitative study from 2018 indicated that as many as 519 women who reside in Britain had contacted the non-profit organisation 'Women on Web' over a 4-month period to try to access medical abortion drugs via the internet.5 The reasons given for trying to access abortion in this way highlighted personal and logistical barriers faced by women through the British healthcare system. These barriers included work commitments that impact ability to attend clinic appointments, lack of information about how to access abortion services, distance to clinic, and long waiting times.5
Qualitative research from Scotland among women living in Edinburgh and the surrounding region who had an early medical abortion (EMA) demonstrated high social acceptability of EMA at home, yet the women reported that they would benefit from abortion services being even more accessible.6 Other research among women in a remote and rural part of Scotland found that alongside travel difficulties faced when accessing abortion care, stigma surrounding abortion and anticipation of a traumatic experience also deterred women from seeking abortion care.7 A 2017 systematic review highlighted lack of consistency and agreement surrounding indicators of quality abortion care; ‘high-quality service provision’ mainly relates to the technical act of performing an abortion, rather than the sociocultural facets of healthcare provision. This indicates that with evidence-based development of key indicators of quality care, both the standard of care and women’s experiences of abortion care will be improved.8
These studies indicate that despite recent improvements to abortion care throughout Scotland and the rest of Great Britain, there is still a need to remove barriers that impede access to abortion and develop initiatives to further improve access and establish a more woman-centred approach to service provision.
The aim of this study was to determine the views of women seeking abortion on current perceived barriers to, and facilitators of, accessing abortion and on future improvements that could enhance the quality of abortion care. The study was conducted in the Chalmers Centre, a National Health Service (NHS) community abortion service in Edinburgh which is the main provider of abortion care in the region; each year over 2000 women present for abortion care at this service.9
Methods
Self-administered anonymous questionnaires were distributed to women presenting for abortion care at Chalmers Sexual Health Centre, NHS Lothian between 13 March and 24 April 2018.
Clinic reception staff were trained in the study requirements and distributed the questionnaires to attendees of specialist clinics for women requesting an abortion. Questionnaires were given to women who were aged 16 years and over, able to read or speak English to the level required for participation, and who did not appear overly distressed or agitated during clinic attendance. The clinic staff emphasised that participation had no bearing on the treatment that participants received and that they should not feel obliged to complete the questionnaire. Women completed the questionnaires before leaving the clinic and placed them in an opaque envelope within a closed collection box in the waiting room. Women could choose to return a partially completed, or completely blank, questionnaire. The questionnaire was anonymous and no identifying information was collected. Questionnaires were numbered in order to calculate distribution and completion rates.
Questionnaires were short and consisted of questions that required women to tick/circle the most appropriate answer, or rank options from a predefined list with three free-text answers, where additional comments could be entered (online supplementary material 1). The questionnaire enquired about barriers and facilitators to the women’s visit to clinic, future developments, and collected simple demographics from the participant (e.g, age, reproductive history). Predefined lists of options for barriers/facilitators and future improvements were developed based on a review of the existing literature and from the abortion service clinical staff feedback and the clinic’s Patient and Public Involvement (PPI) group, who reviewed the questionnaire.
Supplemental material
Ethical approval was granted by Research Ethics Committee Wales 5 (18/WA/0075) and NHS Lothian Research and Development (2018/0040). The local Quality Improvement Team at Chalmers Centre also reviewed the study before commencement and gave their approval.
Completed questionnaires were coded and data were entered into a secure Microsoft Excel database, where Excel formulae were used to analyse data using descriptive statistics and to determine correlation. GraphPad Prism 7 software (GraphPad Software, La Jolla, California, USA) was used to make comparisons using Fisher’s exact tests; p values <0.05 were considered statistically significant.
Patient and public involvement
The draft questionnaire was piloted within the PPI group and some changes to improve the clarity of the questionnaire were made as a result. A lay summary of the results from the questionnaire was uploaded onto the Chalmers service website so that participants could access the findings.
Results
A total of 246 women attended the service requesting an abortion over the study period. Questionnaires were only distributed on the days that trained clinic staff were present and so were distributed to 165 (67%) women over the period. A total of 154 (93%) questionnaires were completed and returned. The demographics of the respondents are shown in table 1; the median age of women was 26 years, with ages ranging from 16 to 49.
Demographics of the study population (n=154).
Barriers to seeking abortion services
“We want to know what difficulties you may have faced in the lead up to seeking our abortion services.”
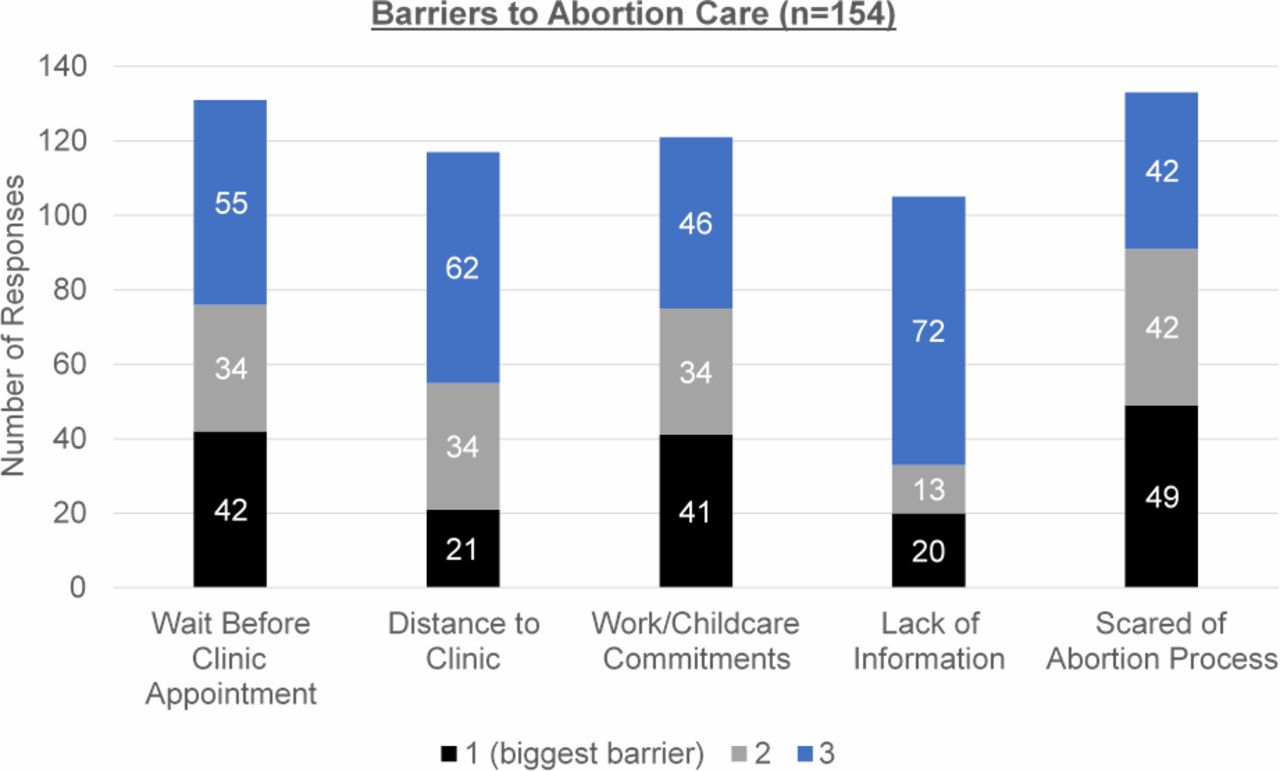
Question 1 asked women to rank potential barriers to abortion care from a list of five commonly cited barriers.5 Women were asked to rank the options as 1, 2 or 3, where a ranking of ‘1’ was indicative of the most difficult barrier. Though asked to rank three options, many women attributed a ranking of 1, 2 or 3 to more than one barrier; all responses are included.
As seen in figure 1, the most commonly ranked barrier was fear of what the abortion process would involve, with a total of 133 women (86% of respondents) indicating that this was a barrier. Of these 133 women, 49 (39%) indicated that fear of the abortion process was the most difficult barrier (ranked as ‘1’) that they faced in the lead up to seeking abortion services. The wait to get an appointment at the clinic and work/childcare commitments were the second and third most commonly ranked barriers.

Graph showing the responses received from 154 women to Question 1 of the questionnaire, which asked them to rank the barriers they faced in the lead up to seeking abortion serivces; a ranking of 1 equates to the biggest barrier faced.
A significantly higher proportion of women who reported that they had never had a previous abortion indicated that fear of the process was the most difficult barrier (ranked as ‘1’) when compared with women who had previously had an abortion (73% vs 27%, respectively, p=0.033). There were no correlations between the other responses to this question and the demographic characteristics recorded.
Facilitating factors
“We would like to know if any of the following made seeking our abortion service easier for you?”
Question 2 asked women to indicate whether they found a selection of abortion service aspects helpful, not helpful, or neither, by circling the answer that corresponded most closely to how they felt. Table 2 shows the results; over 80% of women indicated that the ability to self-refer to the clinic, the information on the abortion service website, and the text message reminder of their appointment were helpful aspects of the service. One hundred women (65%) indicated that they found the option to self-administer misoprostol at home as part of EMA helpful. There was no correlation between the responses to this question and any of the demographic characteristics recorded.
Responses to Question 2 of the questionnaire, which asked women whether they found facilitating factors helpful when seeking abortion services (n=154).
Future improvements to abortion services
“What FUTURE developments would improve the care of women seeking abortion in Scotland, in your opinion?”
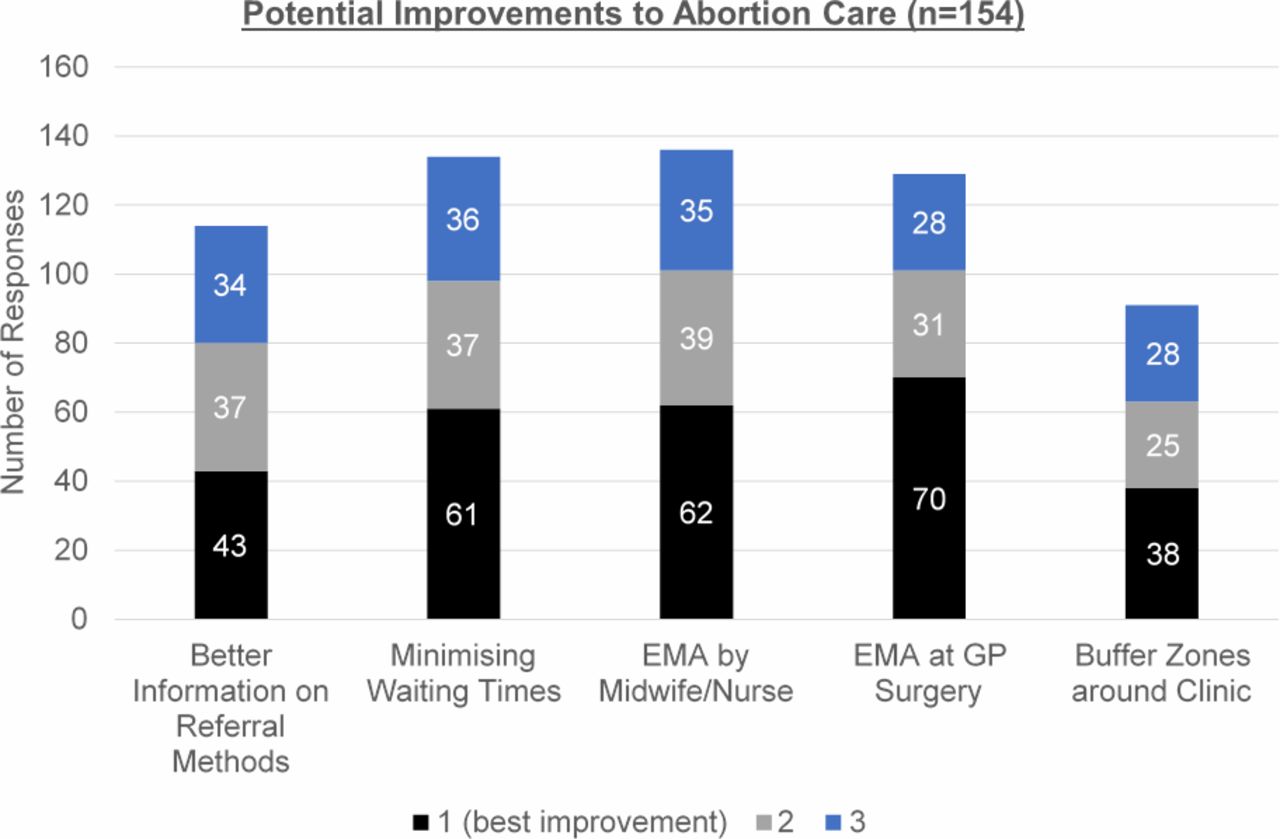
Question 3 asked women to indicate possible future developments that may improve the current service; a ranking system as in Question 1 was used. Again, some women ranked more than one option as 1, 2 or 3, and so all of these responses are included. As seen in figure 2, the ability to access EMA care directly from a nurse/midwife was the potential improvement that most women indicated would be beneficial, with 136 (88%) of respondents ranking it. Of these 136 women, 62 (46%) women considered this option the top-ranking improvement that they would like to see.

{kind=link}
{kind=link}
Graph showing the responses received from 154 women to Question 3 of the questionnaire, which asked them to rank the improvements they would benefit from within the abortion serivces; a ranking of 1 equates to the best improvement. EMA, early medical abortion.
Minimising the waiting time before the first clinic visit, and the ability to access EMA via a general practitioner’s (GP) surgery were the next most commonly chosen options, with 134 (87%) and 129 (84%) women ranking these (as either ‘1’, ‘2’ or ‘3’), respectively.
Overall, the possibility of accessing EMA via a GP’s surgery was the option that received most top rankings of ‘1’ with 70 (45%) women ranking it as such.
Three (2%) women indicated that they had witnessed anti-abortion protestors outside Chalmers Clinic. Despite this low number, 91 (59%) women considered ‘buffer zones’ around abortion clinics a welcome potential improvement.
There was no statistically significant correlation between the responses to this question and any of the demographic characteristics recorded.
Discussion
Fear of the abortion process was reported most frequently as the top-ranked barrier to seeking abortion. A significantly higher proportion of women who had not previously had an abortion indicated this as the most difficult barrier, when compared with women who had previously had an abortion. As fear is still a marked barrier among all women, this might suggest that some irreducible, natural fear is present, and that fear does not solely arise from facing the unknown. However, the fear arising from facing the unknown may stem from a lack of public information about abortion and from social stigma. Lack of information regarding the process of abortion has been reported to contribute to a delay in seeking care in around 22% of women who present for termination in the second trimester of pregnancy,10 putting women at greater risk of clinical complications,11 and this could possibly be improved by making accurate, standardised information more easily available and widely publicised. Stigma around abortion is known to be responsible for delay in seeking care.11
All the barriers listed in the questionnaire were ranked by a proportion of women as one of the top three barriers that they had faced, in particular the waiting time before women could be seen at a clinic to discuss the request to have an abortion. This highlights that once women have made the decision to end a pregnancy, perceived prolonged waiting is distressing. During the study period, the waiting times to be seen at the clinic were within the recommended waiting times (referral to assessment within five working days) of the Royal College of Obstetricians and Gynaecologists.12 Strategies to further reduce unnecessary delays between referral and consultation for abortion are therefore required. Moreover, for women who struggle with work and childcare commitments, services could consider the introduction of evening consultations to offer greater flexibility.
The study confirmed that facilitators to accessing an abortion include the ability to self-refer, being sent a text message reminder of an appointment, and the availability of information about abortion prior to the consultation that is available on the abortion clinic website.
Despite all options for improvement being highly ranked, this study found that women would particularly like the opportunity to access EMA care through other healthcare professionals, such as nurses/midwives and their GP. These responses suggest that many women wish to eliminate the need to have to see both a doctor and a specialist abortion clinic. The option to include a wider range of healthcare professionals in abortion care is recommended by the WHO.13 In addition, as EMA does not require any surgical training, a variety of healthcare professionals can provide this treatment. The most frequently top-ranked potential improvement was the ability to access EMA from the GP, with almost half of all participants ranking this as the best (number ‘1’) future improvement for abortion care; this is a model of service delivery that works efficiently in countries such as France and the Netherlands.14 While Scottish legislation now allows for misoprostol to be taken in a patient’s home, it does not permit mifepristone to be provided from GP premises or for non-doctors to prescribe abortion medication.3 If GPs, midwives and nurses could all provide abortion care (as women in this study would like) it would not only increase the accessibility of abortion services, but the wider range of healthcare providers would contribute to normalising the abortion process and lessening stigma.15
EMA with self-administration of misoprostol at home3 and self-assessment of the success of the procedure9 has vastly decreased the ‘body work’ that is required of healthcare professionals during abortion care,16 potentially making it more acceptable for a wider range of healthcare professionals to provide the services. In light of this, the views of GPs, nurses and midwives in the UK on potentially providing medical (and surgical) abortion care should be investigated. Surprisingly, although the introduction of buffer zones was ranked positively by over half of women, very few women had first-hand experience of protestors outside the clinic.
A strength of this study is the good response rate, and demographic similarity between participants and the wider population of women requesting abortion care in the region.17 It is possible, however, that this study may not represent the opinions of women seeking abortion care in other parts of Scotland, including rural and remote areas – this is a limitation of a single-site study within a city centre where NHS healthcare is provided. Additionally, women with poor English skills were excluded from this study. Therefore, opinions of these minority groups are not represented in this research; this provides an area of focus for future studies. Future research should also examine women’s views on improvements in surgical abortion care, despite medical abortion being the most common method of abortion in Scotland (90.1% of all abortions in 2017).18
Although the questionnaire used predefined lists of options based on current literature and had input from a PPI group, a drawback was its inability to capture novel opinions or women’s reasons for their rankings. Further qualitative research in this area would provide important opportunities to receive and understand women’s unique opinions on this topic.
Conclusions
Although there have been many improvements to abortion care in Great Britain since the legalisation of abortion, this study shows that women would like shorter waiting times to access abortion care and to access it from a greater range of community providers.
Acknowledgments
The authors wish to thank Anne Johnstone for overseeing the running of the project and for facilitating patient and public involvement (PPI), the clinic staff who distributed the questionnaires, and the women who participated in this study.
Footnotes
Contributors SC conceived the idea for the research, supervised the project and helped edit the paper. JLS developed the questionnaire, conducted the research and the analysis, interpreted the data, and drafted the paper. Both authors approved the final draft of the paper.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.