Article Text

Abstract
Background Data on utilisation of in-facility second-trimester abortion services are sparse. We describe temporal and geographical trends in utilisation of in-facility second-trimester abortion services across Mexico.
Methods We used 2007–2015 data from Mexico’s Automated Hospital Discharge System (SAEH) to identify second-trimester abortive events (ICD O02-O08) in public hospitals across Mexico’s 32 states. We described utilisation, calculated rates using population data, and used logistic regression to identify woman- and state-level factors (municipality-level marginalisation, state-level abortion law) associated with utilisation of second-trimester versus first-trimester services.
Results We identified 145 956 second-trimester abortions, or 13.4% of total documented hospitalizations for abortion between 2007 to 2015. The annual utilisation rate of second-trimester abortion remained constant, between 0.5 to 0.6 per 1000 women aged 15–44 years. Women living in highly marginalised municipalities had 1.43 higher odds of utilising abortions services in their second versus their first trimester, when compared with women in municipalities with low marginalisation (95% CI 1.18 to 1.73). Living in a state with a health or fetal anomaly exception to abortion restrictions was not associated with higher utilisation of second-trimester abortion services.
Conclusions Our results suggest there is a need for all types of second-trimester abortion services in Mexico. To improve health outcomes for Mexican women, especially the most vulnerable, access to safe second-trimester abortion services must be ensured through the implementation of current legal exceptions and renewed attention to the training of healthcare providers.
- abortion
- statistics
- epidemiology
- service delivery
- reproductive health politics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The need for second-trimester abortion services does not diminish, even with expansion of first-trimester abortion services.
Poorer, younger women are more at risk for second-trimester abortion (versus first-trimester).
States with health and fetal anomaly legal exceptions do not have higher utilisation of second-trimester abortion services, indicating under-utilisation of these legal exceptions.
Introduction
Overall, 10%–15% of abortions worldwide occur in the second trimester, yet they account for a disproportionate number of maternal deaths when provided under unsafe conditions.1–3 Reasons women need second-trimester abortion services vary, but include late diagnosis of fetal anomalies, delays in recognition of pregnancy, newly diagnosed or worsening maternal health conditions, and delays associated with access to care.2–4 Access to safe second-trimester abortion is an essential part of global efforts to reduce maternal morbidity and mortality, yet access is restricted in many parts of the world.2
Two-thirds of countries with laws regulating second-trimester abortion allow it only to save the woman’s life.3 While many countries do have exceptions permitting second-trimester abortion, such as the woman’s physical or mental health, rape, fetal anomalies, or socioeconomic reasons, access to services under these exceptions varies by country.5–7 The unmet need for second-trimester abortion remains unknown since many national vital statistics systems do not specifically capture incidence of second-trimester abortions.2
In Mexico, abortion laws are determined at the state level. In Mexico City, one of Mexico’s 32 states, women have had access to first-trimester abortion in the private and public sectors since 2007.8 In Mexico’s 31 other states, abortion at all gestational ages remains restricted.7 Gestational age (GA) measures the age of a pregnancy and is reported in weeks. Rape is the only circumstance for which abortion is legally permitted at the federal level.9 Other grounds for legal access vary by state. For example, 14 states permit abortion when the health of a woman is at risk, while 16 permit abortion in cases of fetal anomalies.10
Previous research on abortion in Mexico has estimated incidence using indirect methods11–13 or focused on Mexico City’s pubic abortion programme.8 14 15 Data on in-facility second-trimester abortion is lacking; yet, it is critical to measure documented service provision in order to understand demand for abortion services and population health outcomes. We used Mexico’s hospital discharge register to describe utilisation of second-trimester spontaneous, induced, and post-abortion services, over time (2007–2015) and by state.
Methods
Data and variables
We used 2007–2015 data from Mexico’s hospital discharge system, SAEH (Subsistema Automatizado de Egresos Hospitalarios).16 Hospital discharge was defined as the exit of a patient from inpatient services (at least one night in the facility). All facilities included in this dataset are operated by national and state ministries of health (Secretaría de Salud, SSA). These facilities largely serve individuals without insurance or covered by Seguro Popular, a public insurance programme for the unemployed, self-employed, or those without access to employment-based social security.17 These government facilities accounted for an estimated 76% of the country’s total inpatient post-abortion cases in 2009.12
We built a dataset of obstetric events (births and abortions). Each discharge record includes up to six international Classification of Diagnosis Codes Version 10 (ICD-10) codes for reason for admission. We identified abortive events using ICD-10 codes O02-O08 (online supplementary web appendix table A1); we excluded ectopic and molar pregnancies with an abortive outcome, ICD-10 codes O00 and O01. We identified all types of abortion care through these hospital records; although the codes theoretically provide a way to differentiate between induced and spontaneous abortions, nearly 70% of second-trimester abortions were coded as 'O06 Unspecified abortion', making it difficult to differentiate between type of abortion. Therefore, we classified all abortive events (ICD codes O02-O08) as abortion for this analysis. In order to comprehensively capture second-trimester abortions, we also included women who had abortion codes for up to six discharge diagnosis codes (N=894; 0.6% of total sample (online supplementary web appendix table A2)). Additional abortions that may not have been identified using ICD-10 diagnostic codes were identified using a 'type of attention' checkbox in the SAEH records, which indicates whether an abortion or a delivery was performed (N=3974; 2.7% of total sample).
Supplemental material
Among the records between 2007–2015, 22% (238 972) were missing GA (online supplementary web appendix table A3). Records missing GA were disproportionately from women in less marginalised urban areas, such as Mexico City. There were few abortions identified after 20 weeks; under international and national definitions, spontaneous or induced abortions after 20 weeks are classified as 'stillbirths'.18 The SAEH records also include the following variables: age, municipality and state of residence, parity, hospital of admission, and length of hospital stay. We defined reproductive age as women aged 15–44 years.
We used 2010 population estimates of women aged 15–44 years from the Mexican government’s population agency, Consejo Nacional de Población (CONAPO),19 at the state and national level to calculate rates. We also used the 2010 municipality-level marginalisation index, a measure of community-level socioeconomic status.20 The index includes information about education, housing, income, and population density and is generated using principal components analysis.21 We classified municipalities into five groups: very low, low, medium, high, and very high marginalisation. We merged the marginalisation index into the individual-level discharge data using the residence municipality of the woman. We also categorised states into four groups based on the percentage of the population living in poverty in 2014 as reported by The National Council for the Evaluation of Social Development Policy (CONEVAL)21 and previous literature.22
We included information on state-level legal exceptions for abortion categorised as binary variables based on whether a state had exceptions for health of the woman or fetal anomaly in their penal code.10 Finally, we merged in hospital tier of specialisation (primary, secondary and tertiary).23 24 All data sources were publicly available and downloadable (online supplementary web appendix table A4).
Analysis
We calculated second-trimester abortion hospitalisation rates per year per 1000 women aged 15–44 years at the national and state levels. We mapped second-trimester abortion hospitalisation rates across Mexico by state, and by the presence of state-level health or fetal anomaly exception laws.
We next examined changes in mean and median GA of second-trimester abortions over time. We examined trends nationally and in Mexico City versus other Mexican states. Since Mexico City has legal first-trimester abortion services, we hypothesised that trends in second-trimester GA would be lower in Mexico City due to availability of first-trimester abortion.
Finally, we identified factors associated with utilisation of hospital-based second-trimester (vs first-trimester) abortion using a logistic regression model. We included age, parity, municipality-level marginalisation, state-level health and fetal anomaly exceptions, and hospital specialisation. We assessed model robustness by running models with different covariates, such as hospital bed size, women’s education, and maternal mortality rate; results were robust and we show only the final model. We estimated robust standard errors to account for non-independence of observations within hospitals using the 'cluster' option in STATA version 15 (StataCorp, College Station, TX, USA).25
Patient and public involvement
There was no patient involvement in this secondary data analysis.
Results
Among 1 083 803 induced and spontaneous abortions documented in the SAEH hospitalisation records between 2007 and 2015, we identified 145 956 (13.4%) second-trimester abortions. The majority of second-trimester abortions (70%) were classified as ICD-10 code O06 ('unspecified'). Nearly 60% of second-trimester abortions were among women aged ≤25 years, and only 2.4% occurred among women aged >40 years (table 1). Most (70%) women who had a second-trimester abortion were hospitalised for 1 day. Over 50% of reported second-trimester abortions occurred in the least marginalised municipalities (table 1). Overall, 20.2% of second-trimester abortions were performed in tertiary care hospitals, 78.4% in secondary care hospitals, and 1.4% in primary health facilities. However, in Mexico City, 51.2% of second-trimester abortions were performed in specialised hospitals, while in the poorer states of Guerrero, Oaxaca and Chiapas, only 1.6% of second-trimester abortions were performed in specialised hospitals (online supplementary web appendix table A5).
Characteristics of women receiving in-hospital second-trimester abortions, Mexico 2007–2015
The annual nationwide hospitalisation rate of second-trimester abortion services remained stable, between 0.5 to 0.6 per 1000 women of reproductive age (15–44 years) over the study period. In our spatial analysis of second-trimester induced and spontaneous abortion hospitalisations, there was clustering of higher rates of hospitalisation in the central and southern parts of Mexico (figure 1). The states of Zacatecas and Durango had the highest rates of utilisation of hospital-based, second-trimester abortion services (1.1 and 0.89 per 1000 women, respectively) followed by predominantly southern states, including Tlaxcala and Guerrero. The northeastern states, including Coahuila, Nuevo León and Tamaulipas, had some of the lowest rates of utilisation of second-trimester abortion services.
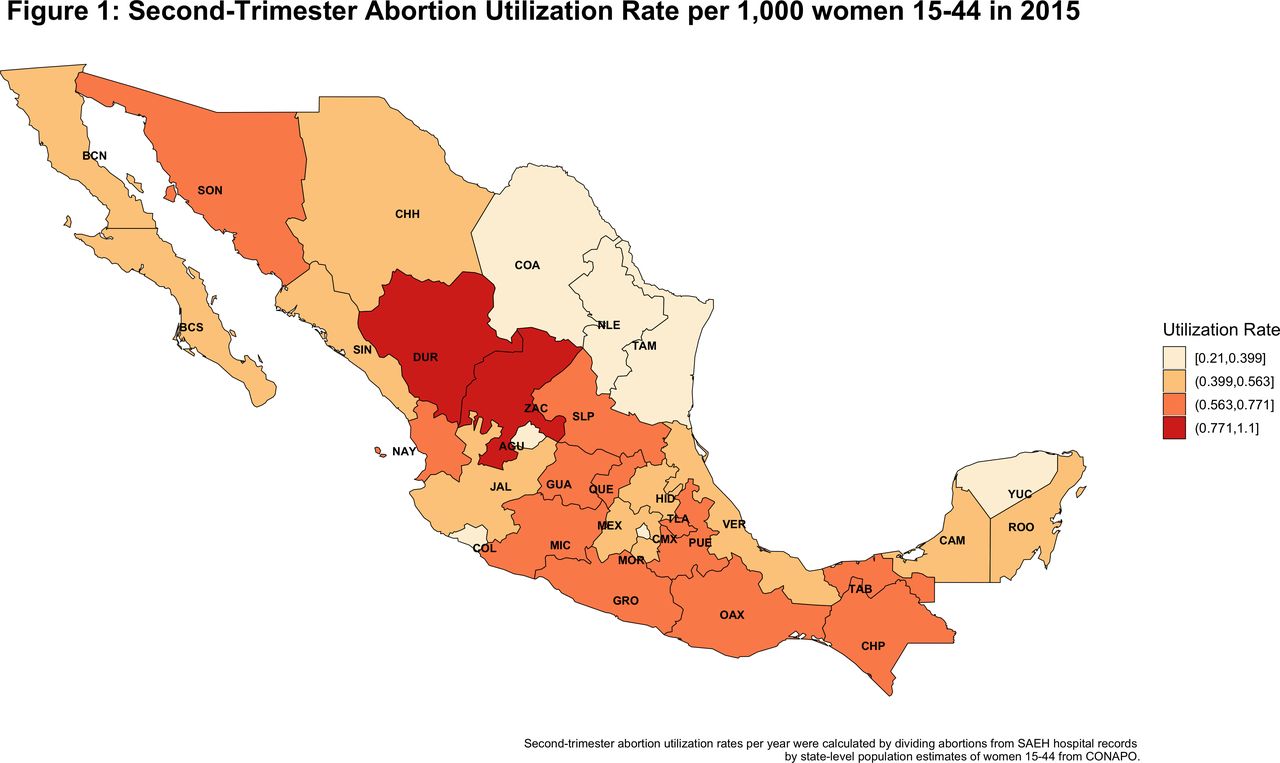
Second-trimester abortion utilisation rate per 1000 women aged 15–44 years in 2015 for individual Mexican states
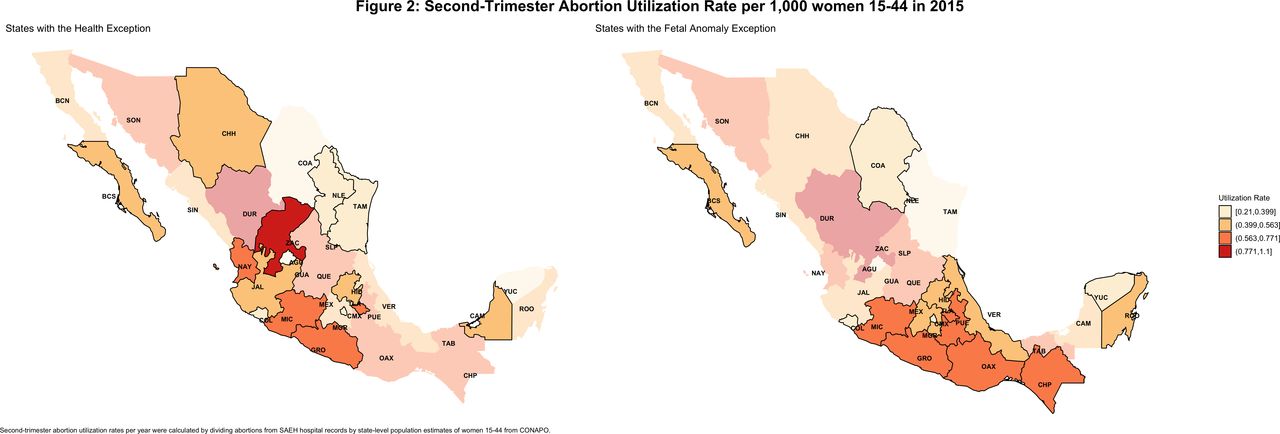
No relationship between legal exceptions that permit abortion and documented utilisation of public, hospital-based abortion services was detected. In states with a health exception (figure 2), utilisation rates of hospital-based second-trimester abortion were 0.30 to 1.10 per 1000 women; rates were similar in states without a health exception (0.2 to 0.9). Among states with fetal anomaly exceptions, the hospitalisation rater varied between 0.21 and 0.77 per 1000 women, and did not differ based on region (figure 2).

Second-trimester abortion utilisation rate per 1000 women aged 15–44 years in 2015 in Mexican states with health exceptions and fetal anomaly exceptions.
The majority (62%) of second-trimester abortions were performed between 13 and 16 weeks, 38% occurred between 17 and 20 weeks, and <1% from 21 to 24 weeks. In 2007, mean GA of second-trimester abortion patients in Mexico City was 18.11 weeks (95% CI 18.01 to 18.21), 1.82 weeks higher than the other Mexican states at 16.29 weeks (95% CI 16.25 to 16.34). In 2009, this difference narrowed to 0.12 weeks, and remained constant for the rest of the study period. However, overall mean GA remained marginally higher in Mexico City (16.6) compared with the other states (15.9) over the study period (p<0.0001).
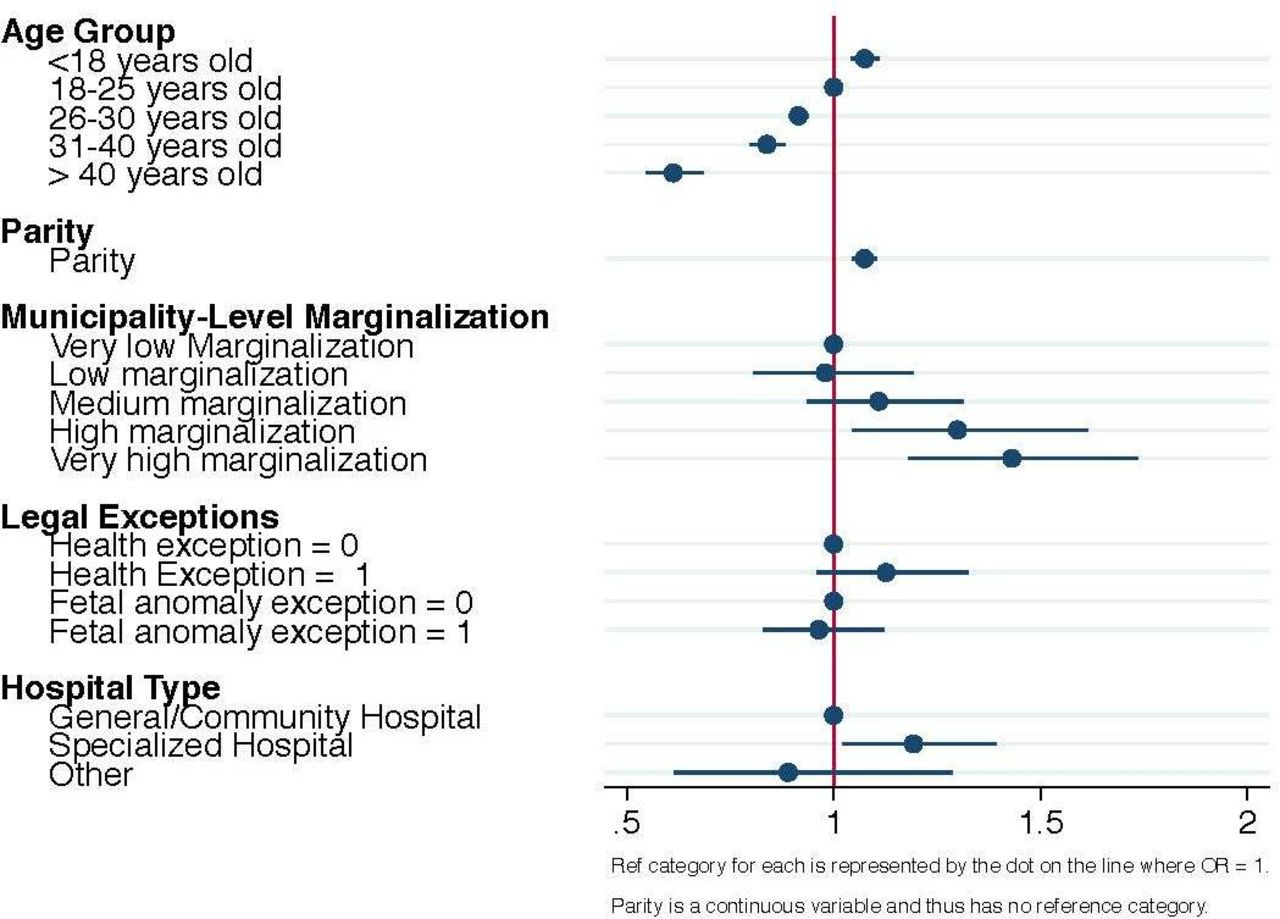
In multivariable analyses, adolescents were more likely than older women to present for abortion services in the second trimester compared with the first trimester (odds ratio (OR) 1.07, 95% CI 1.04 to 1.11) (figure 3). Women living in municipalities with high levels of marginalisation had higher odds of utilising abortion services in their second trimester versus first trimester compared with women living in municipalities with lower marginalisation (OR 1.43, 95% CI 1.18 to 1.73). Living in a state with a health or fetal anomaly exception was not associated with utilisation of second-trimester versus first-trimester services.

{kind=link}
{kind=link}
{kind=link}
Factors associated with second-trimester abortion versus first-trimester abortion care. OR, odds ratio; Ref., reference.
Discussion
In this study, we present novel data on the utilisation of second-trimester abortion services in the public sector in Mexico. We found that women seek care in health facilities for second-trimester abortion care, including spontaneous, induced, and post-abortion services, even in places where abortion is highly restricted, although not at the rates that might be expected.2 Although second-trimester induced abortion is largely illegal throughout Mexico, some women are able to access abortion services under the available exceptions; many others present for and receive post-abortion care.
We found the average hospitalisation rate for second-trimester abortions was 0.57 per 1000 women, and 13.4% of total hospital-based abortions occurred in the second trimester. Existing estimates of utilisation of abortion services in Mexico range from 7.3 per 1000 women26 to 38 per 1000 women aged 15–44 years.12 Under the assumption second-trimester induced and spontaneous abortions account for ~15% of total abortions,2 27 we might expect the utilisation of second-trimester abortion to range from 1.1 to 5.7 per 1000 women. We found consistent utilisation of second-trimester abortion services during the study period, including in Mexico City, even following liberalisation of first-trimester abortion in the capital in 2007. However, we did detect a slight decline in GA at the time of second-trimester abortion among women in Mexico City after 2007, which may be due to improved access to first-trimester abortion. Our results demonstrate the need for second-trimester abortion services remains present, even with expansion of first-trimester abortion services.
Furthermore, we found health and fetal anomaly exceptions in the state laws were not associated with higher utilisation of second-trimester abortion services. The potential under-utilisation of second-trimester abortion services may be due to poor implementation of all legal exceptions.7 For example, while Jalisco passed a law in 2009 that mandated institutions to provide abortion in cases of rape, there have only been 16 cases documented.28 This type of low utilisation was reflected in our study; women living in states with legal exceptions for health or fetal anomaly were no more likely to utilise second-trimester services than women living in states without these exceptions. There remains widespread under-utilisation of legal exceptions, likely due to lack of information and training among providers, poor dissemination of information to women, and a continued environment of criminalisation.7 29 30
Our results support other evidence that Mexico’s most vulnerable women are often disproportionately affected by obstacles to obstetric or prenatal care.14 This finding has been reflected in other settings, where younger, poorer and more disenfranchised women were more likely to seek second-trimester abortions.4 14 31–33 In our study, women in less marginalised municipalities comprised half of our sample of second-trimester abortions, but had lower odds of presenting for second-trimester (versus first-trimester) abortion services. Adolescents had higher odds of presenting for second-trimester (versus first-trimester) abortion services when compared with older women.
Our study has limitations; Mexico is among a few low- and middle-income countries with robust health information systems, but secondary health services data are limited. We included all abortions – spontaneous and induced – and were not able to differentiate between them. Second, this is not a study of second-trimester abortion incidence, but of documented utilisation in the public sector. Our results may not be generalisable to private or employment-based health sectors or abortions that occur out-of-facility.34–36 The SAEH data contain limited individual-level sociodemographic information; we leveraged other data sources with facility, municipality and state-level characteristics to partially address this limitation of the data. Fourth, in our comparison of women seeking first-trimester versus second-trimester abortions, our sample of first-trimester abortions is limited by the fact that it does not include any outpatient services from Mexico City’s legal first-trimester abortion programme. However, we found similar results when running our model with and without data from Mexico City. In addition, 22% of records were missing GA; improvements in the documentation of GA would increase our understanding of the timing of abortion in Mexico.
In our study, we leveraged objective clinical data to report on in-facility second-trimester spontaneous and induced abortion across the public sector in a low- and middle-income country where abortion is restricted. We found the average hospitalisation rate for second-trimester abortions was 0.57 per 1000 women, and 13.4% of total hospital-based abortions occurred in the second trimester. We highlight there is a need for second-trimester abortion services in Mexico. To improve health outcomes for Mexican women, especially the most vulnerable, access to safe second-trimester abortion services must be ensured through the implementation of current legal exceptions and renewed attention to provider training.
Footnotes
Funding BGD was supported by Society of Family Planning awards SFPRF11-02, SFPRF10-II2-2, R01HS025155 (Cottrell, PI), and grant number K12HS022981 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Linked Articles
- Highlights from this issue