Article Text

Statistics from Altmetric.com
1. Purpose and scope
This document updates previous Faculty of Sexual & Reproductive Healthcare (FSRH) guidance and aims to summarise the available evidence and expert opinion on combined hormonal contraception (CHC). The guideline is intended for use by healthcare practitioners (HCPs) providing CHC.
2. Identification and assessment of the evidence
This guideline was developed in accordance with standard methodology for developing FSRH clinical guidelines. The recommendations made within this document are based on the best available evidence and the consensus opinion of experts and the guideline development group (GDG). The methodology used in developing this guideline and a list of GDG members and other contributors can be found in Appendix 1.
Appendix 1
The recommendations included should be used to guide clinical practice but are not intended to serve alone as a standard of medical care or to replace clinical judgement in the management of individual cases.
3. Introduction
CHC has been used by women worldwide for almost 60 years, with significant changes in dosage and preparation over time. Millions of UK women choose to use CHC. The Natsal 3 survey1 carried out in 2010–2012 reported that more than a third of UK women aged 16–44 years had used oral contraception (OC) in the last year (no distinction was made between combined oral contraception (COC) and the progestogen-only pill (POP)), but data from the Office for National Statistics (2008/09)2 indicate that the majority of women using OC choose COC.2
HCPs should support women to make informed decisions about choosing and using CHC, ensuring that they are informed about contraceptive effectiveness (and how this compares to other contraceptive methods) as well as potential risks and benefits.
Extrapolation of COC data to inform recommendation on all CHC methods
Unless stated otherwise, the recommendations for COC in this guideline refer to low-dose COC containing ≤35 μg ethinylestradiol (EE) combined with a progestogen. Recommendations are the same for all COC formulations, irrespective of their progestogen content. Data relating to COC containing estradiol are very limited; recommendations for these preparations are currently as for EE-containing COC.
Limited information is available on the short- and long-term safety of the combined transdermal patch (CTP) and combined vaginal ring (CVR); most of the available studies were sponsored by the manufacturers. After reviewing the available evidence, the GDG considers that recommendations for COC can be extrapolated to include CTP and CVR, unless stated otherwise.
4. Summary, including changes to existing guidance
CHC contains an estrogen and a progestogen delivered as a pill (COC), transdermal patch (CTP) or vaginal ring (CVR).
Contraceptive effectiveness: CHC is highly user-dependent. If used perfectly, the risk of CHC contraceptive failure is low (<1%), but with typical use it is estimated that 9% of women have unplanned pregnancies in the first year of CHC use. Effectiveness could also be affected by drug interactions (all CHC methods) and malabsorption (COC only); the CTP could be less effective in women weighing >90 kg. See Section 7.
Health risks: The increased risk of serious health events, including venous and arterial thromboembolism, breast cancer and cervical cancer associated with current or recent use of CHC is small, but is greater than that with progestogen-only or non-hormonal contraception.
Levonorgestrel (LNG), norethisterone (NET) and norgestimate COC are associated with a lower risk of venous thromboembolic events than COC containing newer progestogens, the CTP and the CVR. COC containing higher EE doses may be associated with greater risk of arterial thrombotic events than lower EE doses. See Section 10.
Health benefits: Ever-use of CHC is associated with a reduced risk of endometrial, ovarian and colorectal cancer; other non-contraceptive benefits of CHC use include predictable bleeding patterns, reduction in menstrual bleeding and pain, and management of symptoms of polycystic ovary syndrome (PCOS), endometriosis and premenstrual syndrome. See Section 9.
Side effects: CHC use – and the hormone-free interval (HFI) – can be associated with side effects including mood change, headache and unscheduled bleeding. There is no one CHC formulation that is associated overall with fewest unwanted nuisance effects. See Section 11.
CHC regimens: The traditional 21/7 CHC regimen with a monthly withdrawal bleed confers no health benefit over other patterns of CHC use. In addition, symptoms associated with the HFI can be problematic and ovarian activity during a 7-day HFI could risk escape ovulation (particularly with lower doses of EE and if use is not perfect). This guideline highlights the fact that ‘tailored’ CHC regimens in which there are fewer (or no) HFI and/or shortened HFI can be safely used to avoid withdrawal bleeds and associated symptoms and theoretically reduce the risk of contraceptive failure. Suggested tailored regimens (using a monophasic EE CHC) are described. Women should be told about tailored regimens and given their choice of regimen based on their preference. See Section 6.
Medical eligibility: Contraindications to use of CHC are unchanged in this guideline, in line with United Kingdom Medical Eligibility Criteria (UKMEC) 2016. Women aged over 50 years should generally use safer alternative contraception. Information and checklists are provided to support clinicians with assessment of medical eligibility for CHC. The guideline notes that appropriate self-assessment medical questionnaires can be safe and useful tools that may also facilitate remote prescribing; advice is given about obtaining blood pressure and body mass index (BMI) measurements. See Section 12.1.1.
Concomitant use of other drugs: Hepatic enzyme-inducing drugs could reduce the contraceptive effectiveness of all CHC methods. Contraceptive hormones can affect serum levels of drugs such as lamotrigine with potential significant clinical effects. Women using teratogenic medications should be encouraged to use the most effective long-acting reversible contraception (LARC) methods. See Section 7.2.3.
Choice of contraceptive method, CHC formulation and CHC regimen: A woman requesting CHC who is medically eligible should be given information about the contraceptive effectiveness of CHC and alternatives including LARC. If CHC is the preferred option, a COC containing ≤30 µg EE in combination with LNG or NET is a reasonable first-line option to minimise venous thromboembolism (VTE) risk; women may choose other preparations or routes of administration depending on their past experience of side effects and personal preference. Non-oral CHC may be considered if there are concerns about absorption of COC. Women should be given the option of standard or tailored CHC regimens. See Section 12.
Starting CHC and supporting information: Charts and information boxes are provided to guide starting CHC (see Section 6.3) and to support clinicians with informing women as to how to take CHC, what to do if they make a mistake (see Section 8) and symptoms/new medical diagnoses that should prompt them to seek medical advice (see Box 4). Specific advice is given regarding CHC use during travel, at high altitude, and during times of prolonged immobilisation (see Section 14).
Provision of CHC: Up to a year’s supply of CHC may be prescribed at the first consultation. See Section 12.6.
Follow-up: Annual follow-up with review of medical eligibility, drug interactions, compliance and consideration of alternative contraception including LARC is recommended as routine. See Section 13.
Stopping CHC: CHC use is not associated with a delay in return to fertility after stopping (see Section 11.6). Guidance is given (see Table 3a and Table 3b) to support switching from CHC to other contraceptive methods. There is no arbitrary maximum period of CHC use. Repeated stopping and starting of CHC should be discouraged because of thrombotic risk (see Section 10.1). Medically eligible women who are aware of effectiveness and associated health risks may choose to continue CHC for contraception until age 50 years (see Section 15). CHC may be of benefit for menopausal symptoms and maintenance of bone mineral density (BMD) in perimenopausal women aged under 50 years who also require contraception.
5. What is combined hormonal contraception?
5.1 Hormonal content of combined hormonal contraception
CHC contains an estrogen paired with a progestogen in different formulations.
5.1.1 Estrogens
In the UK, the majority of COC as well as the CTP and CVR, contain between 20 μg and 35 μg of the synthetic estrogen, EE. Current ‘low-dose’ COC was developed to reduce the health risks associated with the high estrogen content of COC in the 1960s and 1970s.3 A COC product containing the synthetic estrogen, mestranol (metabolised to EE) is also available (50 μg mestranol roughly equates to 35 μg EE).4
COC has been introduced that contains 17β-estradiol, structurally identical to that which occurs naturally in humans. Theoretically, estradiol COC could have improved safety profiles compared to formulations containing EE or mestranol due to reduced thrombotic and metabolic effects.5 This has not yet been established: although limited evidence suggests that estradiol COC is safe to use and highly effective in preventing unintended pregnancy,6 further research will be required to assess the safety profile of estradiol COC relative to that of EE COC.
5.1.2 Progestogens
Progestogens are synthetic steroids designed to have some of the properties of progesterone. The synthetic progestogen component of CHC allows convenient dosing intervals, potent suppression of ovulation, and prevents over-proliferation of the endometrium in response to estrogen. Newer progestogens were developed to have fewer androgenic and glucocorticoid effects; some are anti-androgenic and have potentially favourable anti-mineralocorticoid effects.7
However, different progestogens may modify the effect of EE on hepatic clotting factors differently; CHC containing some newer progestogens in combination with EE appear to be associated with greater risk of VTE than COC containing other progestogens. See Section 10.1.1.
The progestogens that are components of CHC are sometimes grouped by ‘generation’, according to the time they were first marketed as constituents of COCs.7,8 (note that classification varies).
First: norethisterone (NET)
Second: levonorgestrel (LNG)
Third: desogestrel, gestodene, norgestimate*
Newer/other: drospirenone (DRSP), dienogest, nomegestrol acetate
(*sometimes classified as second generation: LNG is one of its active metabolites).
Norelgestromin is a metabolite of norgestimate; etonogestrel is the active metabolite of desogestrel.
Co-cyprindiol (containing 35 μg EE with cyproterone acetate, an anti-androgen) is indicated for management of moderate to severe acne and hirsutism. Women using co-cyprindiol for these indications do not require additional contraception.9
5.2 What methods of CHC are available in the UK?
There are currently three methods of CHC available in the UK:
Combined oral contraceptive pill (COC)
Combined transdermal patch (CTP) that releases an average of 33.9 µg EE and 203 µg norelgestromin per 24 hours.10
Combined vaginal ring (CVR) that releases EE and etonogestrel at daily rates of 15 µg and 120 µg, respectively.11
Monophasic verses multiphasic COC
The majority of COC products in the UK are monophasic; that is, all pills in the packet contain the same dose of estrogen and progestogen. Multiphasic (variable dose) COC is also available in which the dose of either or both steroid hormones varies during the pill cycle.
Cochrane Reviews of randomised controlled trials (RCTs) comparing monophasic with biphasic, triphasic and quadriphasic COC regimens identified extremely limited evidence.12–15 The COC regimens studied differed not only because they were differently phasic, but also contained different progestogens. For example, the only quadriphasic preparation studied contained estradiol valerate which was compared with a monophasic preparation containing EE. Evidence is inadequate to establish whether multiphasic COC differs significantly from monophasic COC in terms of bleeding patterns, side effects, discontinuation rates or effectiveness in preventing pregnancy. As the existing evidence suggests no particular advantage associated with multiphasic preparations, the GDG recommends that monophasic COC should be used first-line.
5.3 How does CHC work?
The primary mechanism of action of CHC is prevention of ovulation. CHC acts on the hypothalamo-pituitary-ovarian axis to suppress luteinising hormone (LH) and follicle-stimulating hormone (FSH) and thus inhibit ovulation.16–19 Changes to cervical mucus, endometrium and tubal motility that result from progestogen exposure may also contribute to the contraceptive effect.
6. How is CHC used?
Key information
✓ Tailored CHC regimens can reduce the frequency of withdrawal bleeds and can reduce withdrawal symptoms associated with the hormone-free interval (HFI); however, unscheduled bleeding is common.
Clinical recommendations
✓ Women should be given information about both standard and tailored CHC regimens to broaden contraceptive choice.
✓ Women should be advised that use of tailored CHC regimens is outside the manufacturer’s licence but is supported by FSRH.
✓ Women should have access to clear information (either written or digital) to support tailored CHC use.
Traditional (standard) 21/7 CHC cycles were designed to induce a bleed each month, mimicking naturally occurring menstrual cycles. There is, however, no health benefit from a monthly withdrawal bleed, and the 7-day HFI has the following drawbacks:
Withdrawal bleeding may be heavy, painful or simply unwanted.
The HFI may be associated with symptoms such as headache and mood change.
Ovarian suppression is reduced,20–26 and follicular development occurs during the HFI, particularly with COC containing lower EE doses.20–23 Errors in pill-taking (or patch or ring use) around the HFI could result in extension of the HFI, risk of ovulation, and thus potential risk of pregnancy.
Tailored (non-standard) CHC regimens reduce the frequency of HFI (extended regimens), abolish the HFI (continuous regimens) and/or shorten the HFI. Using tailored regimens, women can reduce or avoid HFI-associated symptoms and could potentially reduce the risk of escape ovulation and resulting contraceptive failure. Such regimens are as safe and as effective for contraception as standard 21/7 regimens.27,28
The GDG recommends that the tailored CHC regimens suggested in Section 6.2.1 can be offered as an alternative to 21/7 CHC regimens to widen contraceptive choice. Women should have access to clear information (either written or digital) to support tailored CHC use.
6.1 Standard CHC regimens
6.1.1 Combined oral contraception
The majority of COC in the UK is designed to be taken as 28-day cycles, with 21 consecutive daily active pills followed by a 7-day HFI prior to starting the next packet of pills. The first seven pills inhibit ovulation29 and the remaining 14 pills maintain anovulation. Traditionally women have then either had seven pill-free days or taken seven placebo tablets; during this HFI, most women will have a withdrawal bleed due to endometrial shedding. It should be made clear to women that this bleed does not represent physiological menstruation and that it is has no health benefit.
6.1.2 Combined transdermal patch
One patch is applied to the skin and worn for 7 days to suppress ovulation. Thereafter the patch is replaced on a weekly basis for two further weeks. The fourth week is patch-free to allow a withdrawal bleed. A new patch is then applied after seven patch-free days.
6.1.3 Combined vaginal ring
One ring is inserted into the vagina and left in place continuously for 21 days. After a ring-free interval of 7 days to induce a withdrawal bleed, a new ring is inserted.
6.2 Tailored CHC regimens
Tailored CHC regimens include:
Continuous use of CHC (no HFI)
Extended use of CHC (less frequent HFI); timing of HFI can be fixed or flexible
CHC regimens in which the HFI is shortened (the shortened HFI may be taken after each 21 days of CHC use or incorporated into an extended regimen).
In continuous or extended CHC regimens, CHC is taken for more than 21 consecutive days without a HFI. Such regimens have the potential advantage of eliminating or reducing the frequency of withdrawal bleeding and associated symptoms; bleeding pattern is, however, unpredictable. Less frequent HFI could also reduce the risk of escape ovulation20 and (potentially) contraceptive failure.
A shortened HFI, offering more continuous ovarian suppression, could also reduce the risk of escape ovulation,20 particularly if CHC use is imperfect around the HFI. A shortened HFI can be taken after every 21 days of active CHC or incorporated into an extended regimen.
6.2.1 Suggested tailored CHC regimens
A variety of regimens have been studied; however, data are currently too limited to recommend one approach over another. In some countries (but not the UK) COC are available that are intended to be taken as an 84/7 regimen, with a 3-monthly HFI. In the UK, some monophasic 24/4 COC regimens are marketed30,31 and one quadriphasic COC with a 2-day HFI is available.32 The FSRH supports off-label use of tailored CHC regimens such as those detailed in Table 1 using monophasic CHC that are licensed to be taken as a 21/7 regimen. If the preparation includes placebo pills, these should be omitted. Multiphasic COC should not be used in tailored regimens.
Standard and tailored regimens for use of combined hormonal contraception (CHC)
6.2.2 Contraceptive effectiveness of tailored CHC regimens
How does contraceptive effectiveness of tailored regimens compare with standard regimens?
It has been suggested that reducing the frequency of the HFI, abolishing the HFI and/or shortening the HFI could reduce the risk of escape ovulation and resulting contraceptive failure.
The findings of studies that consider the contraceptive effectiveness of tailored CHC regimens compared to one another and to standard 21/7 regimens are difficult to bring together because they consider different CHC formulations (different doses of estrogen, different progestogens) and different regimens. In addition to very limited direct data from studies with pregnancy as an outcome, indirect evidence is available from studies that consider ovarian activity during HFI of various lengths as a marker of potential risk of pregnancy.
On the basis of the available evidence (summarised below), the GDG considers that extended or continuous CHC regimens and shortened HFI could theoretically reduce risk of escape ovulation compared with standard CHC regimens, but that there is not conclusive evidence of greater contraceptive effectiveness.
Studies considering ovarian activity in the HFI as an indication of risk of pregnancy
A standard 7-day HFI is associated (in most studies) with more hypothalamic-pituitary-ovarian axis activity than a shortened, 3- or 4-day HFI.24,25,33–36 Ovarian activity has been observed to be significantly lower with continuous COC than with standard 21/7 regimens.37,38 It has therefore been suggested that a regimen including a HFI shorter than 7 days could reduce the risk of pregnancy resulting from escape ovulation.
Imperfect use of CHC in the days around the HFI could in effect extend the HFI. A systematic review39 identified 10 biomedical studies that reported on risk of ovulation with a deliberately extended HFI. Findings varied: five studies observed no ovulations with extended HFI up to 14 days; in the other five studies, presumed ovulations were documented with HFI between 8 and 11 days long. All studies involved small numbers of women and used different definitions and indicators of ovulation. A shorter HFI could theoretically reduce the risk of ovulation if CHC use around the HFI is imperfect.
One small RCT found that endogenous estradiol levels increased more quickly during the HFI after extended (84/7) COC use than in a 21/7 regimen.40 The authors postulated, but did not demonstrate, that escape ovulation could occur earlier with extended than with standard COC regimens.
There is limited evidence that ovarian activity in the HFI could be more pronounced in obese women. In one study41 hormone profiles at the end of a 7-day HFI in 10 women with normal BMI and 10 women with obesity noted estradiol levels consistent with dominant follicles and progesterone levels consistent with ovulation in more women with obesity than women with normal BMI. A further study42 of women with obesity who were initially taking 20 μg EE COC in a 21/7 regimen and were then randomised to either a continuous regimen of 20 μg EE COC or to 30 μg EE COC as a 21/7 regimen noted that both options decreased evidence of a follicle-like structure compared with 20 μg EE taken in a 21/7 regimen.
Studies with pregnancy as an outcome
A systematic review39 identified no direct evidence for risk of pregnancy associated with a HFI extended beyond 7 days.
The RCTs identified by a 2014 Cochrane Review27 were not powered to detect significant differences in pregnancy risk between continuous/extended and cyclical CHC regimens; only one reported a significantly lower risk of pregnancy with continuous compared to cyclical (vaginal) administration of COC (odds ratio (OR) 0.14, 95% confidence interval (95% CI) 0.02–0.97).43 One RCT published after the Cochrane Review (and designed to investigate continuation rather than effectiveness) reported similar pregnancy rates among 358 women randomised to either cyclical or continuous use of the same COC.44
Some observational studies suggest that risk of pregnancy associated with extended CHC regimens45 or CHC regimens with shortened HFI46 could be lower than that with traditional 21/7 regimens. A study47 examining pregnancy rates during an extended 91-day CHC regimen with 20 μg EE noted no reduction in contraceptive efficacy in women with obesity compared to women without obesity.
6.2.3 Safety of tailored CHC regimens
Available information regarding safety of extended compared to standard CHC regimens is reassuring. RCTs comparing extended and standard CHC regimens record very few serious adverse events associated with either type of regimen.27 Observational studies report similar (small) numbers of serious adverse events for extended regimens and for regimens with shortened HFI compared to 21/7 regimens.48,49
Direct data comparing risk of cardiovascular events and cancer between extended and standard CHC regimens are lacking. However, indirect evidence regarding cardiovascular risk is reassuring. In a Phase 3 trial of 20 μg EE/DRSP COC, 1067 women were randomised to standard cyclical, flexible extended or fixed extended pill-taking regimens for 1 year. A total of 755 women then entered an extension phase, taking the flexible extended regimen. Metabolic and haemostatic parameters, serum hormone levels and blood pressure were similar in all groups. Numbers of serious adverse events were very low in all groups.50 A smaller trial which randomised 78 women to use extended or standard cyclical regimens of 30 μg EE/DRSP COC found no statistically significant differences in carbohydrate or lipid profiles between the two groups over 6 months of use.51 In a third trial, 174 women were randomised to cyclical or continuous use of 20 μg EE/LNG COC (the dose of LNG was different in the two groups). The authors concluded that after 13 months of use, carbohydrate metabolism, lipid profile and haemostatic variables were broadly similar between the groups, but that further studies would be required to assess long-term continuous CHC.52 Haemostatic parameters were reported to be similar for 187 women randomised to extended or cyclical use of 30 μg EE/LNG COC for 6 months.53
Several studies have assessed the endometrium during continuous or extended CHC; endometrial thickening and histological abnormalities were not observed.27,50,54,55
6.2.4 Bleeding patterns with extended CHC regimens
A Cochrane Review of RCTs27 reported that in most studies bleeding patterns with extended CHC regimens were equivalent or improved compared to standard regimens.37,43,51,56–64 A systematic review28 that included both RCTs and observational studies concluded that overall, the total number of days of bleeding was lower with continuous or extended regimens than with cyclical use of CHC. Although there was an increase in breakthrough bleeding during the first months of use of continuous or extended regimens, its frequency and intensity subsequently decreased over time. Limited evidence suggests that bleeding patterns with continuous or extended use of the CTP and CVR show a similar reduction in bleeding/spotting days over time to that seen with extended use of COC.59,62,65–67
One study68 compared bleeding patterns in 139 existing cyclic COC users who were randomised to continuous use for 180 days of COC containing 30 μg EE/100 μg LNG, 20 μg EE/100 μg LNG, 30 μg EE/1000 μg NET or 20 μg EE/1000 μg NET; it should be noted that only the first of these is a COC preparation available in the UK. The study suggested more favourable bleeding patterns (more amenorrhoea and fewer spotting days) with continuous use of NET COC than with continuous use of LNG COC. The authors noted that the study findings did not support use of higher EE doses to prevent breakthrough bleeding during continuous COC use. It is not known how bleeding patterns with continuous use of other COC would compare.
6.2.5 Tailored CHC regimens and symptoms associated with the HFI
Symptoms such as headache, pelvic pain, bloating and breast tenderness are more frequent during the HFI than during the time that CHC hormones are being taken.69,70 Women may choose extended CHC regimens to avoid or reduce the frequency of symptoms associated with the HFI.
A Cochrane Review27 of RCTs identified studies that reported improvement in menstrual-related headache, bloating, tiredness and menstrual pain with extended COC regimens.
Observational studies similarly suggest benefit; a cohort study71 of 111 women who reported cyclical symptoms with two cycles of use of a 21/7 COC regimen found that mood, headache and pelvic pain scores improved significantly after the women switched to an extended COC regimen and were followed up for a year. Some 80% of the women continued the extended regimen for the full year, and 6 months after that most women reported that they had continued the extended regimen on their own. A prospective cohort study72 of 109 women given 30 μg EE/DRSP COC for two 21/7 cycles, followed by two 84/7 cycles (two-thirds completed all cycles) reported a significantly reduced incidence of heavy menstrual bleeding (HMB), intermenstrual bleeding, dysmenorrhoea, abdominal bloating, depressed mood and irritability at the end of the second 84/7 cycle compared to at enrolment.
6.2.6 Return to fertility after use of extended CHC regimens
One study73 found that of 187 women aged 18–49 years who had used continuous 20 μg EE/LNG COC for at least 6 months, 98.9% returned to spontaneous menstruation or became pregnant within 90 days. In another study, amongst 47 women who had used 20 μg EE/LNG COC continuously for 84 days, ovulation was observed within 37 days of stopping treatment in all but one case (98%).74
6.2.7 Acceptability of tailored CHC regimens
Evidence indicates that continuous or extended CHC regimens offer an acceptable alternative to standard CHC regimens for many women.
A UK trial56 randomised 503 women to use 30 μg EE/LNG COC either as a 21/7 regimen or as a regimen in which pills were taken consecutively until a 3-day bleed triggered a 3-day break in pill-taking. Of the 252 women using the tailored regimen, 179 women were followed up at 12 months; 54% were continuing the tailored regimen. This compared to 67% of women followed up in the 21/7 regimen arm of the study. Of note, there was no significant difference between standard and tailored regimens in terms of the proportion of women who continued taking any COC regimen at 12 months. The authors concluded that “tailored use can provide a suitable alternative to standard COC use for selected women” and that “offering the tailored regimen is unlikely to increase the risk of discontinuation of the COC”. Qualitative research carried out as part of this trial showed that some women using tailored COC regimens much preferred the reduced bleeding while others disliked the unpredictability of bleeding.56
A recent trial in Australia65 randomised 172 women to continuous use for a year of either a CVR or 20 μg EE/LNG COC. Women were instructed to take a 4-day break if they bled for four consecutive days. The study reported high satisfaction rates with continuous use of both methods; women liked the ease of use and infrequent bleeding, and for some women the absence of dysmenorrhoea, headaches and premenstrual symptoms were particular advantages. However, many women who were otherwise satisfied with the regimen disliked the unpredictability of bleeding.
A Cochrane Review27 identified six other RCTs that considered participant satisfaction with extended regimens; satisfaction was high and similar for both traditional and extended regimens.
A retrospective review75 of 318 women with unwanted hormone withdrawal symptoms on COC, who were counselled about using extended COC regimens, reported that of the 292 women followed up, 267 women chose to start an extended regimen and 172 continued to use the extended regimen at the time of their last follow-up. Various extended durations of pill-taking and shortened HFI were used.
As far back as 1977, a UK cohort study76 of 202 women started on a tricycling COC regimen reported that 82% of participants welcomed the reduction in bleed frequency. A total of 107 women completed 12 months of the tricycling regimen; of these 91% chose to continue the regimen after the trial had finished. Surveys of women in Holland,77 Germany,78 the USA79,80 and Italy81 found that more than half of the women of reproductive age would prefer to bleed less than once a month. In an Australian survey 54% of women preferred a monthly bleed.82
A Cochrane Review27 identified three RCTs in which study discontinuation rates were higher for extended or continuous regimens than for traditional 21/7 cycles; 10 RCTs reported no significant difference in discontinuation between regimens.
6.2.8 Offering tailored CHC regimens
In a UK study 112 women requesting COC (most already COC users) were given information about tailored COC regimens by a HCP using a structured script and patient advice sheet. The information was welcomed and understood by women and HCPs did not find the information-giving too time consuming.83
6.3 When can CHC be started?
Key information
D. CHC containing EE can be started by medically eligible women up to and including Day 5 of a natural menstrual cycle without the need for additional contraceptive protection.
D. CHC containing EE can be quick started by medically eligible women at any other time (with advice to use additional contraceptive precaution for 7 days) if:
It is reasonably certain that the woman is not pregnant
OR
A high sensitivity urine pregnancy test is negative (even if there is a risk of pregnancy from UPSI in the last 21 days). A follow up high sensitivity urine pregnancy test is required 21 days after the last UPSI.
Established FSRH guidance is that CHC containing EE can be started up to and including Day 5 of a natural menstrual cycle without the need for additional contraceptive precaution. After Day 5, CHC can be ‘quick started’ with advice to use additional contraceptive precautions (condoms or abstinence) during the first 7 days of CHC use (after seven consecutive days of CHC use, the evidence suggests that ovulation is inhibited).29 Follow-up pregnancy testing is required 21 days after the last UPSI. This advice is in line with current recommendations in the USA and from the World Health Organization (WHO).84,85 See FSRH Guideline Quick Starting Contraception.86
6.3.1 Starting CHC at the beginning of a natural menstrual cycle
Five studies are identified by a recent systematic review29 that consider the risk of ovulation (but not of pregnancy) if CHC is started at a time other than Day 1 of the menstrual cycle. Two small studies87,88 (n=14 and n=22) compared a group of women starting COC on Day 1 with a group starting on Day 5. No ovulations were observed, but ovarian suppression was greater if COC was started on Day 1. In two larger studies89,90 comparing commencement of COC on Day 1 and Day 7, ovarian activity was greater in the Day 7 group; risk of ovulation was significantly greater in the Day 7 group with a 20 μg EE, but not a 30 μg EE COC. However, markers used for occurrence of ovulation are not consistent across studies and frequency of ovulation may have been overestimated. A study91 of 40 women randomised to start COC on Day 1 or CVR on Day 5 observed no ovulations, but there was less ovarian suppression in the group who started CVR on Day 5.
In a study considering the effects of oral contraceptives administered at defined stages of ovarian follicular development, no ovulations were observed when COC was commenced at a follicle diameter of 10 mm (mean cycle Day 7.6).92 However 5/14 women ovulated when COC was initiated at 14 ± 1 mm (mean Day 11.7 ± 0.7; range Day 5–20) and 14/15 ovulated when COC was initiated at 18 ± 1 mm (mean Day 13.6 ± 0.8; range Day 7–20).
No studies are identified that consider ovarian activity when starting the CTP on different cycle days therefore advice is extrapolated from evidence for COC and CVR. Estradiol-containing COC should be started on Day 1 of a natural menstrual cycle. If started at any other time, additional contraceptive precautions are advised as per the manufacturer’s recommendations.
Women with short menstrual cycles
Fewer than 5% of women aged 15–44 years and fewer than 2% of women aged 20–39 years have menstrual cycles shorter than 20 days.93 Even smaller numbers (<1%) of women aged 14–42 years have cycle lengths shorter than 15 days.94 However, if there is concern about earlier ovulation associated with very short or variable cycles, women can be given the option to use additional contraceptive precautions when starting CHC after Day 1.
6.3.2 Quick starting CHC
Quick starting CHC, rather than waiting for the start of the next menstrual period, has the potential advantage of reducing the time during which a woman is at risk of pregnancy; it could also reduce barriers to commencing effective contraception that could result if a woman has to wait to start her contraceptive method.86 CHC can be quick started for medically eligible women in either of the following circumstances:
If pregnancy can be reasonably excluded (see Box 1) CHC can be quick started immediately.
If pregnancy cannot be reasonably excluded, a high-sensitivity urine pregnancy test (HSUPT) (able to detect human chorionic gonadotrophin (hCG) levels around 20 mIU/ml) should be taken; if negative, CHC can be quick started despite a risk of pregnancy from very recent UPSI. Almost all the available evidence suggests no adverse impact of fetal exposure to contraceptive hormones on pregnancy outcomes or risk of fetal abnormality. Refer to the FSRH Guideline Quick Starting Contraception for details of studies assessed. A further HSUPT should be taken 21 days after the last UPSI. Note that quick starting of CHC should be delayed for 5 days after ulipristal acetate (UPA) oral emergency contraception (EC).95
Criteria for reasonably excluding pregnancy
Healthcare practitioners can be reasonably certain that a woman is not currently pregnant if any one or more of the following criteria are met and there are no symptoms or signs of pregnancy:
She has not had intercourse since the start of her last normal (natural) menstrual period, since childbirth, abortion, miscarriage, ectopic pregnancy or uterine evacuation for gestational trophoblastic disease.
She has been correctly and consistently using a reliable method of contraception. (For the purposes of being reasonably certain that a woman is not currently pregnant, barrier methods of contraception can be considered reliable providing that they have been used consistently and correctly for every episode of intercourse.)
She is within the first 5 days of the onset of a normal (natural) menstrual period.
She is less than 21 days postpartum (non-breastfeeding women).*
She is fully breastfeeding, amenorrhoeic and less than 6 months postpartum.*
She is within the first 5 days after abortion, miscarriage, ectopic pregnancy or uterine evacuation for gestational trophoblastic disease.
She has not had intercourse for >21 days and has a negative high-sensitivity urine pregnancy test (able to detect human chorionic gonadotrophin (hCG) levels around 20 mIU/ml).
*See UKMEC 201696 and FSRH Guideline Contraception After Pregnancy97 for recommendations regarding use of combined normonal contraception after childbirth.
Bleeding patterns associated with quick starting CHC
A systematic review found that bleeding patterns were similar regardless of when in the cycle CHC was started.29
6.3.3 Summary of advice for starting CHC
Table 2 summarises when combined hormonal methods can be started and the requirements for additional contraceptive precaution. For further details on use of CHC after pregnancy (childbirth, abortion, miscarriage, ectopic pregnancy or gestational trophoblastic disease) see the FSRH Guideline Contraception After Pregnancy.97
Starting combined hormonal contraception and requirement for additional contraceptive precautions
6.3.4 Switching to CHC from other contraceptive methods
FSRH guidance98 on switching from hormonal contraception and non-hormonal contraception to CHC is summarised in Table 3a and Table 3b, respectively. See FSRH Guidance Switching or Starting Methods of Contraception.98
Switching from hormonal contraceptive method to combined hormonal contraception98
Switching from non-hormonal contraceptive method to combined hormonal contraception98
7. How effective is CHC?
7.1 Contraceptive effectiveness of CHC
Key information
C. Contraceptive effectiveness of all CHC is similar.
✓ If used perfectly, CHC is very effective for contraception. With typical use, CHC is less effective for contraception than long-acting reversible contraception (LARC).
Clinical recommendation
✓ Women requesting CHC should be informed about the effectiveness (with both typical and perfect use) of CHC and other contraceptive methods, including the superior effectiveness of LARC.
All CHC methods require consistent and correct use to provide effective contraception. Method adherence can vary widely depending on user characteristics such as age, socioeconomic status, desire to prevent or delay pregnancy, and culture. A Cochrane Review comparing standard use of the combined pill, patch and ring concluded that these methods are of similar effectiveness.99 See Section 6.2.2.
With perfect use of CHC (following directions for use) it has been estimated that 0.3% of users experience an unplanned pregnancy during the first year of use. In contrast, the first-year failure rate associated with typical use of CHC (actual use including inconsistent or incorrect use) has been estimated to be around 9%.100 This estimate uses data from the US National Survey of Family Growth.101–103 Reported CHC contraceptive failure rates vary. It is noted that women who know that they are taking part in a study might comply differently with pill-taking. The Contraceptive Choice project in the USA reported a first-year failure rate for combined pill, patch and ring of 4.8% among women who were provided with their choice of contraceptive method free of charge.104 The International Active Surveillance of Women Taking Oral Contraceptives study in the USA reported a 1-year failure rate of 3.5%, based on 1634 unintended pregnancies during 73 269 woman-years of oral contraceptive pill exposure.105 Secondary analysis of data from the European Active Surveillance (EURAS) study of OC (which included (112 659 woman-years of OC exposure and 545 unplanned pregnancies) reported a 0.75% failure rate (95% CI 0.68–0.82) for OC in the first year of use.106
Table 4 compares the effectiveness of currently available contraceptive methods, with the most effective LARC methods highlighted. Given the relatively high estimated failure rates associated with typical use of CHC, the GDG recommends that women requesting CHC should be informed about the effectiveness of different contraceptives, including LARC.107 The failure rate of LARC is less than 1% with both typical and perfect use as it is not subject to user failure.
Percentage of women experiencing an unintended pregnancy within the first year of use with typical use and perfect use (modified from Trussell)100
Acceptability of LARC methods for women who initially request short-acting contraception
Some women who request OC can find LARC methods an acceptable alternative; in a US study, 916 women aged 18–29 years who requested short-acting contraception were given the option of receiving their short-acting method in the usual way or being randomised to receive either a short-acting method or a LARC method of their choice free of charge. A total of 392 women agreed to randomisation. Amongst women randomised to LARC, method acceptability and continuation rates were high and unintended pregnancy rates significantly lower than for women choosing or randomised to short-acting methods.108 LARC methods should be discussed, but women should not be pressured into using any particular method of contraception.
7.2 What can affect contraceptive effectiveness of CHC?
As noted in Section 7.1, effectiveness of CHC is highly dependent on correct and consistent use. Other factors that could affect contraceptive effectiveness are considered below.
7.2.1 Is contraceptive effectiveness of CHC affected by obesity/weight?
Key information
C. Most evidence suggests no association between weight/BMI and effectiveness of COC.
D. Limited evidence suggests a possible reduction in patch effectiveness in women ≥90 kg.
Note that use of CHC is UKMEC 3 for use by women with BMI ≥35 kg/m2. UKMEC recommendations relate to safety of use rather than to effectiveness.
Evidence relating to the effect of body weight/BMI on effectiveness of CHC is limited to observational studies in which height, weight and pregnancy are often self-reported and potential confounding factors such as contraceptive compliance and frequency of intercourse are unknown. Most studies include relatively few women in the highest weight/BMI categories. There is limited evidence that ovarian activity in the HFI could be more pronounced in obese women.41,42 See Section 6.2.2 regarding studies considering ovarian activity in the HFI as an indication of risk of pregnancy.
A 2017 systematic review109 reported that 10 out of 14 studies of COC identified did not report a difference in effectiveness by body weight or BMI; in the remaining four studies, the magnitude of the reported difference in COC failure was very small. Differences between different COC formulations could not be distinguished. A 2016 Cochrane Review110 concluded that in general the evidence identified did not indicate an association between increasing body weight or BMI and effectiveness of COC.
The limited evidence identified109 suggests that increasing body weight and BMI may contribute to decreasing effectiveness of the CTP. No direct evidence regarding body weight/BMI and effectiveness of the contraceptive ring was identified.
The GDG (in line with the Summary of Product Characteristics for the CTP)10 notes that contraceptive effectiveness of the CTP could be decreased in women weighing ≥90 kg, therefore it is recommended that additional precautions or an alternative method should be advised for women ≥90 kg.
7.2.2 Is contraceptive effectiveness of CHC affected by bariatric surgery?
Clinical recommendation
D. Women who have had bariatric surgery should be advised that the effectiveness of COC could be reduced.
There are theoretical concerns that both malabsorptive and restrictive bariatric procedures could decrease the absorption of oral contraceptives.111,112 A systematic review113 identified one small prospective cohort study114 in which two of nine women using COC after biliopancreatic bypass surgery (both with significant diarrhoea) became pregnant in the 2 years following surgery; a second descriptive study115 reported no pregnancies among COC users (number unknown) in the 2 years after a gastric banding procedure.
One pharmacokinetic study116 reported lower serum progestogen levels after administration of oral progestogen for morbidly obese women (BMI ≥40 kg/m2) after bypass surgery compared with healthy non-obese women; the difference could however be attributable to body weight. In contrast, a second pharmacokinetic study117 reported higher serum progestogen levels after administration of an oral combined estradiol/progestogen preparation in 12 morbidly obese women after bypass surgery than in six morbidly obese women who had not had surgery.
The evidence is too limited to make a definite recommendation regarding the effectiveness of COC after bariatric surgery. The GDG recommends that women who have had bariatric surgery should be advised of potential reduced effectiveness of COC and should consider a non-oral method of contraception.
7.2.3 What drug interactions are important to consider in relation to CHC?
Serum levels of contraceptive hormones may be altered by concomitant use of other drugs; contraceptive effectiveness could be affected. Hormonal contraceptives may themselves alter serum levels of other drugs that a woman is taking, with potential adverse effects. Drug interactions should therefore always be considered when prescribing CHC and when prescribing other drugs for women who are using CHC.
Refer to the FSRH Guideline Drug Interactions with Hormonal Contraception.118
Enzyme-inducing drugs
Clinical recommendations
D. Women using enzyme-inducing drugs should be informed that the contraceptive effectiveness of CHC could be reduced during use of the enzyme-inducer and for 28 days after stopping.
D. Women using enzyme-inducing drugs should be offered a reliable contraceptive method that is unaffected by enzyme-inducers.
FSRH Guideline Drug Interactions with Hormonal Contraception118 notes that hepatic enzyme-inducing drugs increase the metabolism of estrogens and progestogens, which could reduce the contraceptive effectiveness of all CHC methods. Women using enzyme-inducing drugs should be advised to switch to a contraceptive method (e.g. intrauterine methods or the progestogen-only injectable) that is unaffected by enzyme-inducers.
It is established practice that if, after advice to switch contraceptive method, a woman wishes to use COC concomitantly with an enzyme-inducing drug (with the exception of rifampicin or rifabutin which are potent enzyme-inducers) use of a minimum 50 µg (30 µg + 20 µg) EE monophasic combined pill may be considered during use of the enzyme-inducer and for a further 28 days after stopping. A continuous or tricycling regimen plus a shortened pill-free interval of 4 days should be used. Breakthrough bleeding could indicate low serum EE concentrations. Dose of EE can exceptionally be increased up to a maximum of 70 µg after specialist advice. It is not known how such usage affects risk of VTE. The use of two patches or two rings is not recommended.
Short-term use of enzyme-inducing drugs (<2 months) can be managed more flexibly than longer-term use. Continuing use of CHC with consistent and careful use of condoms may be appropriate in this situation.
Lamotrigine
Clinical recommendation
D. Women taking lamotrigine should be advised that CHC may interact with lamotrigine; this could result in reduced seizure control or lamotrigine toxicity. The risks of using CHC could outweigh the benefits.
Serum levels of lamotrigine can be reduced by CHC.119–124 A case series122 reported increased seizure frequency in four women with reduced lamotrigine levels following the initiation of COC. Data120 demonstrate increased lamotrigine levels during the HFI and increased lamotrigine side effects have been reported on cessation of CHC.119
Lamotrigine is not thought to be an enzyme-inducing drug, but the manufacturer advises that contraceptive effectiveness of CHC could be reduced by concurrent use of lamotrigine. This advice is based on a study125 of 16 women using 30 µg EE/150 µg LNG and lamotrigine for 6 weeks which found a modest increase in levonorgestrel clearance and changes in serum FSH and LH. The clinical significance in terms of contraceptive effectiveness is unknown. An earlier study of women using 30 µg EE/150 µg LNG and lamotrigine for 10–14 days reported a statistically non-significant decrease in the mean plasma concentration of EE but no change in LNG levels; no ovulation occurred and no change in menstrual patterns was observed.126
The risk of using CHC may outweigh the benefit for women using lamotrigine, given the potential risk of reduced seizure control whilst taking CHC, and potential for lamotrigine toxicity in the HFI. It is advised that alternative contraception should be considered.118
Antibiotics (non enzyme-inducing)
Key information
D. Additional contraceptive precautions are not required when antibiotics that do not induce enzymes are used in conjunction with CHCs.
Most broad-spectrum antibiotics are non-enzyme-inducing and it is established FSRH guidance118 that no additional contraceptive precaution is required unless the antibiotics (and/or illness) cause vomiting or severe diarrhoea (see Section 7.2.4).127,128
Progestogen receptor modulators
Clinical recommendation
D. Women should be advised to wait 5 days after taking UPA-EC before starting CHC. Women should be made aware that they must use condoms reliably or abstain from sex during the 5 days waiting and then until their contraceptive method is effective.
UPA is a selective progesterone receptor modulator. Limited evidence from biomedical studies129,130 suggests that effectiveness of oral hormonal contraception is not reduced by concomitant use of UPA-EC. Biomedical studies have demonstrated that starting an EE/LNG COC131 or a desogestrel POP129 soon after UPA 30 mg given for emergency contraception (UPA-EC) reduces the ability of UPA-EC to delay ovulation and could therefore reduce the effectiveness of UPA-EC. The FSRH Guideline Emergency Contraception recommends that after UPA-EC, commencement of CHC is delayed for 5 days (at least 120 hours) after UPA-EC has been given.95 This ensures that the UPA-EC is as effective as possible in preventing pregnancy resulting from the episode(s) of UPSI for which it was taken. After the 5 days waiting, CHC can be started with advice to use additional contraceptive precautions for the following 7 days.
Theoretically, there could be an interaction between CHC and UPA taken for management of fibroids.
7.2.4 Severe diarrhoea or vomiting
Clinical recommendation
D. Women using COC should be advised that contraceptive effectiveness could be reduced by vomiting or severe diarrhoea.
The general advice for women using oral contraceptives is to follow the instructions for missed pills if vomiting occurs within 3 hours of taking COC or severe diarrhoea occurs for >24 hours. Women should be advised to consider non-OC if diarrhoea or vomiting persist.118 Some drugs have the potential to reduce the effectiveness of contraceptives indirectly by causing diarrhoea or severe vomiting.
8. Incorrect use of CHC
Missing CHC removes the suppressive effects of contraceptive steroids on ovarian follicle growth thereby risking ovulation and conception. Women using CHC who miss pills or make mistakes with their CVR or CTP are at increased risk of pregnancy compared with women who use CHC perfectly.
Repeated attempts to re-write ‘missed pill rules’ which more accurately reflect the evidence have concluded that simple rules are more likely to be followed. As a result, advice on what to do when pills (or other methods of CHC) are taken incorrectly is overcautious. Nevertheless a simple, overcautious rule to which everyone agrees is better than complicated rules that are not followed. See FSRH Guidance on Incorrect Use of CHC.
8.1 Combined oral contraception
A COC pill is missed if it is not taken in the 24 hours after it should have been taken. Missing a single COC pill is insufficient to reverse ovarian suppression; however, missing several pills or extending the HFI by missing pills at the end of a packet or forgetting to restart the new packet on time could theoretically increase risk of ovulation.
Many observational studies have attributed pregnancy during COC use to missed pills, but even when daily diaries of pill-taking are kept during studies, information on dosing errors is likely to be inaccurate.132 One study of typical COC use in which 82 new users of a standard 21/7 COC were given their pill supply in an electronic dispenser which recorded whether or not pills had been taken from the packet showed that during 3 months of COC use 57% of women missed an average of three or more pills each cycle but there were no pregnancies.132 Evidence from biomedical studies that have assessed ovarian activity associated with missed pills is limited by the fact that studies are small and use different markers to define ovulation.
Missed pills in weeks adjacent to the HFI
The available evidence for risk of ovulation if the HFI is extended is presented in Section 6.2.2. It is considered that missing pills in the first week of pill taking after the HFI or in the week prior to the HFI effectively extends the HFI; missed pill rules reflect this.
Missed pills in weeks not adjacent to the HFI
Two small studies that examined ovulation risk if pills are missed in weeks not adjacent to the HFI indicated that ovarian activity is suppressed after seven consecutive days of COC.29 A systematic review39 concluded (on the basis of 10 small, biomedical studies) that missing one to four consecutive pills on days not adjacent to the HFI resulted in little follicular activity and low risk of ovulation. The review identified two studies comparing missed pills containing either 20 or 30 μg EE which reported more follicular activity when 20 μg EE pills were missed; differences in ovulation rates did not vary with the progestogen component of COC.
No studies have explored the effect of missed pills among women using COC containing natural estrogens. Providers should refer women who use these brands to the advice given on the label.
See FSRH Guidance on Incorrect Use of CHC.
8.2 Combined transdermal patch
A systematic review39 included two studies that examined the CTP: a pharmacokinetic study found that serum concentrations of EE and norelgestromin remained within the reference range for contraceptive efficacy even after extending patch use for 3 days;133 in the second study, little follicular activity and low risk of ovulation were observed when use of a patch was extended to 10 days or a patch was removed after 7 days of use and not replaced for 3 days thereafter.134 No studies were found on extending the patch-free interval.
See FSRH Guidance on Incorrect Use of CHC.
8.3 Combined vaginal ring
A systematic review39 included six studies examining dosing errors with the CVR: three observational studies135–137 provided limited evidence suggesting that extension of the ring-free interval for up to an additional 48 hours does not increase the risk of pregnancy; one study138 reported that after a deliberately extended HFI which was continued until a 13 mm ovarian follicle developed, ovarian function and further follicular growth was re-suppressed when a new ring was inserted; in another study inhibition of ovulation was maintained after deliberately leaving the ring in place for up to 5 weeks, suggesting that the suppressive effects of the CVR last a considerable time.
See FSRH Guidance on Incorrect Use of CHC.
Women who frequently miss COCs or make repeated mistakes with a CTP or CVR should be advised to consider an alternative contraceptive method that is less dependent on the user to be effective (e.g. LARC methods).
9. Non-contraceptive health benefits associated with CHC use
Key information
✓ Use of CHC for contraception may also be associated with non-contraceptive health benefits
B. Use of CHC can reduce heavy menstrual bleeding (HMB) and menstrual pain and improve acne.
C. Use of CHC may be beneficial for women with premenstrual syndrome (PMS) symptoms.
A. Use of CHC (particularly continuous CHC regimens) can reduce risk of recurrence of endometriosis after surgical management.
B. CHC can be used for management of acne, hirsutism and menstrual irregularities associated with polycystic ovary syndrome (PCOS).
C. CHC use is associated with a significant reduction in risk of endometrial and ovarian cancer that increases with duration of CHC use and persists for many years after stopping CHC.
C. Use of CHC is associated with a reduced risk of colorectal cancer.
9.1 Heavy menstrual bleeding
The National Institute for Health and Care Excellence (NICE) Heavy Menstrual Bleeding guideline indicates that COC can be used for management of HMB but would generally be second-line after the LNG-releasing intrauterine system (IUS).139 Evidence from RCTs and non-randomised trials consistently reports a reduction in menstrual blood loss in women with HMB using CHC.140–143
Further evidence from two RCTs142,143 that compared CVR with COC for the management of HMB suggests that they are equally effective, and that CVR could offer better cycle control and adherence to correct use.
9.2 Menstrual pain
Limited evidence identified in two systematic reviews144,145 suggests that COC reduces menstrual pain. There is no robust evidence for a differential benefit between different preparations of COC including different estrogen dose. One RCT146 reported that CVR is effective in treatment of idiopathic chronic pelvic pain. A small number of RCTs147–149 suggest that extended use of COC is effective for the treatment for primary dysmenorrhoea and may be superior to the traditional cyclic regimen, at least in the short term.
9.3 Acne
Evidence suggests that use of CHC can improve acne vulgaris. A Cochrane Review150 updated in 2012 concluded that COCs are effective in reducing facial acne lesions. The review included nine placebo-controlled trials, all demonstrating that COC reduced acne lesion counts, severity grades and self-assessed acne compared to placebo. Data were limited for comparative effectiveness of different COC; overall few differences between the COCs studied were identified in terms of their effectiveness in treating acne. The authors noted that the lack of use of standardised methods for assessing acne prevents the pooling of results across trials and complicates their interpretation. Two further RCTs151,152 also reported improvement in acne outcomes with COC use.
Two small observational studies have reported that acne improved for some women during CTP use.153,154 A Cochrane Review99 which included three RCTs found that acne was reported as a side effect less often by CVR users than by COC users.
9.4 Premenstrual symptoms
Based on the limited available evidence (presented below) the GDG recommends that symptoms of premenstrual syndrome (PMS)/premenstrual dysphoric disorder (PMDD) could be improved in women who use COC for contraception. A continuous regimen may be considered. The 2016 Royal College of Obstetricians and Gynaecologists (RCOG) Green-top Guideline Management of Premenstrual Syndrome155 recommends that EE/DRSP COC should be considered a first-line pharmaceutical intervention for management of PMS.
9.4.1 EE/DRSP COC for management of premenstrual symptoms
Addressing EE/DRSP COC specifically, a 2012 Cochrane Review of RCTs156 concluded “Drospirenone with EE 20 µg COC may help treat premenstrual symptoms in women with premenstrual dysphoric disorder (PMDD). However, a powerful placebo effect was evident: in one trial, symptoms were reduced for 48% of the drospirenone COC group versus 36% of the placebo group. The difference may not be clinically significant. Furthermore, effectiveness after three cycles is unknown. Little evidence exists for treating less severe symptoms or whether a drospirenone COC works any better than other COCs.”
Subsequent to the Cochrane Review a small RCT demonstrated no significant difference between placebo and EE/DRSP COC taken either cyclically or continuously for management of PMDD.157 The authors commented on the marked placebo response that was observed; a second small RCT suggested that COC containing either DRSP or desogestrel could reduce PMS symptoms, but there was no placebo arm.158
9.4.2 Other COC for management of premenstrual symptoms
Evidence from RCTs for CHC other than EE/DRSP is sparse and inconclusive, but suggests that other COC formulations could also be associated with symptom improvement in women with PMDD.159,160 The findings of the observational studies identified161–166 are limited by small study size, short duration of observation, lack of a verified symptom assessment tool, and lack of a comparator group that was not using hormonal contraception.
9.4.3 Extended COC regimens for management of premenstrual symptoms
A cohort study (and its extension) commenced 114 women on an EE/DRSP COC for two 21/7 cycles and then changed them to a continuous regimen of the same COC.71,162 102 women completed 168 days and 80 completed a year of extended use. The study reported that PMS symptoms improved significantly with the extended regimen compared to cyclical use.
9.5 Vasomotor symptoms
Overall, limited evidence suggests that use of COC can help alleviate vasomotor symptoms in perimenopausal women.
A placebo-controlled, double-blind, randomised, parallel group study167 including 132 perimenopausal women found that the frequency and severity of hot flushes decreased in the group treated with a low-dose, monophasic COC (20 µg EE/norethisterone) compared to placebo. Among the 65% of subjects who experienced at least one hot flush daily (38 COC, 36 placebo), COC users experienced approximately 50% fewer hot flushes over the 6-month study period than placebo users. However, statistical significance was not reached due to wide variability. Quality of life assessments indicated significant improvements in the COC treatment group.
A randomised, double-blinded study168 of 56 women in their 40s presenting with mood disorders and/or hot flushes reported that the addition of 5 days of estrogen during the HFI improved the vasomotor symptoms of perimenopausal women using COC. Thirty-three women were randomised to the estrogen group (21 tablets containing 20 µg EE/desogestrel, followed by two placebo tablets and five tablets containing 10 µg EE) and 23 women to the placebo group (21 tablets containing 20 µg EE/desogestrel and then seven placebo tablets). During 3 months of use, women in the estrogen group reported a significant decrease in vasomotor symptoms (p<0.04) compared to the placebo group.
A 3-year, prospective cohort study169 comparing 100 perimenopausal women treated with a triphasic COC (30/40/30 µg EE and 0.05/0.075/0.125 mg LNG) with a similar number of age-matched untreated women reported that all women in the treatment group had complete relief of vasomotor symptoms after 3 months’ use; 90% achieved this within 2 months. In contrast, 60% of women in the untreated group had no improvement in vasomotor symptoms during the 3-month observation period.
Clearly there is a great deal more evidence for use of hormone replacement therapy (HRT) for vasomotor symptoms170. Decisions about whether it is more appropriate for a woman aged under 50 to use HRT plus additional contraception or CHC alone must be made on an individual basis, taking into consideration the safety of use of HRT compared to that of CHC.
9.6 Bone health
A Cochrane Review of RCTs171 concluded that COC use does not appear to negatively affect BMD. A Cochrane Review of observational studies172 reported that the evidence identified does not indicate an overall association between oral contraceptive use and fracture risk.
Adolescents
Some studies have suggested that in adolescents, accrual of BMD could be lower in users of COC than in non-users of hormonal contraception.173–175 One study174 which randomised 487 girls aged 12–19 years to use of a 30 μg EE/LNG COC either as a traditional 21/7 regimen or as an extended 84/7 regimen compared lumbar spine BMD after 12 months of use to an unmatched reference group of non-users of hormonal contraception. Increase in BMD was significantly greater among non-users than for those using 21/7 COC, but not for users of the extended regimen 84/7 COC.
Perimenopausal women
Note that use of CHC by women aged over 50 years is not generally recommended (see Section 15.1.1). Evidence suggests that COC could be beneficial in preventing the decline in BMD in perimenopausal women. Five prospective cohort studies169,176–179 (four studies from the same authors) compared perimenopausal women given various low-dose COC for 2 or 3 years (n=16 to n=100) with non-COC-using controls; the studies reported no change or increase in BMD amongst COC users and reduced BMD in the control groups. A very small RCT180 which compared eight perimenopausal women given low-dose COC with nine matched controls over 3 years reported a slight, non-significant increase in BMD in COC users and a significant reduction in BMD in controls. Evidence from a large RCT181 investigating use by perimenopausal women of EE/NET preparations containing much lower doses of EE (1–10 μg) than those in COC also suggests a protective effect of EE/progestogen on BMD in the perimenopause.
The clinical significance of these findings in terms of fracture risk is uncertain.
9.7 Endometriosis
NICE Guidance Endometriosis: Diagnosis and Management182 and European Society of Human Reproduction and Embryology (ESHRE) Guideline Management of Women with Endometriosis183 indicate that CHC has an important role in the management of endometriosis.
Studies have shown that CHC therapy is effective, safe and well-tolerated by women with endometriosis.182,184 A meta-analysis185 reported a significantly higher rate of remission from endometriosis symptoms and a lower rate of recurrence in women taking COC after surgery compared with surgery alone.
Evidence suggests that a continuous rather than a cyclical COC regimen is advantageous in the management of endometriosis. One systematic review186 showed that after conservative surgery, continuous COC use was associated with a significant reduction in dysmenorrhoea and a longer period before dysmenorrhoea recurred compared with cyclical use. One further RCT187 also reported a reduction in endometriosis-associated pelvic pain, an improvement in sexual activity and quality of life in women on a EE/dienogest continuous regimen compared to a 21/7 regimen. Another systematic review188 reported that a significantly lower postoperative dysmenorrhoea recurrence rate was observed in continuous compared to cyclical COC users; however, this study did not identify significant differences in dyspareunia, non-menstrual pelvic pain, or endometriosis recurrence rates between continuous and cyclical users.
Women with endometriosis who wish to use OC may also be advised about progestogen-only contraception, which is an effective first-line alternative for management of endometriosis symptoms and reduction of recurrence risk, but avoids any estrogen-associated health risks.184,189,190
9.8 Polycystic ovary syndrome
The Endocrine Society Clinical Practical Guideline Diagnosis and Treatment of Polycystic Ovary Syndrome191 recommends CHC (including the CTP and CVR) for first-line treatment of menstrual irregularity, acne and hirsutism in women with PCOS. The guideline notes however that “there are insufficient data to define the optimal duration of treatment”
The Endocrine Society also recommends CHC as the first-line treatment for adolescents requiring treatment for acne, hirsutism or menstrual bleeding irregularities due to anovulation and for pre-menarchal girls with clinical and biochemical evidence of hyperandrogenism in the presence of advanced pubertal development (i.e. Tanner Stage IV breast development).191
With regard to management of acne and hirsutism, there is no good evidence for any differential effectiveness of CHC containing different progestogens. Recent studies have focused on the effects of COC containing DRSP, an anti-androgenic progestogen. A systematic review192 which included 18 RCTs of EE/DRSP versus standard treatment options concluded that DRSP was effective in treating the symptoms of PCOS. Recent evidence suggests benefit with use of 20 μg EE/DRSP COC.193,194
9.9 Effect of CHC use on cancer risk and mortality
A large number of epidemiological studies (and systematic reviews and meta-analysis of these studies) have informed our understanding of the association between use of COC and risk of cancer. Long-term follow-up in the Royal College of General Practitioners (RCGP) Oral Contraception Study195 indicates a statistically non-significant 4% reduced risk of any cancer (incidence rate ratio (IRR) 0.96; 99% CI 0.9–1.03) associated with ever-use of OC compared with never-use.
9.9.1 Endometrial cancer
Systematic review and meta-analyses of observational studies196,197 indicate that OC use is associated with a reduced risk of endometrial cancer that correlates with duration of use and persists for many years after cessation. A recent meta-analysis197 of 36 international epidemiological studies found that every 5 years of OC use is associated with a relative risk of 0.76, resulting in a 50% reduction in risk of endometrial cancer with 10–15 years of use. A meta-analysis reported a persistent protective effect for as long as 30 years after cessation of OC; no significant differences were observed when comparing OC doses and formulations.197
In line with this, the RCGP Oral Contraception Study195 reported that compared to never-users of OC, the risk of endometrial cancer for ever-OC-users is reduced by 34% (IRR 0.66; 99% CI 0.48–0.89). Similarly, recently published data from a large US prospective cohort study198 indicate a significant 34% reduction in risk of endometrial cancer associated with ≥10 years OC use compared to never-use or use for less than a year; the greatest risk reduction was observed amongst smokers and women with obesity.
9.9.2 Ovarian cancer
A systematic review of observational studies199 reported a reduction in risk of ovarian cancer in ever-users of OC compared to never-users. The meta-analysis199 found that the protective effect is duration-dependent, with women who have used OC for at least 10 years having a 50% reduction in incidence of ovarian cancer. A review of published meta-analyses200 reported that the protective effect has been observed in women both with and without a genetic predisposition to ovarian cancer, increases with increasing duration of OC use and persists for at least 30 years after cessation of use. A subsequently published case-control study201 which included 1632 cases and 2340 controls suggested that there could be greater protection conferred to those who start OC before the age of 35 years than those who start after age 35 years. The UK RCGP Oral Contraception Study195 reported that, compared to never-users of OC, the risk of ovarian cancer of ever-OC-users is reduced by 33% (IRR 0.67; 99% CI 0.5–0.89). Recently published data from a large US prospective cohort study198 indicate a significant 40% reduction in risk of ovarian cancer associated with ≥10 years of OC use compared to never-use or use for less than 1 year.
BRCA gene mutation carriers
On the basis of evidence from case-control studies that include small numbers of cases, three systematic reviews with meta-analysis202–204 have concluded that amongst BRCA carriers, use of OC (COC or POP not specified, but majority likely to be COC) is associated with reduced risk of ovarian cancer with use, proportional to the duration of use. The evidence is stronger for BRCA1 carriers but exists for both BRCA1 and BRCA2. See Section 10.4.
9.9.3 Colorectal cancer
Evidence from three meta-analyses196,205,206 of data from observational studies suggests that ever-OC-users have a reduced risk of colorectal cancer compared to never-OC-users. In line with the findings of the other two studies, the most recent meta-analysis205 which included 12 cohort studies and 17 case-control studies with a total of 15 790 cases of colorectal cancer reported a summary relative risk (RR) for colorectal cancer of 0.82 (95% CI 0.76–0.88) for ever-users versus never-users of OC after adjustment for confounding lifestyle factors. More recently published data198 from a large prospective cohort study suggested no significant association between OC use and risk of colorectal cancer. The UK RCGP Oral Contraception Study195 reported that compared to never-users of OC, the risk of colorectal cancer of ever-users is reduced by 19% (IRR 0.81; 99% CI 0.66–0.99).
9.9.4 Mortality
A meta-analysis207 of eight cohort studies involving 217 868 women and 40 570 deaths did not find a significant association between ever-use of OC and all-cause mortality (hazard ratio (HR) 0.94; 95% CI 0.87–1.02) regardless of duration of OC use and time since last use. The UK RCGP Oral Contraception Study, a large prospective UK cohort study with 1.3 million woman-years of observation, found that women who had ever used OC had a 12% lower risk of all-cause mortality when compared with those who had never used OC.208 In addition to reduced mortality, ever-users of OC were observed to have a non-significant reduction in overall cancer risk, and for some cancers this protective effect persisted for decades following cessation of OC.195 Reassuringly, over a 44-year period of follow-up, no increased cancer risk was observed later in life for women who had ever used OC.
10. Health risks associated with CHC use
Clinical recommendation
✓ Women should be informed about the health risks associated with use of CHC.
10.1 Venous thromboembolism (VTE) (including deep vein thrombosis and pulmonary embolism)
Key information
C. Current use of CHC is associated with increased risk of VTE; some CHC formulations are associated with a greater risk of VTE than others, dependent on progestogen type and estrogen dose.
Clinical recommendation
C. Women should be advised that use of CHC is associated with an increased risk of VTE, but the absolute risk of VTE for an individual CHC user remains very small.
Evidence from observational studies suggests that current use of COC is associated with a 3- to 3.5-fold increase in VTE risk compared with non-use of CHC.209–211 It is important to note that despite this increased risk, the number of VTE events in women using CHC remains very small; the absolute risk of VTE during use of CHC is estimated by the European Medicines Agency to be between 5 and 12 per 10 000 women per year of use compared to 2 per 10 000 non-CHC users per year.212 Of the small number of VTE events that do occur during use of CHC, approximately 1% are fatal.213
VTE risk is lower during CHC use than during pregnancy and the postpartum period.214–221 By reducing rates of unplanned pregnancy, CHC use lowers the overall rate of VTE in the population in comparison to populations without access to effective contraception.222
Risk of VTE is highest in the months immediately after initiation of CHC223–226 or when restarting after a break of at least 1 month.223 The risk then reduces over the first year of use and remains stable thereafter.224,226–229 Frequent stopping and starting of CHC is therefore discouraged.
UKMEC 2016 gives recommendations regarding safety of use of CHC by women with characteristics or medical conditions (such as increasing age, higher BMI and thrombophilia) that put them at increased risk of VTE.96
10.1.1 Effect of progestogen type on VTE risk
A systematic review identified no relevant RCTs.230 Meta-analysis230 of the data from observational studies (which may be subject to confounding and prescribing bias) indicated that use of low-dose COC (<50 μg EE) containing cyproterone acetate, desogestrel, gestodene or DRSP was associated with a significant 1.5- to 2-fold risk of VTE compared to use of COC containing LNG. Norgestimate COC was found to be associated with similar VTE risk to LNG COC. These findings are consistent with those of other recent meta-analyses which suggest that use of some third-generation COC is associated with greater VTE risk than use of second-generation COC (differences are not always statistically significant).209,210,231,232
In 2014, the EMA published estimated figures for absolute risk of VTE in users of CHC (see Table 5).
European Medicines Agency estimated risk of developing a venous thromboembolism (VTE) in a year according to type of combined hormonal contraception (CHC) used212
Note that estimates of background VTE risk in women of reproductive age vary. The EMA estimates that the incidence of VTE among women who are not using CHC and are not pregnant is about 2 per 10 000 woman-years233; a large Danish cohort study234 reported a VTE incidence of 3.7 per 10 000 woman-years for non-users of CHC; a 2007 literature review235 concluded that the overall VTE incidence in all women of reproductive age is likely to be in the range of 5–10 per 10 000 woman-years.
10.1.2 Effect of dose of EE on VTE risk
Available studies are limited by their observational nature and the small numbers of VTE events in some study groups. COC preparations that have been studied vary with respect to progestogen as well as the dose of EE; it is therefore difficult to compare the effect of EE dose on VTE risk.
A systematic review and meta-analysis suggested that VTE risk among users of COC is dependent on the dose of EE, with higher EE dose being associated with greater VTE risk.209,236 The meta-analysis209 concluded that a 50 μg EE/LNG COC was associated with RR for VTE of 2.1 (95% CI 1.4–3.2) and 2.3 (95% CI 1.3–4.2) compared with a 30 μg and 20 μg EE/LNG COC, respectively. VTE risk was significantly greater for 30 μg EE than 20 μg EE COC containing gestodene, but not those containing LNG or desogestrel.
Subsequent to the systematic review, a large French database study indicated a lower risk of pulmonary embolism associated with COC containing 20 μg EE than COC with 30–40 μg EE (adjusted RR 0.75; 95% CI 0.67–0.85).237
10.1.3 Effect of estrogen type on VTE risk
Most COC contain EE. However, COC are now available that have estradiol as their estrogen component, in combination with either dienogest or nomegestrol acetate. Direct evidence regarding risk of VTE associated with use of these COC is limited. A large cohort study in the USA and Europe which observed 47 VTE events amongst 50 203 new COC users followed for a mean of 2.1 years reported adjusted HRs of 0.4 (95% CI 0.2–1.0) and 0.5 (95% CI 0.2–1.5) for users of estradiol valerate/dienogest compared to users of “other COC” and EE/LNG COC, respectively.238 Studies that have compared the effect of estradiol COC on haemostatic variables to that of EE/LNG COC suggest that use of estradiol-containing COC (particularly estradiol/nomegestrol acetate) is associated with a haemostatic profile similar to or more favourable than that with EE/LNG COC. The potential impact of this on VTE risk remains to be clarified.5,239–243
10.1.4 Effect of route of administration on VTE risk
Data for VTE risk associated with the EE/norelgestromin CTP and EE/etonogestrel CVR are limited and conflicting.
Combined transdermal patch
A systematic review244 identified conflicting evidence from seven observational studies that compared the VTE risk associated with use of the CTP to that with use of COC containing LNG or norgestimate. One retrospective cohort study245 and one case-control study246 reported significant, 2-fold greater VTE risk among CTP users compared to COC users. One cohort study247 considered only risk of cerebral venous thrombosis and recorded very few events (two in COC users and none in CTP users). Of the remaining four case-control studies, one248 reported a non-significantly increased VTE risk for CTP users compared to COC users (OR 2.0; 95% CI 0.9–4.1) and three248–250 did not find significant differences.
Combined vaginal ring
A systematic review244 identified three studies that examined VTE among vaginal ring users compared to EE/LNG COC users. Two studies (one cohort105 and one case-control250 study) did not find a statistically significant difference between CVR and EE/LNG COC users. The third (cohort) study245 reported an increased risk of VTE (RR 1.9; 95% CI 1.3–2.7) in women using the CVR compared to EE/LNG COC users.
10.1.5 Women with inherited thrombophilias
Known thrombophilia is an absolute contraindication to CHC use (UKMEC 4).96
Women with inherited thrombophilias who use CHC are at significantly greater risk of VTE than CHC users without thrombophilia. A systematic review and meta-analysis251 which included data from 14 observational studies concluded that COC users with mild thrombophilias (e.g. factor V Leiden heterozygosity and prothrombin G20210A mutation) had a risk of VTE almost six times that of COC users without thrombophilia (RR 5.89; 95% CI 4.21–8.23); severe thrombophilias (e.g. antithrombin, protein C and protein S deficiencies and the homozygous forms of factor V Leiden and prothrombin G20210A) were associated with a more than 7-fold increase in VTE risk (RR 7.15; 95% CI 2.93–17.45).
Cohort studies included in the systematic review reported absolute risks of VTE as high as 4.3 (95% CI 1.4–9.7) and 4.62 (95% CI 2.5–7.9) per 100 pill years among COC users with antithrombin, protein C or protein S deficiency who also had a family member with both a thrombophilia and a VTE event. The authors of the review conclude that compared to the general CHC-using population (VTE risk of 6 per 10 000 woman-years), CHC users with a mild thrombophilia and a family history of VTE have an 8- to 33-fold increase in VTE risk; for CHC users with a severe thrombophilia and a positive family history, VTE risk is increased 70-fold. It is suggested that there could be co-inheritance of other thrombophilic defects.251
Thrombophilia screening
Screening for inherited thrombophilia in women with no known family history of thrombophilia is considered to be neither cost effective nor necessary.252,253 Screening women with a first-degree relative who has a hereditary thrombophilia is of uncertain benefit; studies evaluating the cost-effectiveness are of generally low quality.254 One limitation of these studies is that they consider only 1 year of COC use rather than the longer durations that reflect many women’s use. Furthermore, they do not take into account other situations that increase VTE risk – pregnancy, surgery, air travel – for which knowing thrombophilia status could be beneficial.
Due to the lack of high-quality evidence, the GDG advises that a woman with a first-degree relative who has an inherited thrombophilia can be counselled that a negative thrombophilia screen does not necessarily exclude thrombophilia (particularly if the relative has had a VTE event). A contraceptive method other than CHC that is not associated with increased VTE risk should be considered.
10.2 Arterial thromboembolic disease
Key information
C. Current use of CHC is associated with a very small increased risk of myocardial infarction (MI) and ischaemic stroke that appears to be greater with higher doses of estrogen in COC.
Clinical recommendation
C. Women should be informed that current use of CHC is associated with an increased risk of MI and ischaemic stroke but that that these events are still extremely uncommon in CHC users.
✓ Use of CHC by women with significant additional risk factors for arterial disease should be strongly cautioned or avoided.
The absolute risk of arterial thromboembolism (ATE) in young women is very low but increases markedly with age through a woman’s reproductive years.255 Most studies indicate that current use of CHC is associated with increased risk of ischaemic stroke and myocardial infarction (MI) compared to non-use of CHC; risk appears to increase with increasing dose of estrogen in COC. The absolute risk of ATE remains extremely small for CHC users; a large Danish cohort study reported 2.1 thrombotic strokes and 1.0 MI per 10 000 woman-years of use of hormonal contraception (the majority of the cohort used COC).255 However, any increase in risk is important because the morbidity and mortality associated with ATE events are significant. The risk of ATE among past-users of COC is similar to that for never-users.
FSRH UKMEC 201696 recommends that use of all CHC is either strongly cautioned or avoided for women with hypertension, women over the age of 35 years who smoke, women with multiple risk factors for cardiovascular disease including smoking, hypertension, high BMI, dyslipidaemias and diabetes, and for women with migraine with aura or migraine without aura that is of new onset during use of CHC.96 A family history of ATE events does not preclude use of CHC.
The evidence relating to risk of ATE and current use of CHC is summarised below. No RCTs are identified. The observational studies included are limited by the fact that ATE events are rare among women of reproductive age, data are often extracted from databases or self-reported by participating women, and data relating to bias and confounding factors are incomplete. Overall the evidence suggests that risk of ATE associated with COC use increases with increasing EE dose. Risk of ischaemic stroke does not appear to vary according to progestogen type in COC; risk of MI does not vary clearly according to progestogen type in COC, although some studies suggest that risk could be lower with third-generation progestogens than with first- or second-generation. Evidence relating to ATE risk with use of the CTP, CVR and estradiol-containing COC is limited, but risk appears to be similar to that associated with EE COC use.
10.2.1 CHC use and risk of myocardial infarction
A Cochrane Review256 of 24 observational studies found a significantly increased risk of MI for current users of COC compared with non-users (RR 1.6; 95% CI 1.2–2.1). The review included studies of users of older COC with higher EE content. Three earlier meta-analyses reported similar significant results (ORs 1.70 (95% CI 1.2–2.3), 1.84 (95% CI 1.38–2.44) and 2.48 (95% CI 1.91–3.22) for current use compared to non-use).257–259 One further meta-analysis210 found a non-significant increased risk of MI associated with current COC use (OR 1.34; 95% CI 0.87–2.08).
10.2.2 CHC use and risk of ischaemic stroke
A Cochrane Review256 found a RR for ischaemic stroke of 1.7 (95% CI 1.5–1.9) for current COC use compared to non-use. This is consistent with the findings of three previous meta-analyses which reported OR for ischaemic stroke in current COC users of 1.8 (95% CI 1.2–2.8),259 2.12 (95% CI 1.56–2.86)257 and 1.90 (95% CI 1.24–2.91)210 compared to non-users. A 2015 meta-analysis260 found a higher OR (OR 2.47; 95% CI 2.04–2.99) for first-time ischaemic stroke with current COC use compared with non-current use, however the risk declined significantly with decreasing estrogen dose.
10.2.3 Estrogen dose and risk of ATE
A Cochrane Review256 and a meta-analysis260 concluded that risk of ATE seemed to increase with higher doses of estrogen in COC.
Myocardial infarction: A large cohort study255 (data extracted from Danish databases) – which was included in the Cochrane Review – reported RR of MI of 1.4 (95% CI 1.07–1.81) for users of COC containing 20 µg EE and 1.88 (95% CI 1.66–2.13) for users of COC containing 30–40 µg EE compared to non-users. One meta-analysis258 of 19 case-control studies and four cohort studies found a significantly increased risk of MI with preparations containing 30–49 μg EE (OR 1.97; 95%CI 1.43–2.71) but no increased risk for 20 μg EE preparations (OR 0.92; 95% CI 0.21–4.08). A later (2016) large French cohort study237 reported a significantly lower risk of MI with use of COC containing 20 μg EE than with use of COC containing 30–40 μg EE (RR 0.74; 95% CI 0.67–0.82).
Ischaemic stroke: A meta-analysis260 found that the OR for ischaemic stroke was 1.56 (95% CI 1.36–1.79) in women using COC containing 20 µg EE, 1.75 (95% CI 1.61–1.89) for 30–40 µg EE and 3.28 (95% CI 2.49–4.32) for ≥50 µg EE compared with non-current COC use. The Danish cohort study reported a RR of ischaemic stroke of 1.60 (95% CI 1.37–1.86) for users of 20 µg EE and 1.75 (95% CI 1.61–1.92) for users of EE 30–40 μg compared to non-users. The 2016 French cohort study237 reported a significantly lower risk of ischaemic stroke with use of a COC containing 20 µg EE than with use of a COC containing 30–40 µg EE (RR 0.82; 95% CI 0.70–0.96).
10.2.4 Progestogen type and risk of ATE
A Cochrane Review256 concluded that risk of MI and ischaemic stroke did not vary clearly according to progestogen type.
Myocardial infarction: One meta-analysis259 found no significant association between progestogen type and risk of MI. A Danish cohort study reported RR for MI of 1.33–2.28 for use of 30–40 μg EE COC containing different progestogens (compared with non-use of CHC), but the differences in risk between progestogens were not significant.255 Two meta-analyses reported OR for MI compared with CHC non-use of 1.13 (95% CI 0.66–1.92)261 and 1.34 (95% CI 0.91–1.98)210 for use of third-generation COC, while for second-generation COC the OR were 2.18 (95% CI 1.62–2.94)261 and 1.79 (95% CI 1.16–2.75)210 and for first-generation COC, 3.37 (95% CI 2.04–5.54).210 One meta-analysis258 reported a significantly increased risk of MI for users of first- and second-generation COC compared to non-users (OR 2.21; 95% CI 1.30–3.76; p=0.004) and 2.17 (95% CI 1.76–2.69; p<0.0005), respectively), but not for users of third-generation COC (OR 1.27; 95% CI 0.96–1.67; p=0.094).
Ischaemic stroke: Two systematic reviews257,259 reported similar risk of ischaemic stroke for current users of second- and third-generation COC.
DRSP-containing COC: One large database cohort study found that women using COC containing EE 30 μg and DRSP had an increased risk of ATE compared to women using preparations of COC containing 20–35 μg EE and LNG, norethisterone or norgestimate but this risk was only statistically significant in women aged 35–55 years.262 Conversely, data from the EURAS study224 suggested a non-significant reduction in ATE risk with EE/DRSP compared to other COC, and the continuation of this study reported a significantly lower risk of ATE with EE/DRSP compared to other COC (adjusted HR 0.4; 95% CI 0.2–0.8).263 An Israeli cohort study reported similar ATE risks for users of EE/DRSP and second- and third-generation COC.264
10.2.5 Estrogen type and risk of ATE
The limited data relating to risk of ATE associated with use of COC containing estradiol suggest that risk is similar to that associated with EE COC.238
10.2.6 Route of administration and risk of ATE
A recent systematic review244 identified one cohort study265 and one case-control study246 that compared ATE risk for use of the CTP with that of COC containing norgestimate; neither study reported a significant difference in risk of MI or ischaemic stroke. Two prospective cohort studies were not included in the systematic review because the comparator group comprised users of multiple different COC; one reported similar risk of ATE for use of the CVR to that for use of (various) COC.263 The other study262 found no significant differences in ATE risk between users of the CTP, CVR and (various) COC.
10.2.7 Additional risk factors for ATE
Risk of ATE is greater for COC users with additional risk factors such as hypertension266 and smoking96 and may be increased by hyperlipidaemia.267
Migraine and risk of ischaemic stroke
The evidence (summarised below) suggests that CHC users with migraine with aura are at greater risk of ischaemic stroke than CHC users without migraine. UKMEC 201696 recommends that use of CHC by women who have migraine with aura is UKMEC 4. For women who have migraine without aura, initiation of CHC is UKMEC 2, but if there is new-onset migraine after starting CHC, the risks of continuation generally outweigh the benefits (UKMEC 3).
It is important to note that although relative risk of ischaemic stroke is increased, the number of ischaemic strokes in women of reproductive age is small and the absolute risk remains low. Using data from the UK General Practice Research Database the incidence of ischaemic stroke in all women aged 15–49 years was estimated at 3.56 (95% CI 3.05–4.07) per 100 000 per year.268
Meta-analysis of evidence from observational studies indicates that the risk of ischaemic stroke in individuals who have migraine is approximately twice that of those who do not have migraine.269–273 Four meta-analyses269,270,272,273 find a significant association between migraine with aura and ischaemic stroke, but only one272 reports a significant association for migraine without aura. Use of CHC independently increases the risk of ischaemic stroke (see Section 10.2.2).
Evidence is limited regarding risk of ischaemic stroke amongst women who have migraine and are also users of CHC.270,274,275 A 2016 systematic review274 concluded that the fair to poor quality evidence identified suggests an increased risk of stroke amongst CHC users with migraine compared with non-users of CHC who have migraine, and that the effect on ischaemic stroke risk of migraine and CHC are additive. A recent nested case-control study276 which considered data from US databases identified 25 887 ischaemic strokes amongst women aged 15–49 years between 2006 and 2012. Compared to women who did not have migraine and did not use CHC, the OR for ischaemic stroke was 1.8 (95% CI 1.1–2.9) for women with migraine without aura who also used CHC. This is similar to the OR observed for women with migraine without aura who did not use CHC (OR 2.2; 95% CI 1.9–2.7); CHC was not observed to further increase risk. For women who had migraine with aura, the OR for ischaemic stroke was 2.7 (95% CI 1.9–3.7) with no CHC use and increased to 6.1 (95% CI 3.1–12.1) if they also used CHC compared to women without migraine or CHC use.
10.3 CHC use and risk of haemorrhagic stroke
Two meta-analyses of data from observational studies report no significant increase in risk of haemorrhagic stroke among COC users (OR for current use of COC compared to non-use of COC 1.1 (95% CI 0.7–1.9)259 and 1.03 (95% CI 0.7–1.49)).210
10.4 Breast cancer
Clinical recommendation
C. Women should be advised that current use of CHC is associated with a small increased risk of breast cancer which reduces with time after stopping CHC.
10.4.1 CHC use and risk of breast cancer
Current CHC use
A recent large Danish cohort study reported a relative risk of breast cancer of 1.19 (95% CI 1.13–1.26) for current or recent users of COC compared to never-users of hormonal contraception.277 Risk appeared to increase with duration of use. No major differences in risk were observed between COC containing different progestogens. The study adjusted for potential confounding factors, but data for alcohol intake, age at menarche and breastfeeding were not available and those for BMI were incomplete.
Meta-analyses of data from observational studies,278,279 sometimes including use of older COC with higher estrogen content, have reported a slight but significant increased risk of breast cancer among women currently using COC compared with women who have never used CHC, the RR ranging from 1.19–1.24. One meta-analysis of five cohort studies found a very small but significant increase in breast cancer risk for every 5 years (RR 1.07; 95% CI 1.03–1.11) and 10 years (RR 1.14; 95% CI 1.05–1.23) of use; however, many of the individual studies did not have statistically significant findings.280 Three more recent studies, including the Oxford-Family Planning Association contraceptive study and a meta-analysis of 44 observational studies, found no link between duration of COC use and breast cancer risk.196,281,282
Past CHC use
Increased breast cancer risk associated with current COC use has been found to decline gradually after cessation of COC, with no significant increased risk of breast cancer after 10 years of non-use.196,278,283,284 Compared with never-use of CHC, reported RRs for breast cancer for ever-users of COC are close to unity (range 1.0–1.08) and non-significant.196,278,280,281,283,284 Very long-term follow-up of the RCGP Oral Contraception Study cohort indicates that the increased breast cancer risk that is seen in current and recent OC users appears to be lost within approximately 5 years of stopping, with no evidence of increased risk in later life.195 The evidence is that there is no significant association between use of COC and mortality from breast cancer.208,285–287
10.4.2 Family history of breast cancer
Women with a family history of breast cancer have an increased background risk of breast cancer compared to women with no such family history.288 Several studies do, however, suggest that women with a family history of breast cancer who have ever used CHC are at no higher risk of breast cancer than women with a family history who have never used CHC.204,278,289,290 UKMEC does not restrict use of CHC for women with a family history of breast cancer.96
10.4.3 Genetic mutations relevant to breast cancer risk
UKMEC states that for carriers of known gene mutations associated with breast cancer (e.g. BRCA mutations) the risks of using CHC generally outweigh the advantages.96 Women with such inherited mutations have a higher background risk for breast cancer.291–294 The evidence regarding whether CHC use further increases the risk of cancer for these women is inconsistent, with some systematic reviews/meta-analyses reporting conflicting findings among the studies considered295–297 and others finding no increased risk with CHC use.202–204
Three meta-analyses202–204 based on observational studies conclude that carriers of BRCA mutations who use COC have a reduced risk of ovarian cancer compared with never-users (RR 0.50, OR 0.57 and OR 0.58). This advantage would need to be weighed against the potential increased risk of breast cancer.
10.5 Cervical cancer
Clinical recommendation
C. Women should be advised that current use of CHC for more than 5 years is associated with a small increased risk of cervical cancer; risk reduces over time after stopping CHC and is no longer increased by about 10 years after stopping.
Collaborative analysis298 of data from 24 worldwide observational studies, including large UK cohort studies, suggested that current use of COC for more than 5 years approximately doubled the risk of invasive cervical cancer (RR 1.90; 95% CI 1.69–2.13) compared with never-use of COC. The risk declined after stopping COC, becoming the same as that for never-users about 10 years after cessation. The analysis reported no significant increase in risk of invasive cervical cancer associated with use of COC for less than 5 years.
Studies have consistently reported increased cervical cancer risk associated with current use of COC that increases with duration of use and decreases with time after cessation.283,299–301 Very long-term follow up of the RCGP Oral Contraception Study cohort indicates that the increased cervical cancer risk that is seen in current and recent OC users appears to be lost within approximately 5 years of stopping, with no evidence of increased risk in later life.195 Few studies consider the risk of cervical cancer among COC users who are human papillomavirus (HPV) positive.196
There is currently no evidence regarding whether the CVR, with its intravaginal administration, or the CTP are associated with different cervical cancer risk than COC. Women should be informed about the association between HPV and cervical cancer and given advice regarding condom use, smoking cessation, regular cervical screening and, where appropriate, HPV vaccination. See WHO Guideline Comprehensive Cervical Cancer Control: A Guide to Essential Practice.302
11. Side effects associated with CHC use
Some women using CHC report headaches, nausea, dizziness and breast tenderness. Different CHC preparations and modes of administration can prove more or less tolerable to individual women. It is important to note that there may be confounding factors contributing to women’s experience of side effects; RCTs have found that women report side effects at similar rates in treatment and placebo groups.303
As many CHC side effects arise during the HFI rather than during active pill use, shortened HFI or extended/continuous regimens may be helpful.3 Two systematic reviews27,28 reported that women who use extended CHC regimens benefit from greater improvement of menstrual symptoms associated with the HFI, including headaches, genital irritation, tiredness, bloating and menstrual pain compared to women who use CHC cyclically (see Section 6.2.5).
Women who develop side effects which they find unacceptable can be advised to consider a different formulation or mode of administration of CHC or a different contraceptive method which could have a more acceptable side effect profile.
11.1 CHC and headache
See Section 10.2.7 regarding use of CHC by women with migraine.
Headache is common among women of reproductive age, whether or not they use contraception. Headache is frequently reported as a side effect of CHC (often associated with the HFI) and is sometimes cited as a reason for CHC discontinuation, but in studies headache also occurs with placebo. Among women who have headache prior to CHC use, some women report worsening of headache after starting CHC while others report no change or improvement. Where an increase in headache is seen in the early cycles of CHC use this does not appear to persist with continued use.304,305
Studies investigating the effect of CHC use on headache are of overall poor quality, limited by a lack of information regarding which women had pre-existing headaches, absence of placebo arm or non-CHC using controls. Relevant studies consider different CHC preparations taken for different durations, with different comparators; some studies include migraine under the definition of headache where others do not. As a result, comparison and interpretation of data is difficult.
A 2005 systematic review304 and a 2013 comprehensive literature review305 found no consistent association between CHC use and headache, regardless of progestogen type and route of CHC administration. Lower estrogen doses do not appear to be associated with fewer headaches. Extended or continuous CHC regimens reduce the frequency of headaches associated with the HFI.
11.2 Unscheduled bleeding with CHC (breakthrough bleeding)
Unscheduled bleeding is a relatively common side effect of CHC. The incidence, regardless of route of administration, is around 10–18% per cycle.306–309 This is not very different from the background incidence of intermenstrual bleeding reported among a UK population. In a postal questionnaire survey of 2438 women, some of them using contraception (including CHC), over the course of 1 year self-reported cumulative incidence of intermenstrual bleeding was 17% (95% CI 14–19).310 HCPs should be aware of other causes of unscheduled bleeding such as missed pills, sexually transmitted infections, pregnancy and cervical pathology.
Some studies suggest that the incidence of unscheduled bleeding decreases with time. It is possible that women who find unscheduled bleeding unacceptable discontinue their method of contraception and so over the course of a trial bleeding patterns seem to improve. In some studies with small drop-out rates the improvement over time is convincing311 but in others the fall in incidence is in line with the decrease in the sample size as women discontinue participation in the study.309 Most studies do show that unscheduled bleeding is more likely in the first cycle, and some show an improvement over the first 3 months, with the incidence of unscheduled bleeding remaining constant from 4–12 months for both OC and the vaginal ring.311 It makes sense to recommend that women experiencing unscheduled bleeding continue their method for at least 3 months before seeking advice.312
11.2.1 Differences in bleeding pattern between routes of CHC administration
The nearly constant rate of release of contraceptive steroids administered transdermally or transvaginally, together with the theoretical advantages in respect of compliance, suggest that cycle control could be better than that with COC.313
OC versus CTP: A 2013 Cochrane Review99 identified four RCTs which compared cycle control among women using the EE/norgestimate patch to that among women using a variety of COC. None showed any differences in cycle control despite compliance being significantly better among patch users than among women using the COC in all three studies reporting compliance. More recently published studies have explored different formulations of patches, none as yet licensed.
OC versus CVR: In the 2013 Cochrane Review99 seven trials with the CVR reported bleeding data. Significant differences were found in four trials, all tending towards a lower incidence of breakthrough bleeding (at least in some cycles) among CVR users than among women using a variety of COC. One Chinese study published since the Cochrane Review311 compared the CVR with COC containing 30 μg EE/3mg DRSP. The authors reported significantly less bleeding/spotting in the CVR group than in the COC group for all 13 cycles (p<0.05) These differences are biologically plausible since there is greater bioavailability of steroids when administered through the vagina than through other routes.313
11.2.2 Differences in bleeding patterns between formulations of oral contraceptives
Many studies have attempted to show differences in bleeding patterns between different formulations of COC, however seldom do these studies compare like with like. For example, COC containing different progestogens are compared but they often also contain different doses of EE;314 monophasic formulations are compared with triphasic formulations;314 and regimens with 7 days of placebo pills are compared with a regimen with only two 2 days of placebo.308 The majority of such studies are undertaken by pharmaceutical companies as Phase 3 trials leading to licensing of a new product. The comparator pill could be chosen to maximise the chance of the new product showing non-inferiority. Moreover while the differences in the duration of unscheduled bleeding may be statistically significant, the effect is often small and unlikely to influence acceptability of the method; a difference between 12 and 15 days of unscheduled bleeding over 90 days may not be clinically significant.308
The evidence for an effect of the dose of estrogen on the incidence of unscheduled bleeding is more persuasive than that for an effect of different types of progestogen.
Effect of estrogen dose: A 2013 Cochrane Review315 of 22 RCTs concluded that women using 20 μg of EE experienced higher rates of unscheduled bleeding than women using >20 μg. One study merits specific mention. Although criticised in the review for not specifying who was blinded, Akerlund et al (1993)316 undertook an RCT comparing women using a COC containing 150 μg desogestrel with either 20 μg or 30 μg EE. Thus the progestogen component was the same in both groups. Women taking 20 μg EE were more likely to report irregular bleeding (OR 1.56; 95% CI 1.10–2.20). The difference between the incidence of unscheduled bleeding was statistically significant for 8 of the 12 months of follow-up.
Effect of progestogen type: A 2004 systematic review317 of 22 studies included two RCTs that reported less unscheduled bleeding with third- compared with second-generation progestogens (RR 0.71; 95% CI 0.55–0.91). These RCTs were limited by short study periods. Six RCTs found that cycle control was better with COC containing second-generation versus first-generation progestogens, both for monophasic (RR 0.69; 95% CI 0.52–0.91) and triphasic formulations (RR 0.61; 95% CI 0.43–0.85).
Effect of estrogen type: A number of studies have attempted to compare bleeding patterns among women using COC containing natural estrogens as opposed to those containing EE. Once again the type of progestogen is also different between the formulations, making the results difficult to interpret. Two RCTs comparing use of 1.5 mg 17β-estradiol/2.5 mg nomegestrol acetate30 and 30 μg EE/3 mg DRSP found that the incidence of unscheduled bleeding was comparable between the two formulations.318,319 One RCT comparing estradiol valerate/dienogest32 with 20 μg EE/100 μg LNG over seven cycles also found no difference in the proportion of women experiencing unscheduled bleeding, but reported that women in the estradiol group experienced fewer bleeding/spotting days (median 16 vs 21 during Days 1–90; 12 vs 15 during Days 91–180; p<0.0001).308
11.2.3 Differences in bleeding patterns between CHC regimens
See Section 6.2.4.
Unscheduled bleeding with CHC: summary
In summary, HCPs should inform women that unscheduled bleeding commonly occurs with CHC use but is likely to improve over the first 3–4 months of use. Formulations with higher doses of EE are probably associated with a lower risk of unscheduled bleeding when used in a traditional regimen, and pills containing second-generation progestogens could offer better cycle control than those containing norethisterone. Blood levels of exogenous hormones may vary 10-fold between individuals320 and intra-individual differences also occur, so what works for one woman may not work for another. Trial and error may therefore be the best approach for an individual woman to find a formulation that suits her needs. Extended or continuous regimens could offer less unscheduled bleeding. HCPs should consider other causes of unscheduled bleeding. For guidance on the management of unscheduled bleeding in women using hormonal contraception, refer to the FSRH Guideline Problematic Bleeding with Hormonal Contraception.312
11.3 Mood
Mood change is a common complaint among CHC users321 but a relatively infrequent reason for discontinuation.322 Numerous studies have tried to assess the magnitude of the effect of CHC on mood. A recent systematic review323 concluded that meta-analysis is not possible due to the wide heterogeneity between the studies which compare different types and formulations of hormonal contraceptives in the same cohort and use different instruments for assessing mood change. Other complicating factors include the well documented benefits for many women of CHC for PMS (see Section 9.3), menstrual pain (see Section 9.2) and vaginal bleeding patterns (see Section 11.2), all of which could themselves affect mood.
Few studies have compared healthy CHC users (not complaining of PMS or menstrual pain) with women not using hormonal contraception and even fewer are RCTs. One RCT among women who were sterilised or whose partners were sterilised taking a COC, POP or placebo found no difference in depressive symptoms by the third month of treatment.324 A recent large, double-blind RCT325 randomised 340 women in Sweden to a standard 30 μg EE/LNG COC or placebo taken for 21 days with a 7-day pill-free interval for three cycles.
Pregnancy was prevented with condoms. Scores using standardised instruments before treatment and at the end of 3 months showed a ‘modest’ decrease in general well-being among women using the COC but no differences in depressive symptoms. The predictable withdrawal bleed during the HFI could have prompted some women to guess that they were taking the COC, and in one survey of women who were asked about anticipated side effects before starting COC 20% said they expected to have mood changes.326
Most observational studies are reassuring. Four large epidemiological studies using standardised depression screening instruments among women using modern hormonal contraceptives undertaken in Australia,327 Finland328,329 and the USA330 showed no increase in the incidence of depression associated with CHC use. However a recently published Danish nationwide prospective cohort study reported a significant association between CHC use and depression. The study followed over 1.06 million women aged 15–34 years with no prior diagnosis of depression.331 Compared with non-users, current users of COC had a RR of first use of an antidepressant of 1.23 (95% CI 1.22–1.25), users of a CTP (RR 2.0; 95% CI 1.76–2.18) and users of a CVR (etonogestrel) (RR 1.6; 95% CI 1.55–1.69). The RR of first use of an anti-depressant was also increased among women using POP or LNG-IUS. Similar or slightly lower estimates were found for RR of first diagnosis of depression. Risk generally decreased with increasing age; adolescents (age range 15–19 years) using COC had a RR of a first use of an antidepressant of 1.8 (95% CI 1.75–1.84) and those using POPs (RR 2.2; 95% CI 1.99–2.52). However, significant confounding factors cannot be excluded and a causative association is not established.
The same authors found associations between ever-use of CHC and increased risk of first suicide attempt, and between ever-use of OC and increased risk of suicide compared with never-users of hormonal contraceptives.332 Risk did not differ significantly by COC formulation. Potential confounding factors including psychiatric diagnoses and antidepressant use were considered. Of previous cohort studies, one285 reported a positive association and four208,333–335 found no association between OC use and suicide.
While some studies have suggested differences in the incidence of mood change between COC formulations (EE dose316, progestogen type336) no consistent trends have been reported. It is possible that formulations containing an anti-androgenic progestogen such as drospirenone337,338 could have a more beneficial effect on mood than preparations containing other progestogens. Continuous use of CHC may be of benefit to mood.162 Data on the effects of the CVR or CTP are insufficient to allow any conclusions on their relative effects on mood.99
Effect of CHC on mood: summary
The evidence suggests that some women may experience negative mood changes when taking CHC. However there is not clear, consistent evidence that CHC use causes depression; mood change is common and often related to external events. The GDG recommends that if a woman who experiences negative mood changes wishes to continue using CHC, a different formulation containing an alternative progestogen could be tried empirically. If the negative mood change is premenstrual, continuous use of CHC may be of benefit.
11.4 Weight gain
There is no clear evidence that use of CHC causes weight gain. A 2014 Cochrane Review339 of 49 RCTs identified only four trials that compared CHC with placebo or with no intervention; the remainder compared different CHC formulations. The limited evidence does not support a causal association between use of CHC and weight gain, and there is no consistent evidence that different CHC formulations affect weight differently. A systematic review175 which identified data for women aged under 18 years from nine observational trials, concluded that there is no evidence of an association between CHC use and weight gain in this group of women.
11.5 Effect on libido
Libido is influenced by many social and psychological factors as well as age, health and medications. The available evidence regarding the potential effect of CHC on libido is mixed and is limited by use in different studies of different CHC preparations and assessment tools, and by lack of placebo control or a non-hormonal comparator group in many studies. Overall there is no clear evidence of an association between use of COC containing ≥20 μg EE and libido.
A 2013 systematic review340 included data for 8422 women using various CHC from 36 trials (five RCTs, the remainder observational studies). The review found no clear effect of CHC on libido. Despite the fact that active testosterone levels (where measured) were reduced during CHC use, COC users reported an increase in sexual desire in 15 studies and no impact on sexual desire in 12 studies. Decreased sexual desire was reported in nine studies. The identified evidence suggested that libido could be lower among women using COC containing <20 μg EE than in users of COC with ≥20 μg EE. A short subsequent trial341 which randomised 80 women to use either EE/DRSP COC or barrier/fertility awareness method (FAM) for 3 months reported lower Female Sexual Function Index (FSFI), desire and arousal scores for COC users.
11.6 Return to fertility
There is no evidence that use of COC is associated with subsequent long-term reduction in fertility.
Studies reporting return of ovulation after use of COC indicate that the majority of women ovulate within about a month of COC cessation whether they have used cyclical or extended COC regimens.74,342,343 Of 187 women stopping a 20 μg EE/LNG COC after at least 6 months of use in a cohort study, 98.9% returned to spontaneous menstruation (or became pregnant) within 90 days.73
The evidence from observational studies indicates that among women planning to conceive, pregnancy rates are high in the 2 years after stopping standard cyclical or extended regimen COC.344–346 A systematic review346 which included three prospective observational studies reported typical 1-year pregnancy rates following cessation of OCs ranging from 79.4% to 95.0%. Median time to pregnancy was 2.5–3 cycles. Cohort studies with a non-COC comparator group suggest that compared to women discontinuing barrier methods or who had not been using contraception, those stopping COC and planning to conceive experience a transient delay in conception over the first few months but that by 1–2 years pregnancy rates are comparable.347–352
There is no evidence that increasing duration of COC use is associated with reduced fertility. Some observational studies have in fact suggested that longer duration of COC use could be associated with greater fecundity than short-term use.351,353–355
12. What should be done in an initial CHC consultation?
Box 2 (which links to relevant sections) summarises the suggested content of an initial consultation with a woman who requests CHC. The consultation should focus on provision of safe, effective contraception that suits a woman’s requirements and that could also provide non-contraceptive benefits. Such a consultation is, however, an important opportunity to assess whether a woman is already at risk of pregnancy and could require emergency contraception or pregnancy testing, to assess STI risk and offer advice and testing, and to remind women about the importance of cervical screening.
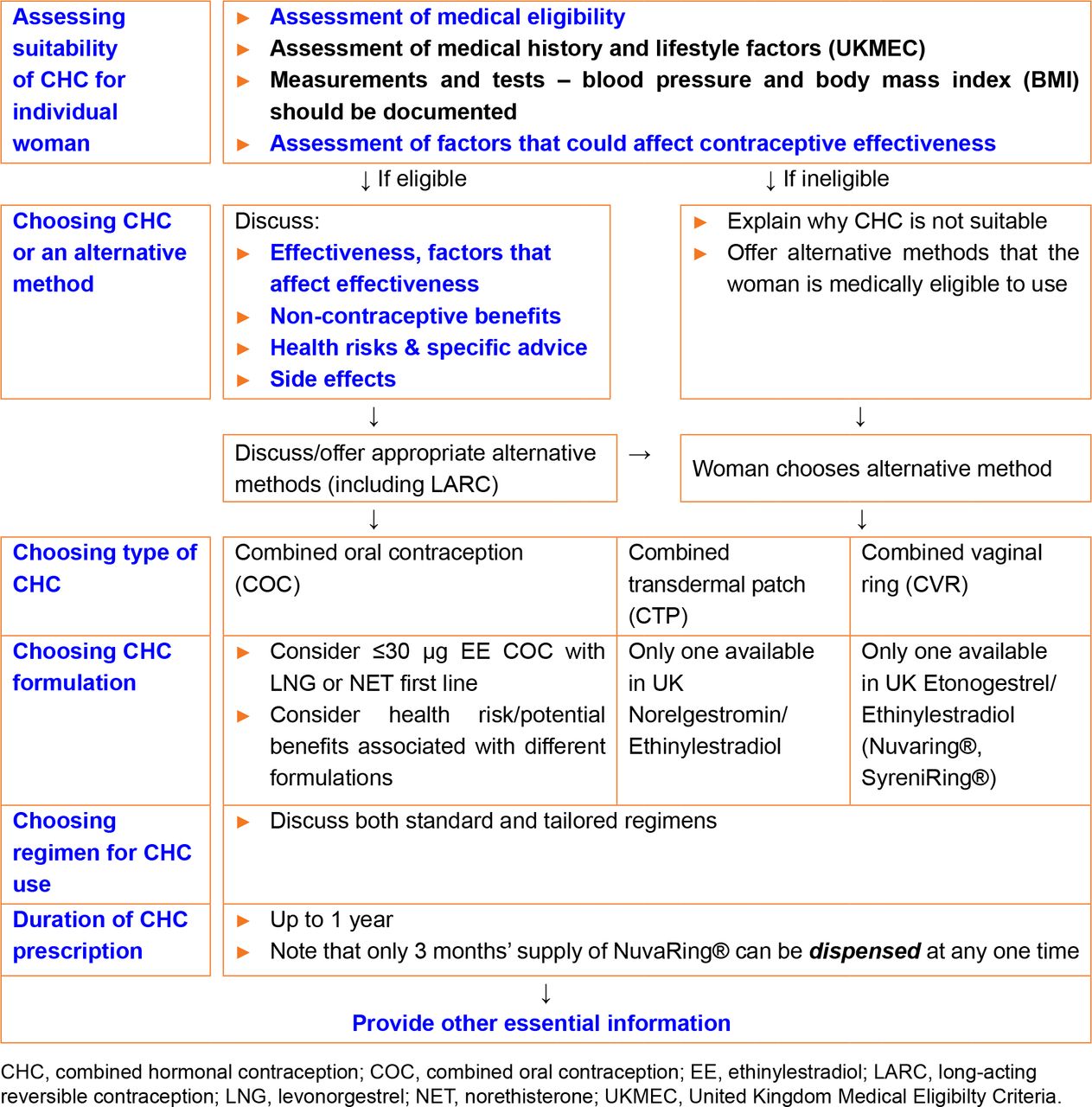
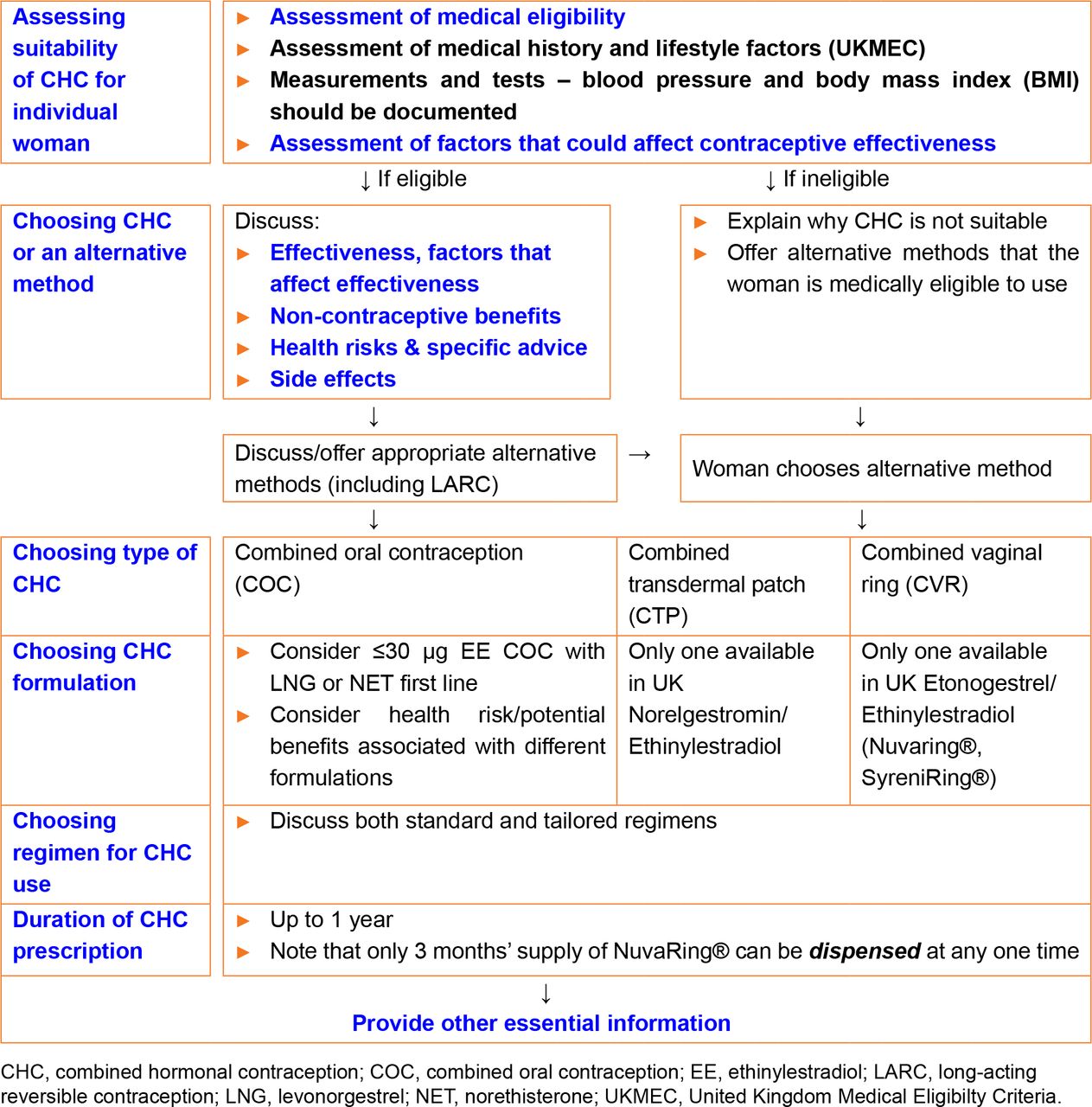{kind=link}
Suggested content of an initial combined hormonal contraception consultation (links to subsequent sections)
12.1 Assessment of suitability of CHC for an individual woman
Key information
C. Use of suitable self-completed checklists for medical eligibility appears to be accurate and acceptable to women.
Clinical recommendation
✓ Assessment of medical eligibility for CHC should include medical conditions, lifestyle factors and family medical history.
✓ A drug history should identify:-
any prescribed or non-prescribed drug that could affect the effectiveness of the contraceptive
any prescribed or non-prescribed drug that could itself be affected by the contraceptive
C. A recent, accurate blood pressure recording should be documented for all women prior to first CHC prescription.
D. BMI should be documented for all women prior to CHC prescription.
D. Pelvic examination is not required prior to initiation of CHC.
D. Breast examination, cervical screening, testing for thrombophilia, hyperlipidaemia or diabetes mellitus and liver function tests are not routinely required prior to initiation of CHC.
✓ Women for whom CHC is unsuitable should be offered alternative effective contraception.
The HCP should obtain a history that includes the woman’s age, past and current medical conditions, smoking, drug history (prescription, non-prescription and herbal preparations) and family history of significant medical conditions. BMI and blood pressure should be recorded.
12.1.1 Assessment of medical eligibility for CHC
Medical history and lifestyle factors
Medical eligibility must be assessed prior to prescription of any contraceptive method including CHC. The UK Medical Eligibility Criteria for Contraceptive Use 2016 (UKMEC 2016)96 provides recommendations for the safe use of CHC by women with different personal characteristics and medical conditions. Each of the personal characteristics or medical conditions considered by the UKMEC is assigned to one of four categories as defined in Table 6. UKMEC 3 and UKMEC 4 characteristics and conditions for CHC use are listed in Appendix 2. If a woman has multiple conditions that are UKMEC 2 for CHC use and relate to the same risk, the suitability of CHC should be carefully considered.
Definition of categories for the UK Medical Eligibility Criteria for Contraceptive Use (UKMEC)96
Appendix 2
Specific attention should be given to enquiring about:
Thrombophilia or previous VTE
Ischaemic heart disease, stroke or transient ischaemic attack, peripheral vascular disease
Additional risk factors for venous or arterial thromboembolism (e.g. smoking, obesity, recent childbirth, immobility, hypertension, migraine, diabetes, hyperlipidaemia, antiphospholipid antibodies, arrhythmia, complicated congenital/valvular heart disease or cardiomyopathy)
Personal history of breast cancer/known breast cancer-related gene mutation
Hepatobiliary disease
Recent childbirth, current breastfeeding.
Use of a self-completed checklist to assess medical eligibility for CHC
The use of a suitable self-completed checklist may be appropriate for identifying personal characteristics, medical conditions or use of medication that could affect medical eligibility for CHC. Four studies (two from the USA356,357 and one each from the UK358 and Tanzania359) which examined assessment of medical eligibility for CHC using questionnaires self-completed by women compared to clinical assessment by trained providers reported high levels of agreement between women and HCPs. All four studies found that women were more likely than providers to identify contraindications. The UK study concluded that no clinically important information relevant to a particular woman’s use of CHC was missed and none of the women would have been wrongly prescribed CHC based only on their self-completed questionnaires.
If self-assessment checklists are used they should be developed and validated to ensure that they are effective.
Measurements and tests
Blood pressure and body mass index (BMI) should be documented for all women before prescription of CHC. The prescriber must be confident that measurements are recent and accurate.
Blood pressure: Women with severe hypertension (systolic pressure ≥160 mmHg or diastolic pressure ≥100 mmHg) should not use CHC (UKMEC 4). Women with less severe hypertension (systolic pressure 140–159 mmHg or diastolic pressure 90–99 mmHg), or with adequately controlled hypertension should not use CHC (UKMEC 3). Blood pressure should therefore be evaluated before initiating CHC.
Evidence from a systematic review360 suggests that risk of MI and ischaemic stroke is higher among women who do not have their blood pressure measured before initiating COC.
Women with raised blood pressure measured in non-primary care settings (e.g. at a pharmacy or specialist services) should be provided with suitable alternative effective contraception and advised to see their general practitioner for blood pressure assessment.
Weight (BMI): Women with BMI <35 kg/m2 generally can use CHC (UKMEC 2). Women with BMI ≥35 kg/m2 generally should not use CHC (UKMEC 3), although CHC may be prescribed by a specialist provider. BMI should be documented before starting CHC. Baseline weight could additionally be helpful for monitoring any changes and counselling women who might be concerned about later weight change perceived to be associated with their contraceptive method.
Pelvic examination: A consultation regarding contraception may be used as an opportunity for health screening but screening should not be a condition for prescribing. Pelvic examination is not necessary before initiation of CHC because it does not affect the decision to prescribe or withhold hormonal contraception.361
Clinical breast examination: Although women with current breast cancer should not use CHC (UKMEC 4), screening asymptomatic women with a clinical breast examination before initiating CHC is not necessary because of the low prevalence of breast cancer among women of reproductive age. A systematic review361 did not identify any evidence regarding outcomes among women who were screened versus not screened with a breast examination before initiation of hormonal contraceptives. Breast self-examination can be encouraged.
Laboratory testing: A systematic review362 conducted to evaluate the evidence regarding health outcomes among women with and without laboratory testing to identify certain medical conditions, including diabetes, hyperlipidaemia, liver disease, cervical cancer, STIs or human immunodeficiency virus (HIV), prior to initiating contraceptives did not identify any relevant evidence.
The GDG (in line with the WHO Selected Practice Recommendations for Contraceptive) advise that routine screening and examination other than blood pressure and BMI are unnecessary prior to prescription of CHC and do not contribute substantially to the safe and effective use of CHC.
12.1.2 Assessment of factors that could affect contraceptive effectiveness
Drug interactions
Some medications could reduce the contraceptive effectiveness of CHC by induction of hepatic enzymes. Contraceptive hormones can affect the action of certain medications. Refer to the FSRH Guideline Drug Interactions with Hormonal Contraception118 for further information. (See also Section 7.2.3).
Malabsorption
The effectiveness of COC (but not the CTP or CVR) could be reduced by malabsorption resulting from, for example, vomiting and severe diarrhoea (see Section 7.2.4), bariatric surgery, small bowel resection (see Section 7.2.2) or inflammatory bowel disease (see FSRH Guideline Sexual and Reproductive Health for Individuals with Inflammatory Bowel Disease).363
12.1.3 Women for whom CHC is unsuitable
Women assessed as medically ineligible for CHC should be told why, and the risk to their health should be explained. Alternative contraceptive methods which can be safely used should be discussed and offered.
Women with medical conditions or using medications that could reduce contraceptive effectiveness should be given advice regarding (and where possible provided with) alternative methods that would be effective for them.
12.2 Choosing a method of contraception
Women requesting CHC who are assessed as medically eligible should be provided with the following information about CHC to enable them to make an informed decision as to whether the method is suitable for them:
Effectiveness and factors that can affect effectiveness (see Section 7)
Non-contraceptive benefits (see Section 9)
Health risks (see Section 10)
Side effects (see Section 11)
Women should also be offered information about, and be given the opportunity to discuss, other suitable contraceptive methods. However, care should be taken to ensure that women do not feel coerced into choosing any particular method. For further information about alternative methods refer to the other method-specific FSRH Guidelines and to UKMEC 2016, available on the FSRH website.
12.3 Choosing type and formulation of CHC
Key information
✓ COC containing ≤30 μg EE in combination with levonorgestrel or norethisterone is a reasonable first-line choice of CHC to minimise cardiovascular risk.
Women should be informed that CHC is available as COC, CTP and CVR and that different formulations of COC are available. When supporting women to make an initial choice of CHC, providers should explain that some types of CHC are associated with a lower risk of cardiovascular events than others; it should, however, be made clear that differences in the numbers of such events are small. It may be useful for a woman to know that there is no clear evidence that there are fewer problematic side effects (as opposed to risks) with any particular CHC. However if side effects are experienced with one formulation another could be more suitable.
The GDG recommends that a COC containing ≤30 µg EE in combination with levonorgestrel or norethisterone is a reasonable first-line choice of CHC to minimise cardiovascular risk.
12.4 Choosing a regimen for CHC use
Women should be provided with information regarding both standard and tailored CHC regimens (see Section 6). CHC providers should assess women’s preferences regarding frequency of scheduled bleeding and associated withdrawal symptoms to support women in making informed choices about the CHC regimen that best meets their needs.
Key messages that may be useful when discussing extended or continuous regimens are included in Box 3.
Key messages for women considering use of tailored combined hormonal contraception regimens
The evidence from studies is that combined hormonal contraception (CHC) is as safe and at least as effective for contraception if it is taken as an extended or continuous regimen as it is when it is taken in a traditional 21/7 cycle.
A woman who is using CHC does not need to have a monthly withdrawal bleed to be healthy.
There is no build-up of menstrual blood inside a woman who uses CHC for an extended time without a break; extended CHC use keeps the lining of the womb thin.
Withdrawal bleeds during cyclical use of CHC have been reported by women who are pregnant; women should not consider monthly bleeds on CHC to be reassurance that they are not pregnant.
By using extended or continuous CHC the frequency of withdrawal bleeds and associated symptoms (e.g. headache, mood change) is reduced; this could be useful for women who have heavy or painful bleeding or problematic symptoms associated with the hormone-free interval (HFI).
The ovaries start to become active during the traditional 7-day HFI. Fewer and/or shorter breaks in CHC use could mean that the risk of pregnancy could theoretically be lower with extended or continuous regimens than if a 7-day break is taken every month.
There can be irregular bleeding or spotting in the first few months of CHC use, particularly with extended or continuous regimens; this does not usually mean that there is any medical problem and it generally improves with time.
The evidence from studies is that using extended or continuous regimens of CHC does not affect the return of a woman’s fertility when she stops CHC.
12.5 Other important supporting information
Clinical recommendation
✓ Women should be provided with written information or a link to a trusted online resource to support safe, effective CHC use.
It is important that women are offered the opportunity to ask questions. Women should be provided with the following information regarding use of their chosen CHC:
When/how to start the method (see Section 6.3), highlighting whether additional contraceptive precaution is required before the contraceptive effect of CHC can be relied upon
What to do when the method is used incorrectly or inconsistently (see Section 8) and when emergency contraception may be indicated
Health risks associated with use of CHC (see Section 10) and specific advice for travel, living at altitude and having surgery (see Section 14)
Key signs and symptoms that should alert them to seek medical advice (see Box 4)
Significant new health events that should prompt them to review their contraceptive method (see Box 4)
Advice that they should check with the prescriber of any new medication or with their contraceptive provider whether any new prescribed or non-prescribed drug could affect the contraceptive effectiveness of CHC
Arrangements for subsequent prescription of CHC (including obtaining an emergency supply) and follow-up (see Section 13)
What to do if they wish to discontinue CHC or change their contraception (see Section 15).
Women using combined hormonal contraception: key indications for medical review
Key symptoms that should prompt women to seek urgent medical review
Calf pain, swelling and/or redness
Chest pain and/or breathlessness and/or coughing up blood
Loss of motor or sensory function
Key symptoms that should prompt women to seek medical review
Breast lump, unilateral nipple discharge, new nipple inversion, change in breast skin
New onset migraine
New onset sensory or motor symptoms in the hour preceding onset of migraine
Persistent unscheduled vaginal bleeding
New medical diagnoses that should prompt women to seek advice from their contraceptive provider (and review of the suitability of CHC)
High blood pressure
High body mass index (>35 kg/m2)
Migraine or migraine with aura
Deep vein thrombosis or pulmonary embolism
Blood clotting abnormality
Antiphospholipid antibodies
Angina, heart attack, stroke or peripheral vascular disease
Atrial fibrillation
Cardiomyopathy
Breast cancer or breast cancer gene mutation
Liver tumour
Symptomatic gallstones
Verbal information-giving should be supported by a comprehensive leaflet or direction to a trusted website.
12.6 Duration of CHC prescription
Clinical recommendation
C. HCP can prescribe up to 12 months’ supply of CHC for women who are initiating or continuing CHC.
In line with the WHO Selected Practice Recommendations85 the GDG advises that provision of up to a 1-year supply of CHC may be appropriate depending on the woman’s preference and anticipated use. Restriction of the length of supply could result in unwanted discontinuation of the method and increased risk of pregnancy. Although there could be some potential wastage, cost and use of resource associated with frequent follow-up appointments are avoided. It may be appropriate to provide a more limited supply (e.g. 3 months) for women who would benefit from returning for a follow-up visit (e.g. women with pre-existing significant medical conditions).
12.6.1 Combined oral contraception
A systematic review364 suggested that provision of a greater number of packs of COC was associated with increased rates of continuation. Studies that compared provision of 1 vs 12 packs, 1 vs 12 or 13 packs, or 3 vs 7 seven packs found increased continuation of pill use among women provided with more pill packs.365–367 Provision of more pills packs was associated with fewer pregnancy tests, fewer pregnancies, and lower costs for users. However, a greater number of pill packs (i.e. 13 packs vs 3 packs) was also associated with increased pill wastage in one study.365
12.6.2 Combined transdermal patch
No evidence was identified on which to base recommendations for the number of packs of patches provided but once a woman is established on CTP, provision of a 12-month supply is reasonable.
12.6.3 Combined vaginal ring
Following manufacture, supplies of Nuvaring have to be kept refrigerated. After dispensing, Nuvaring can be stored at room temperature and used within a maximum of 4 months. Therefore no more than one pack of three Nuvaring can be provided at any one time. Arrangements should be made for repeat prescription to prevent users routinely having to return to the provider more than once per year. SyreniRing does not required refrigeration and a one-year supply can be dispensed.
13. What follow-up is required for women continuing with use of CHC?
13.1 What follow-up arrangements are appropriate?
Clinical recommendation
✓ Women should be advised that routine annual review of their contraception is recommended during CHC use.
The GDG recommend that women who continue CHC should be routinely reviewed on an annual basis; routine follow-up, including annual recording of blood pressure and BMI measurement may be achieved without a face-to-face consultation. Women with certain existing medical conditions may benefit from attending more frequently or for face-to-face follow-up.
All women should be advised to return or seek professional advice at any time if they are experiencing troublesome side effects, have a significant new health event, start new medication, wish to discontinue CHC or to discuss alternative methods.
There is no evidence that frequent follow-up improves correct or continued use of CHC. A systematic review368 which identified two studies found little difference in effective contraceptive use between adolescents who had (telephone) contact with their provider and those who did not. A randomised trial of daily text message reminders among women with a mean age of 22 years did not improve OC adherence.132
13.1.1 What should be done at CHC follow-up?
Clinical recommendation
✓ Medical eligibility, drug history, method adherence and method satisfaction should be reassessed at follow up. BMI and blood pressure should be recorded.
Routine follow-up has long been considered an essential aspect of ensuring the safety of contraceptive use and a way to ensure adherence. At follow-up, medical eligibility should be rechecked, drug history updated, method adherence and method satisfaction assessed, and alternative contraceptive options considered. Women should be reminded about signs, symptoms, health events and changes in medication that should prompt them to seek medical review.
Weight and blood pressure have been the two parameters considered most important with respect to routine follow-up.
Weight/BMI: A systematic review339 identified no large effect of CHC use on weight gain. In one matched cohort study of adolescents using COC published since this review,369 BMI increased by a mean of 0.04 kg/m2 per month among COC users versus 0.025 kg/m2 per month among controls. If BMI is ≥35 kg/m2 at follow-up, women should be advised to switch to an alternative method of contraception.
Blood pressure: A systematic review370 of five studies, with methodological limitations, examining blood pressure after CHC initiation, generally showed that only a small percentage of women (2% in the largest study) develop hypertension between 1 and 24 months after starting hormonal contraception. One matched cohort study published since this review found no significant changes in blood pressure among adolescents using COC during 18 months of follow-up when compared with controls.369 No studies were identified that examined changes in blood pressure with time among patch users. A small study of 18 women suggested that in normotensive women, the CVR slightly increased 24-hour ambulatory blood pressure after six cycles of use.371 The increase was statistically significant but small (mean 24-hour blood pressure increased by 2.69 ± 5.35 mmHg) and clinical relevance is uncertain.
Since hypertension increases the risk of MI and stroke, the GDG recommend that a woman wishing to continue using CHC should have her blood pressure checked annually to ensure that it remains within the acceptable range.
13.2 Online and remote provision of CHC
At the time of publication of this guideline, little has been published in the peer-reviewed literature about remote prescribing of CHC. A number of pilot projects have been started but evaluation is still awaited.372
The recommendation of the GDG is that both remote and online prescribing are suitable for CHC. The checks that are suggested above can all take place remotely, and therefore a face-to-face consultation is not necessary for safe prescribing.
The General Medical Council (GMC) provides guidance on safe prescribing for doctors.373 If the doctor has adequate knowledge of the patient’s health and is satisfied that the medicine will serve the patient’s needs, remote prescribing is acceptable. For CHC, doctors prescribing remotely must ensure that the woman does not have any health conditions categorised as UKMEC 3 or UKMEC 4 for CHC. A recent blood pressure measurement taken by a HCP or obtained at a self-testing station (e.g. in a general practitioner surgery) is acceptable for the purposes of prescribing CHC and may be self-reported by the woman. Recent height and weight measurements may be taken and self-reported by the woman.
For other information, self-completed questionnaires have been shown to be safe and adequate, as outlined in Section 12.1.1. As more evidence becomes available about online prescribing, the FSRH Clinical Effectiveness Unit (CEU) will consider whether further guidance becomes appropriate.
14. What specific advice is required for women using CHC?
14.1 CHC use during travel
Clinical recommendation
C. Women using CHC should be advised about reducing periods of immobility during travel.
14.1.1 VTE risk during travel
Long duration travel is a weak risk factor for VTE. The risk is not confined to air travel (although most of the evidence relates to flying), increases with the duration of travel and with the presence of pre-existing risk factors for VTE. The British Society for Haematology bases its recommendations on a systematic review of the evidence.374 Data from prospective studies which evaluated air travellers for deep vein thrombosis (DVT) before and after their journeys suggest an incidence of DVT of 1 in 560 people travelling by air for 8 hours. Retrospective studies suggest that pulmonary embolism is extremely rare in flights of <8 hours but that the risk is associated with the duration of travel (5/million in flights >12 hours) and with pre-existing risk factors for VTE. There is indirect evidence that maintaining mobility during travel is a reasonable precaution, while for people without pre-existing risk factors, compression stockings and anti-platelet drugs (aspirin) are not indicated.
Case reports have suggested that CHC use could be associated with further increased risk of VTE associated with travel.375 The GDG recommends that women using CHC should minimise immobility during travel, but existing evidence is inadequate to allow any recommendation to be made about use of compression stockings or anti-platelet drugs.
14.1.2 Adherence to CHC when crossing time zones
Women travelling through different time zones should be reminded of the importance of taking their COC pill approximately 24 hours after their most recent pill (i.e. using the time of day in the time zone in which the last pill was taken as a reference point rather than local time).
A COC is missed when it has been more than 24 hours since the pill should have been taken. Two pills have been missed when it has been more than 72 hours since the last pill was taken. Refer to Section 8.1 for advice on missed CHC.
14.2 CHC use at high altitude
Clinical recommendation
D. Women trekking to high altitudes (above 4500 m or 14 500 feet) for periods of more than 1 week may be advised to consider switching to a safer alternative contraceptive method.
Exposure to high altitude results in an increase in erythropoiesis and in the risk of thrombosis.
Environmental factors associated with climbing to high altitude (hypoxia, dehydration, low temperature and enforced immobility due to bad weather) all contribute to the risk. Despite lack of robust evidence and few reported cases, experts recommend that women should consider avoiding CHC if they are to spend more than a week above 4500 m (14 764 feet).376 Below this altitude, use of CHC is likely to be safe in a healthy, active, non-smoking woman with no personal or family history of venous thrombosis or thrombophilia.
14.3 Surgery/periods of immobilisation
Clinical recommendation
D. Women should be advised to stop CHC and to switch to an alternative contraceptive method at least 4 weeks prior to planned major surgery or expected period of limited mobility.
Women who are immobile or have restricted mobility for an extended period of time (due to surgery or other reasons) are at increased risk for VTE. This risk may be further increased with use of CHC.
With regard to the use of CHC by women undergoing surgery, the British National Formulary377 advises that “estrogen-containing contraceptives should preferably be discontinued (and adequate alternative contraceptive arrangements made) 4 weeks before major elective surgery and all surgery to the legs or surgery which involves prolonged immobilisation of a lower limb; they should normally be recommenced at the first menses occurring at least 2 weeks after full mobilisation. A progestogen-only contraceptive may be offered as an alternative and the estrogen-containing contraceptive restarted after mobilisation. When discontinuation of an estrogen-containing contraceptive is not possible, e.g. after trauma or if a patient admitted for an elective procedure is still on an estrogen-containing contraceptive, thromboprophylaxis (with unfractionated or low molecular weight heparin and graduated compression hosiery) is advised. These recommendations do not apply to minor surgery with short duration of anaesthesia (e.g. laparoscopic sterilisation or tooth extraction), or to women using oestrogen-free hormonal contraceptives.”
15. What recommendations are there regarding stopping CHC?
15.1 How long can women use CHC?
Clinical recommendation
D. CHC can be used by medically eligible women for contraception until age 50 years.
15.1.1 Use of CHC by women aged over 40 years
Women may use CHC for contraception until age 50 years provided there are no contraindications as outlined in UKMEC.96 After age 50 years, the risks of CHC use generally outweigh the contraceptive benefits and women should be advised to switch from CHC to a POP, subdermal implant, LNG-releasing IUS or a non-hormonal contraceptive method.378 Women taking CHC for non-contraceptive benefits who wish to continue use after the age of 50 years should be considered on an individual basis. See FSRH Guideline Contraception for Women Aged Over 40 Years.378
15.1.2 Duration of CHC use
For medically eligible women under the age of 50 years, there is no arbitrary maximum length of time for which CHC can be used. Repeated starting and stopping of CHC should be discouraged because VTE risk is highest in the months after initiation or when restarting after a break of at least 1 month (see Section 10.1).
15.2 Switching to another method of contraception
Women who wish to switch to a different method of contraception should be advised whether additional contraceptive precaution (i.e. barrier methods/ abstinence) is required, and for how long (see Table 7).
Recommendations for additional contraceptive precautions when switching from combined hormonal contraception to another method
15.3 Planning pregnancy
15.3.1 Return of fertility
Women who wish to conceive after stopping contraception should be advised that after stopping CHC there is no significant delay in return to fertility and conception rates are comparable to those among women stopping other contraceptive methods or using no contraception (see Section 11.6). Folic acid supplementation can be started prior to stopping CHC.
15.3.2 Preconception care
Refer to the FSRH Clinical Statement Preconception Care.379
15.3.3 Unplanned pregnancy during CHC use
The available evidence suggests that fetal exposure to CHC is not associated with fetal abnormality (see Section 6.3.2). See FSRH Guideline Quick Starting Contraception.86
16. Use of CHC in the perimenopause
16.1 Use of CHC as an alternative to HRT
Clinical recommendation
D. CHC can be considered for use by medically eligible women until age 50 as an alternative to HRT for relief of menopausal symptoms and prevention of loss of bone mineral density as well as for contraception.
Use of CHC can suppress menopausal symptoms, regulate bleeding and maintain BMD in the perimenopause (see Section 9). CHC can therefore be used by eligible women aged under age 50 years as an alternative to HRT as well as for contraception. During use of CHC, serum levels of estradiol, FSH and LH are suppressed and cannot be used to inform advice regarding menopausal status.380,381
Estradiol/nomegestrol acetate and estradiol valerate/dienogest COC formulations contain estradiol rather than the synthetic EE present in most COC. They share some similarities with HRT preparations, rather than EE COC, so have theoretical safety benefits for women aged over 40 years. However, evidence relating to specific benefits or risks associated with their use is not yet available and FSRH advice relating to CHC in general is currently considered to apply also to estradiol COC.
16.2 Transition to HRT
Women using CHC should be advised to switch to a suitable alternative method of contraception at the age of 50 years, or if they develop medical contraindications to use of CHC, or if they prefer not to use CHC for contraception; if HRT is indicated for control of menopausal symptoms or maintenance of BMD it can be used alongside the (non-CHC) contraceptive method. See FSRH Guideline Contraception for Women Aged Over 40 Years.378
Recommendations for future research
Safety, effectiveness and acceptability of COC regimens that have estrogen-only pills in place of a HFI
Safety and effectiveness of CHC regimens with shortened HFI
Safety, effectiveness and acceptability of continuous CHC regimens
Comparison of bleeding patterns with continuous use of different CHC regimens
Safety and effectiveness of estradiol COC compared to EE COC
Safety, feasibility and acceptability of COC provision (initiation/continuation) at the pharmacy
Considerations for implementation of this guideline
Patient group direction (PGD) for tailored COC regimens
Training and resources to support HCPs discuss tailored regimens with women
Patient resources to support safe and effective tailored CHC use
Useful links
Questions for continuing professional development
The following multiple choice questions (MCQ) have only one correct answer and have been developed for continuing professional development (CPD). The answers to the questions and information on claiming CPD points can be found in the ‘members-only section’ of the FSRH website (www.fsrh.org).
A woman taking lamotrigine is using the combined hormonal transdermal patch (CTP). Which one of the following statements is correct?
a) Lamotrigine is a liver enzyme inducer and will reduce hormone levels
b) Serum lamotrigine levels can be reduced by CTP
c) Lamotrigine levels are unchanged in the hormone-free interval (HFI)
d) The benefits of using CTP with lamotrigine usually outweigh the risks
A woman attends clinic and is 3 days late restarting her combined oral contraception (COC) and had unprotected sexual intercourse (UPSI) only on day 6 of her 7-day HFI having previously taken her pills consistently and correctly. Which one of the following statements is incorrect?
a) She is at risk of pregnancy
b) Copper intrauterine device (Cu-IUD) would not be first choice for emergency contraception in this situation.
c) Ulipristal acetate (UPA) is a suitable choice of emergency contraception in this case
d) If UPA is chosen, she needs to wait 120 hours before restarting her COC
Which one of the following statements about venous thromboembolic (VTE) risk with CHC is correct?
a) VTE risk when using CHC is lower than VTE risk during pregnancy/after delivery
b) Taking breaks from the pill is recommended as this reduces VTE risk
c) VTE risk is higher with LNG- and norethisterone-containing COC compared to those containing desogestrel
d) A thrombophilia screen is recommended before starting combined hormonal contraception (CHC)
A woman suffers from headache and nausea in the HFI. Which one of the following is an inappropriate option to reduce symptoms?
a) Tricycle pill packets
b) Take pills continuously
c) Flexible extended pill taking
d) Increase estrogen dose to 35µg
Which one of the following conditions is not UKMEC 3 for CHC use?
a) Body mass index (BMI) ≥35 kg/m2
b) Breast feeding and ≥6 weeks to < 6 months post-partum
c) Age >35yrs and smoking < 15 cigarettes a day
d) Hypertension with systolic >140–159 mmHg or diastolic >90–99 mmHg
Regarding switching to CHC, which one of the following statements is incorrect?
a) 7 days of extra precautions are needed if CHC is started after taking desogestrel progestogen-only pills (POP) consistently and correctly
b) No extra precautions are needed if CHC is started on same day as in-date subdermal implant is removed
c) 7 days of extra precautions are needed if CHC is started on the same day that an in-date levonorgestrel-releasing intrauterine system (LNG-IUS) is removed
d) Up to 9 days of extra precautions are required if an estradiol-containing COC is started and an in-date Cu-IUD is removed on day 3 of a menstrual cycle
Which one of the following statements is incorrect regarding a woman who wants to switch from CHC and is on day 6 of the HFI?
a) If she has a Cu-IUD inserted today, no additional precautions are needed
b) If she is starts a POP today and has not had UPSI in the HFI, 2 days of additional precautions are needed
c) If she has a subdermal implant inserted today and has had UPSI in the HFI she should restart her CHC for 7 days
d) If she has a LNG-IUS inserted today, and has not had UPSI in the HFI, no additional precautions are required
Which one of the following statements is incorrect regarding cancer and CHC use?
a) Use of CHC is contraindicated for a woman whose mother had breast cancer
b) Increased risk of breast cancer associated with CHC use declines to become non-significant after 10 years of non-use
c) Use of CHC for more than 5 years is associated with a small increase in the risk of cervical cancer
d) Use of CHC is associated with reduced risk of endometrial cancer and ovarian cancer
Which one of the following drugs does not alter the effectiveness of CHC?
a) St. John’s Wort
b) Modafinil
c) Sodium valproate
d) Topiramate
Which one of the following statements regarding CHC and migraine is correct?
a) CHC users with migraine with aura are at greater risk of haemorrhagic stroke than CHC users without migraine
b) Starting CHC for a woman who has pre-existing migraine without aura, is UKMEC 2
c) If >5 years have elapsed since a woman’s last migraine with aura, benefits of CHC use outweigh risks
d) If a woman suffers from migraine without aura in the HFI, using an extended cycle regimen will not be beneficial
Auditable outcomes
The following auditable outcomes have been suggested by the FSRH Clinical Standards Committee.
Comments and feedback on published guideline
All comments on published this guideline can be sent directly to the Clinical Effectiveness Unit (CEU) of the Faculty of Sexual & Reproductive Healthcare (FSRH) via the FSRH website (www.fsrh.org).
The CEU may not respond individually to all feedback. However, the CEU will review all comments and provide an anonymised summary of comments and responses, which are reviewed by the Clinical Effectiveness Committee (CEC) and any necessary amendments made subsequently.
The Faculty of Sexual & Reproductive Healthcare (FSRH) is the largest UK professional membership organisation working in the field of sexual and reproductive health (SRH). We support healthcare professionals to deliver high-quality healthcare including access to contraception. We provide our 15 000 doctor and nurse members with NICE-accredited evidence-based clinical guidance, including the UKMEC, the gold standard in safe contraceptive prescription, as well as clinical and service standards.
The FSRH provides a range of qualifications and training courses in SRH, and we oversee the Community Sexual and Reproductive Healthcare (CSRH) Specialty Training Programme to train consultant leaders in this field. We deliver SRH-focused conferences and events, provide members with clinical advice and publish BMJ Sexual & Reproductive Health – a leading international journal. As a Faculty of the Royal College of Obstetricians and Gynaecologists (RCOG) in the UK, we work in close partnership with the College but are independently governed.
The FSRH provides an important voice for UK SRH professionals. We believe it is a human right for women and men to have access to the full range of contraceptive methods and SRH services throughout their lives. To help to achieve this we also work to influence policy and public opinion working with national and local governments, politicians, commissioners, policymakers, the media and patient groups. Our goal is to promote and maintain high standards of professional practice in SRH to realising our vision of holistic SRH care for all.
References
Online references accessed on 27 June 2018.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
Correction notice Since this set of guidelines were published online the following changes have been made:
February 2019 – Table 4; The rates for perfect use of progestogen-only pill, progestogen-only injectable and levonorgestrel intrauterine device have been corrected from 0.2, 0.6 and 0.6 to 0.3, 0.2 and 0.2, respectively.
July 2019 – Appendix 2; condition description for breast conditions e(i) Current and e(ii) Past and no evidence of current cancer for 5 years has been corrected to e(i) Current breast cancer and e(ii) Past breast cancer, respectively.
November 2020 – Table 2: additional guidance added for estradiol/nomegestrol combined oral contraceptives; Box 2: additional link to specific advice; Section 12.5: added new bullet point to direct users to discuss health risks and specific advice for travel, altitude and surgery. Added hyperlinks to relevant sections.
October 2023 – Table 3b, Table 7 and Box 2 has been updated.