Article Text

Abstract
Background Mycoplasma genitalium (Mgen) causes non-gonococcal urethritis (NGU) and is believed to cause pelvic inflammatory disease (PID). High rates of macrolide resistance are well documented globally for Mgen. In Brighton, patients with NGU and PID are tested for Mgen and test of cure (TOC) offered post-treatment.
Methods Demographic, clinical and treatment history data were collected over a 12-month period for all Mgen-positive patients in a Brighton-based genitourinary clinic.
Results There were 114 patients with Mgen. 18% (61/339) of men with NGU and 9% (15/160) of women with PID had Mgen. 62/114 (54%) returned for first test TOC 4 weeks after treatment. 27/62 (44%) had a positive TOC; 25/27 (92.6%) had received azithromycin first line (500 mg stat then 250 mg OD for 4 days), 1/27 (3.7%) had received moxifloxacin first line (400 mg OD for 14 days) and 1/27 (3.7%) had received doxycycline first line (100 mg BD for 7 days). 20/27 (74%) returned for a second TOC 4 weeks later. 5/20 (25%) patients were positive on second TOC; 3/5 (60%) had received azithromycin second line and 2/5 (40%) had received moxifloxacin second line. Patients were more likely to have a positive TOC if they were at risk of reinfection (9/27 positive TOC vs 3/35 negative TOC; p=0.02). Patients given moxifloxacin were more likely to have a negative TOC (1/27 positive TOC vs 9/35 negative TOC; p=0.03) than those who received other antibiotic regimens.
Conclusions Treatment failure rates for Mgen following azithromycin use are substantial, raising concerns regarding resistance. However, reinfection risk may contribute, suggesting a requirement for improved public awareness and clinician knowledge.
- genitourinary medicine
- sexually transmitted infections
Statistics from Altmetric.com
Key messages
Mycoplasma genitalium (Mgen) was positive in 18% of non-gonococcal urethritis and 9% of pelvic inflammatory disease cases. These patients should be tested for Mgen at initial presentation.
Treatment failure rates following azithromycin use are high, raising concerns regarding macrolide resistance. Resistance-guided treatment will help to reduce rates of treatment failure.
Many patients were at risk of reinfection, suggesting that public awareness and clinician knowledge of Mgen needs to be improved.
Introduction
Mycoplasma genitalium (Mgen) is undisputedly a cause of non-gonococcal urethritis (NGU), accounting for 10%–20% of diagnoses,1 and there is now good evidence that Mgen is a cause of pelvic inflammatory disease (PID).2–6 The newly published British Association for Sexual Health and HIV (BASHH) guidelines recommend testing in all men with NGU and women with suspected PID.2
Until recently, a limited number of commercially available assays were available and lacked thorough validation. Testing was otherwise only available through a reference service using in-house polymerase chain reaction (PCR) if NGU was unresponsive to therapy. However, newer assays are now available and in clinical use. Interest in testing is increasing given the concerns around rising macrolide resistance in Mgen worldwide. Rates of resistance are currently 40%–100%, depending on a country’s prior use of azithromycin to treat chlamydia and NGU.7–10 Epidemiological data from the UK are lacking, but some small studies have shown rates of macrolide resistance among Mgen isolates to be around 41%–78%.11–13 These studies are in men with urethritis attending London genitourinary medicine (GUM) clinics and patients with NGU or PID in a Brighton GUM clinic. Mgen develops resistance easily, requiring only a single point mutation at positions 2058 or 2059 of the 23S rRNA gene to develop macrolide resistance. Rising levels of drug resistance have resulted from transmitted resistance but mainly due to overuse of single-dose azithromycin in the treatment of NGU and chlamydia.14 Patients infected with a resistant organism may see improvement in their symptoms despite not clearing the infection completely, and pose a risk of transmission to sexual partners. National guidance therefore recommends test of cure 5 weeks after initiating treatment to ensure eradication of infection.2
We evaluated the clinical pathway for Mgen testing in our Brighton-based GUM clinic. We aimed to determine the prevalence of Mgen among patients with NGU and PID, to examine treatment histories of patients with Mgen, and to measure rates of microbiological clearance by test of cure (TOC).
Methodology
Patients with a diagnosis of NGU or PID were tested for Mgen using the Fast Track Diagnostics Urethritis Basic Multiplex PCR. This assay also detects Chlamydia trachomatis and Neisseria gonorrhoea. This was the only assay used within our clinic for Mgen detection and local validation of the assay comparing it to the Hologics test displayed a 98% concordance.15
Routine testing for Mgen in patients with NGU and PID has been performed in our clinic since October 2015. The period of data collection took place before publication of the BASHH guidelines and before macrolide resistance testing was available in the UK.
The local protocol at the time of the study advised that at the initial appointment, patients with NGU should be given 100 mg doxycycline twice a day (BD) for 7 days. Patients with PID should be given ofloxacin 400 mg BD for 14 days and metronidazole 400 mg BD for 5 days. All patients diagnosed with NGU or PID were tested for Mgen at initial presentation. Patients with positive Mgen results were then recalled for further treatment with azithromycin 500 mg immediately (stat) followed by 250 mg once a day (OD) for 4 days and invited for TOC 4 weeks after treatment. Those testing positive for Mgen on TOC should then be re-treated with moxifloxacin 400 mg orally OD for 10 days and TOC repeated after 4 weeks. Current and recent partners of index patients with Mgen were invited for testing and treatment of Mgen.
Results reporting systems and electronic patient records were interrogated for data from all patients diagnosed with Mgen from 1 December 2015 to 30 November 2016. Demographic information was collected on gender, age, ethnicity, sexuality, and HIV status. Consultations were reviewed to gather data on symptoms, if they were a known contact of Mgen, reinfection risk, number of contacts in the last 3 months, concurrent sexually transmitted infection (STI), treatments given and Mgen results. Reinfection risk was defined as sex while on treatment (or the first 7 days if the treatment course was less than 7 days) or ongoing sex with an untreated partner following treatment.
Diagnoses for NGU, PID, Mgen, chlamydia and gonorrhoea were based on GUMCAD coding. Microscopy data were not collected but the clinic uses >5 polymorphonuclear lymphocytes/high-powered field on Gram-stain as the minimum required for a diagnosis of urethritis. Patients were included as having NGU if they were symptomatic with a NGU code. In addition, to account for possible inadequate coding by staff, patients with a documented urethral discharge with or without dysuria were also included as NGU patients. PID was considered a clinical diagnosis and was defined as sexually active women presenting with pelvic pain and having tenderness on bimanual examination when other causes had been excluded such as pregnancy or urinary infection. All women coded for PID had symptoms consistent with PID.
Bivariate analysis for differences between patients that remained positive for Mgen on TOC (TOC-positive) and patients that cleared Mgen following treatment (TOC-negative) were performed using Fisher’s exact test (threshold p<0.05). This was calculated using 2×2 contingency table calculators for Fisher’s exact test using two-tailed p values (QuickCalcs, www.graphpad.com). This analysis was also used to compare patients that attended for TOC and those that were lost to follow-up.
Ethical approval was deemed unnecessary as this was an evaluation of anonymised data using an established clinical pathway with a previously evaluated assay.
Patient and public involvement
Due to the nature of the study, participants were not involved in the design, conduct or reporting of this study.
Results
Patient demographics
Over a 12-month period, 115 patients were diagnosed with Mgen. One patient was excluded due to lack of available clinical information, so the analysis was based on the 114 remaining patients. Of these patients, 72% were male (46/82 heterosexual, 36/82 men who have sex with men (MSM)) and 80% self-identified as white British. The median age was 27 (range 16–63) years. Eight (7%) patients were living with HIV, all of whom were male. Sixteen (14%) patients were chlamydia-positive and five (4%) were gonorrhoea-positive.
Reasons for Mgen testing
91/114 (80%) of patients with Mgen had been tested, as they were symptomatic: 15 women with PID and 61 men with NGU. An additional two patients were tested due to epididymitis, one for proctitis and five for dysuria and/or ejaculatory pain. Seven symptomatic women were tested for reasons outside local guidelines for Mgen testing such as dysuria, altered vaginal discharge, altered bleeding, and dyspareunia or abdominal pain not attributed by the clinician as being caused by PID. These patients were all included in the data analysis.
Twenty-three patients were tested for other reasons: 16 were contacts of Mgen (three with symptoms), five were contacts of other infections (two PID, two gonorrhoea and one chlamydia) and two patients were tested for unknown reasons.
Prevalence of Mgen
18% (61/339) of men with NGU had Mgen and 39% (24/61) of these patients were MSM. 9% (15/160) of women diagnosed with PID tested positive for Mgen.
Management at first presentation
Figure 1 shows the patients tested and treated for Mgen. Ninety-two (81%) of the 114 patients with a positive Mgen result were given treatment at their initial presentation before their Mgen test result was known. Fifty-four patients were given doxycycline and 10 were given ofloxacin and metronidazole. Table 1 displays the treatments given at first presentation, subsequent first-line treatments for Mgen once the Mgen result was known and then results of the TOC.

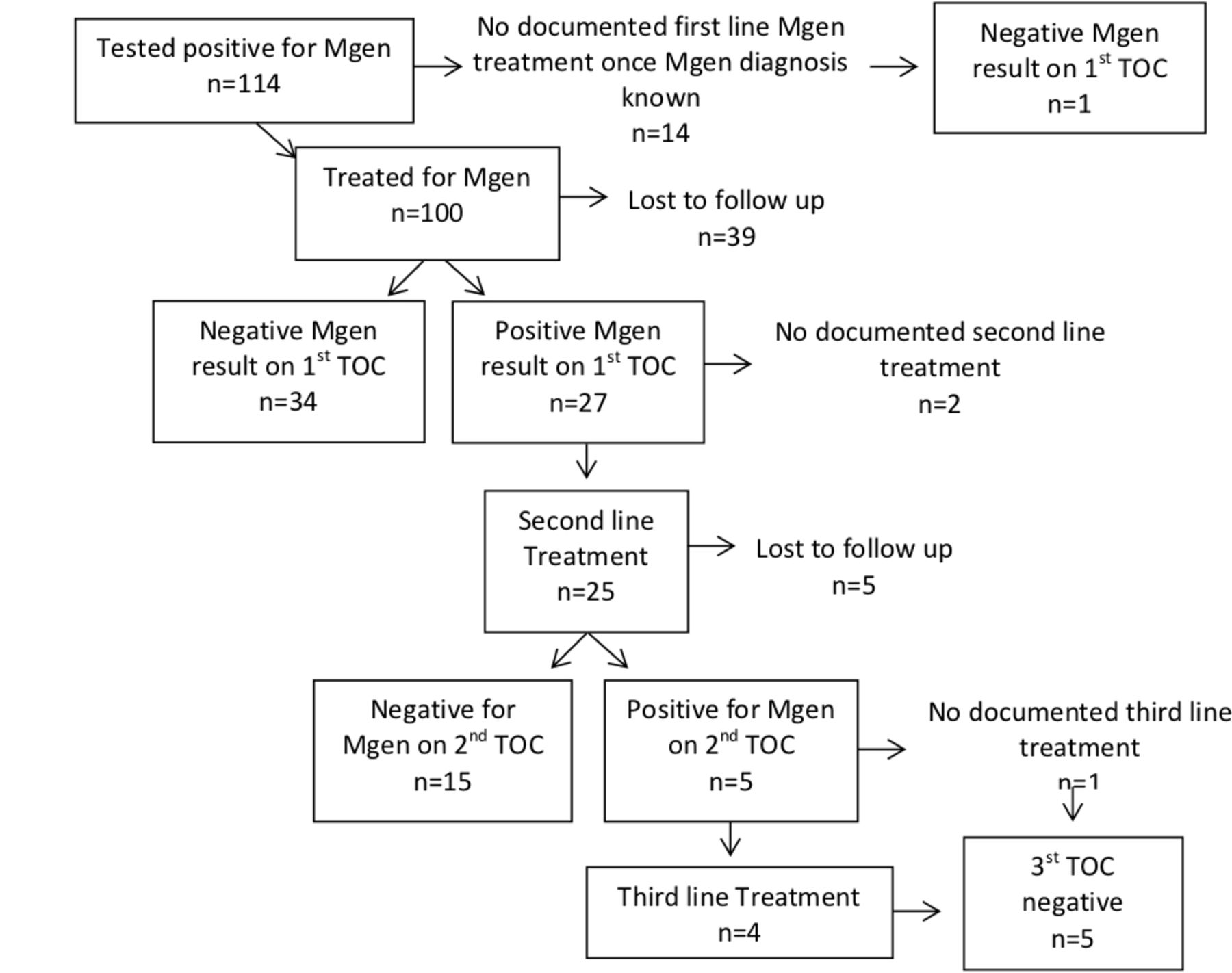{kind=link}
Patients tested and treated for Mycoplasma genitalium (Mgen). TOC, test of cure.
Treatment at first presentation, Mycoplasma genitalium (Mgen) first-line treatment once Mgen result known and test of cure results
Management following Mgen diagnosis
Treatment failure following first-line antibiotic treatment for Mgen once Mgen result known
83/114 (73%) patients were treated with azithromycin regimens first line (Table 1). Two (2%) were treated with doxycycline, 14 (12%) with moxifloxacin and one (1%) with ofloxacin. 14/114 (12%) patients did not receive further treatment for Mgen following a positive Mgen result. 62/114 (54%) patients diagnosed with Mgen returned for a TOC. 27/62 (44%) patients had a positive TOC: 25/27 had been given azithromycin, 1/27 had been given moxifloxacin and 1/27 had been given doxycycline.
Treatment failure following second-line antibiotic treatment for Mgen once Mgen result known
Of the 27 patients with a positive TOC, five (19%) were given azithromycin 500 mg stat followed by 250 mg OD for 4 days for a second time, 20 (74%) were given moxifloxacin and two (7%) did not receive further treatment. 20/27 (74%) of these patients returned for a second TOC. 5/20 (25%) patients tested positive (three had been given azithromycin, two had been given moxifloxacin).
Third-line antibiotic treatment for Mgen once Mgen result known
Three patients were given moxifloxacin and one patient with confirmed resistance to macrolide and quinolone therapy was given a 10-day course of pristinamycin 1 g four times a day and doxycycline 100 mg twice a day. As we did not have access to resistance testing this patient had their sample sent to a laboratory in Denmark for sequencing as they had persistent symptoms with a positive TOC. One patient failed to attend follow-up but subsequently tested negative 6 months later. All patients were negative on third TOC. Table 2 shows a summary of treatments given once the Mgen result was known.
Summary of Mycoplasma genitalium (Mgen) antibiotic treatment regimens once the Mgen result was known
Lost to follow-up
There were high numbers of patients lost to follow-up (figure 1). 54% (62/114) patients returned for a TOC (35 negative and 27 positive). 46% (52/114) were lost to follow-up and had no TOC. The median age was slightly older in the people that attended for TOC (age 28, range 16–63, years) in comparison to those that did not attend TOC (age 25, range 16–62, years). There was no evidence of difference for gender, sexuality, ethnicity or HIV status between those that attended for TOC and those that were lost to follow-up (p=0.21, p=0.43, p=0.49, p=0.73, respectively).
Positive TOC verses negative TOC
Patients were more likely to have a positive TOC if they remained symptomatic (p<0.001), had two or more partners (p=0.002) or were at risk of reinfection (p=0.02). Patients whom were given moxifloxacin either first line or at initial presentation were more likely to have a negative TOC (p=0.03). There was no evidence of difference between those that had a positive and negative TOC for sexual orientation, gender, HIV status, concurrent STIs at the time of first presentation when the Mgen test was performed (chlamydia, gonorrhoea or herpes), or any azithromycin use at first presentation (when Mgen test performed) or as first-line therapy once the Mgen result was known. Table 3 shows associations between positive and negative Mgen results on TOC.
Positive verses negative Mycoplasma genitalium (Mgen) results on test of cure
Discussion
Levels of Mgen in NGU and PID were high but comparable to recognised national chlamydia levels and much higher than gonorrhoea levels in NGU and PID.16 17 In addition, our observed Mgen prevalences in those with NGU and PID are within the region noted by the BASHH 2018 Mgen guidelines.2 Our unit was one of the first units to test for Mgen in the UK and this study adds to the body of international data by providing evidence of clinical treatment failures in a UK-based setting.
High treatment failure rates were observed, especially following azithromycin use. Although reinfection may contribute, these results are also consistent with global and national rates of macrolide resistance.7–11 This could be because individuals either had macrolide-resistant Mgen at baseline or developed resistance following repeated macrolide treatment. Given the ease with which azithromycin induces resistance mutations in Mgen, repeat regimens of this drug should not be used, as the risk of treatment failure is too high.2 18 It was reassuring that microbiological clearance following moxifloxacin was good and the fourth-generation quinolones are still reported as being very efficacious in eradicating Mgen in Europe.19 In addition, the use of ofloxacin and metronidazole treatment for PID followed by azithromycin, once there was a known positive Mgen result, did not show any positive TOC. That said, ofloxacin has a much higher minimum inhibitory concentration for Mgen and should not be used first line in the treatment of Mgen PID.20 Cases of dual macrolide and quinolone resistance are emerging in the UK, and the true extent of quinolone resistance will only become apparent when routine detection and resistance testing is available.21
It is possible that TOC was performed too soon and that Mgen had not yet fully cleared. Few data exist to inform the optimal time to conduct TOC. Current limited evidence suggests that performing a TOC sooner than 3 weeks after treatment can generate false-negative results, because of the initial fall but then rise in organism load following the development of macrolide resistance mutations.22
One of the limitations of the study are that return rates for Mgen TOC were poor; however, we have observed similar return rates for gonorrhoea TOC at our clinic. This could possibly be explained by patients experiencing an initial improvement in symptoms and opting not to return for repeat testing. As many male patients had doxycycline prior to their Mgen diagnosis, which will fully eradicate Mgen in only 30% of cases,23 it is possible that some experienced a fall in organism load, corresponding with clinical improvement, but without full clearance of the organism. This study did not collect data on adherence to the medication or side effects, which may have had an impact on treatment failures. Newer methods such as mobile text reminders and online postal STI testing kits may help to overcome some of the barriers to returning to clinic for repeat testing.24 25
Another limitation of the study is that it was performed in a Brighton sexual health clinic. There is a higher proportion of MSM in comparison to some clinics,26 therefore the results may be less applicable to centres that serve different populations. However, the proportion of treatment failures seen are consistent with other studies.11 27
Mgen treatment failure following azithromycin is primarily related to macrolide resistance.18 In our study, 26/27 patients with positive TOC received azithromycin. Those patients who experienced treatment failure attended clinic multiple times and many took more than one course of antibiotics following positive TOC. A recent study in Australia has shown that the proportion of treatment failures can be significantly reduced through implementation of an assay that concurrently detects macrolide resistance mutations and the organism.28 These assays are now commercially available and the 2018 Mgen BASHH guidelines advise that all Mgen-positive samples should be tested for macrolide resistance.2 During the study period the UK did not have access to these assays. Testing for resistance at baseline would improve antibiotic stewardship by avoiding unnecessary antibiotics and lessening induced resistance. It would also improve patient experience and reduce the need for repeat clinic attendances, testing and treatment.
Fourteen patients had reasons for testing that did not follow local clinic guidelines, for example, women with vaginal discharge only and asymptomatic contacts of non-Mgen infections. Given that Mgen is unlikely to cause disease in the vast majority of infections, screening those without specific STI syndromes such as NGU and PID is not beneficial.29 30
In summary, Mgen is believed to cause significant morbidity, is difficult to treat and represents a real threat to the wider public health in terms of antibiotic resistance. There is an urgent need for availability and affordability of smarter diagnostic assays that have the ability to detect the presence of Mgen and resistance concurrently. As many patients were at risk of reinfection, resources to educate the public about this infection are also required. The recent publication of national guidance will help clinicians to manage this multidrug-resistant organism.2
References
Footnotes
Twitter @doctorjjrw
Contributors KJO and SS were involved in all stages of the study and KJO wrote the first and final draft of manuscript. JJRW participated in study design and data collection. ELAC was involved in the study design, data collection and analysis. LR participated in data collection. MOHI did laboratory work. All authors reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.