Article Text

Abstract
Background Contraceptive and sexual healthcare is increasingly delivered in an integrated setting in the UK and worldwide, requiring staff to be competent in differing styles of delivery, and to have a wide knowledge base.
Objectives We did a scoping review of the literature for evidence of the resources that exist for healthcare professionals to guide or structure the process of conducting an integrated sexual and reproductive health (SRH) consultation.
Eligibility criteria Articles were included in the review if (1) their primary focus was a consultation resource related to one or more aspects of an SRH consultation and (2) they provided details of the resource and/or its application including evaluation of use.
Sources of evidence Peer-reviewed articles published in English, published non-peer-reviewed guides, and web-based guidelines addressing the conduct of a contraception or sexual health consultation were included. Date range: 1998–December 2018. Searches were carried out in the databases AMED (Ovid), ASSIA (ProQuest), CINAHL Complete (EBSCO), Cochrane Library (Wiley), HMIC (NHS Evidence), Medline (EBSCO), PsycINFO (Proquest) and Scopus (Elsevier) on 10 February 2017, and incremental searching performed until December 2018.
Results A total of 12 peer-reviewed journal articles, two web-published guidelines from the Faculty of Sexual & Reproductive Healthcare and three published, non-peer-reviewed resources were included.
Conclusion Many resources exist to guide either the contraceptive or sexual health consultations, but there is a lack of a comprehensive consultation resource to guide the conduct of an integrated consultation.
- education and training
- family planning service provision
- genitourinary medicine
- service delivery
- integrated services
- consultation process
Statistics from Altmetric.com
- education and training
- family planning service provision
- genitourinary medicine
- service delivery
- integrated services
- consultation process
Key messages
Integrated sexual and reproductive health (SRH) services can present difficulties for staff because of the differing styles of consultation and knowledge bases required.
Various resources exist to guide contraceptive and sexual health consultations but few are designed to guide an integrated consultation, except for those with adolescent clients.
A comprehensive, user-friendly framework or model to guide staff who are a new to conducting an integrated SRH consultation is needed.
Additional educational resources
WHO Decision Making Tool
https://www.who.int/reproductivehealth/publications/family_planning/9241593229index/en/
Birth Control Navigator
My Contraception Tool (Brook)
https://www.brook.org.uk/our-services/category/my-contraception-tool
My Birth Control
Calgary-Cambridge Framework for Consultations
Kurtz SM, Silverman JD, Benson J, Draper J (2003). Marrying content and process in clinical method teaching: enhancing the Calgary-Cambridge Guides. Academic Medicine 2003; 78:802–9.
Kurtz SM, Silverman JD, Draper J (1998). Teaching and Learning Communication Skills in Medicine. Radcliffe Medical Press, Oxford, UK.
Silverman JD, Kurtz SM, Draper J (1998). Skills for Communicating with Patients. Radcliffe Medical Press, Oxford, UK.
Rationale
Integrated sexual and reproductive health (SRH) services were endorsed globally at the 1994 International Conference on Population and Development in Cairo. Integrated provision is reflected in recent policy in England, the USA and across Europe1–4 because it better meets service users’ needs by providing holistic services,2 improves access and opportunities for early intervention, diagnostics and screening, and is cost effective.1 We have chosen the term ‘integrated sexual and reproductive services’ to describe a holistic, comprehensive service, throughout the life-course, but we recognise the controversy about this terminology and how such services should be provided. French et al provides a summary of the debate.5
National commissioning guidance in England indicates that integrated services should be provided as a 'one-stop shop', with majority of sexual and contraceptive needs addressed by a health professional in a single SRH consultation.1 A key challenge is the extent to which staff are competent and equipped to work in roles which are broader than those for which they were trained.6–8 Boog et al report that where clinicians are required to address multiple issues in a single SRH consultation but lack the necessary skills, this has resulted in prolonged consultations and increased waiting times.9
A range of types of resources exist to support clinical consultations. Clinical guidelines provide evidence-linked task-focused recommendations for clinical practice, while tools are specific aids, used to address one aspect of the consultation. Toolkits provide practical guidance and support for consultations while frameworks offer a theoretically derived or practical structure within which services are delivered. Consultation models provide memory maps of consultation process and content and their use is well established in general practice where they are widely used, particularly as an educational tool to support novice practitioners.10–14
Objectives
We hypothesised that consultation models and other resources may help staff to deliver integrated consultations in one-stop SRH services, and set out to identify what was currently available and to critically appraise their contribution specifically to an integrated consultation. Our research question was formulated as ‘What resources exist for healthcare professionals to guide or structure the process of conducting an integrated sexual and reproductive health consultation?’.
Methods
A scoping review is characterised as a broad-based assessment, designed to map a body of literature and provide an overview of the existing heterogenous evidence on a specific topic.15 16 Our review was guided by the framework described by Arksey and O’Malley.17
Search strategy
Searches were carried out in the databases AMED (Ovid), ASSIA (ProQuest), CINAHL Complete (EBSCO), Cochrane Library (Wiley), HMIC (NHS Evidence), Medline (EBSCO), PsycINFO (Proquest) and Scopus (Elsevier) on 10 February 2017. Title/abstract words and database subject headings relating to consultation models, frameworks, guidelines and tools were combined with title/abstract words and database subject headings relating to SRH. Date restrictions were 1998 to February 2017 to reflect a 20-year window prior to our searches and following the 1994 Cairo statement committing to comprehensive and inclusive reproductive healthcare. We hand searched a number of key websites (online supplementary file 1) and conducted incremental searches, based on the included articles, both at the beginning of the review process and part-way through, to ensure we included articles published during the review process.
Supplemental material
Selecting and reviewing evidence
We used two screening questions to determine relevance: (1) Is the primary focus a consultation resource related to one or more aspects of an SRH consultation? and (2) Are details of the resource and/or its application including evaluation of use provided? We excluded guidelines if they were purely clinical in nature, rather than addressing the consultation as an event (eg, method-specific guidelines for contraception, and clinical guidelines on the treatment of specific sexually transmitted infections (STIs)). We also excluded SRH resources addressing the context of specific conditions (eg, breast cancer) or which addressed psychosexual dysfunction.
At each stage of review, the findings and process of the previous stage were discussed, and the reasons for including and excluding resources agreed on, in keeping with a scoping review process. This allowed an agreed approach to the next stage of review, and these iterations refined our selection, informed by our increasing familiarity with the available literature. Five reviewers carried out the review of titles, the first screening of abstracts, and the second double-handed review of abstracts (HP, SW, KS, FA, LH). Any disagreements between the two reviewers were discussed and resolved. The final full-text reviews were carried out by four reviewers (HP, SW, FA, KS).
Search outcome
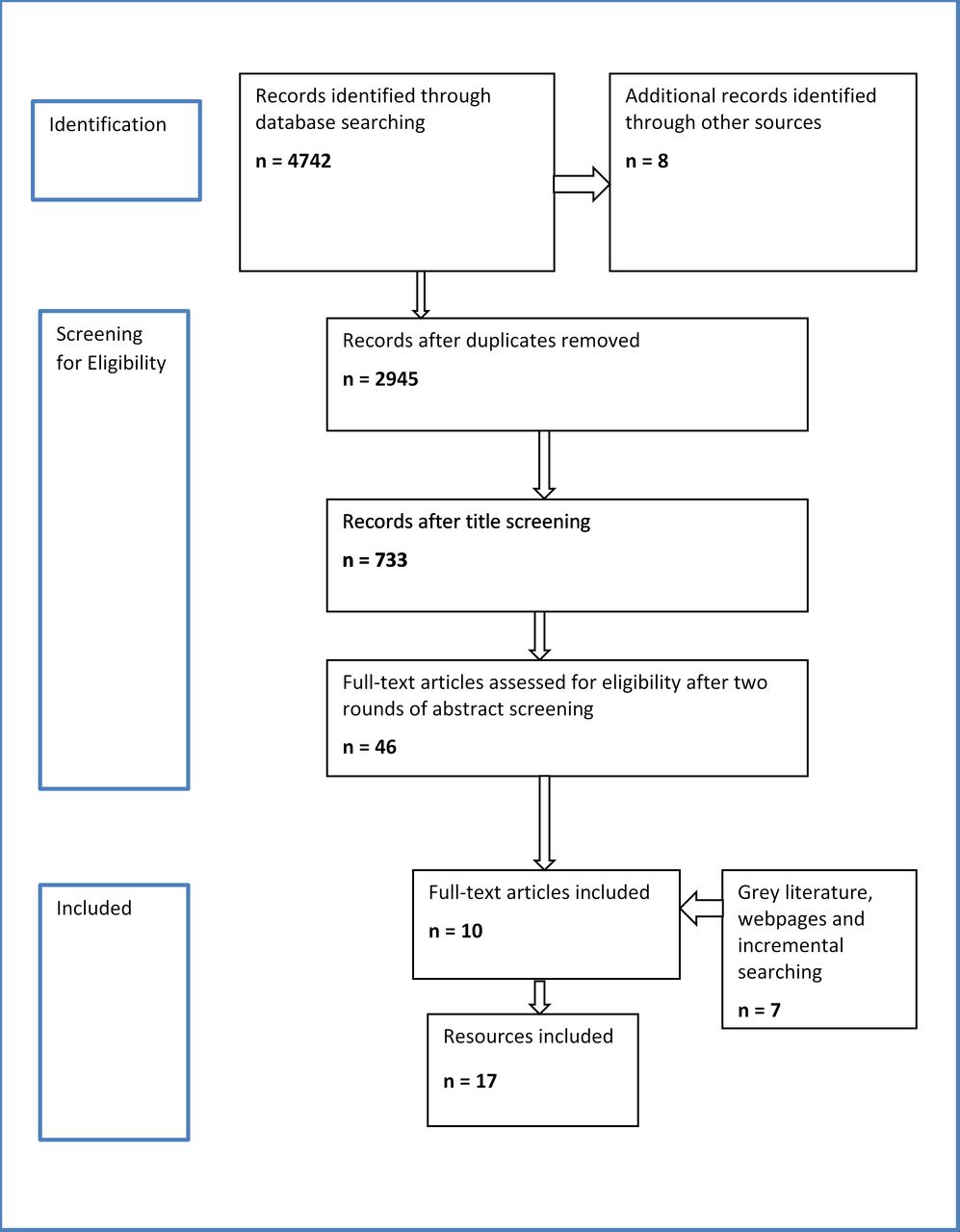
Our original searches resulted in 4742 ‘hits’ to which a further eight identified from other sources were added (figure 1). Some 1805 duplicates were removed resulting in 2945 titles. Screening of titles produced 733 relevant journal articles, dissertations and book chapters. Book chapters were removed, but foreign language resources with English abstracts were retained. Two rounds of abstract screening resulted in 46 resources in English, and a further 30 non-English resources. We excluded the non-English full texts, and also removed texts that primarily discussed sexual dysfunction. Screening of 46 full-text resources resulted in 10 resources from the original database search which met our agreed criteria. These were supplemented with a further two recently published articles identified through incremental searching. Three non-peer-reviewed published resources and two published guidance sources from the Faculty of Sexual & Reproductive Healthare (FSRH) website were included as they also met our criteria. Of these 17 resources, seven were from the UK, six the USA, one European, two global and one from Mexico.
{kind=link}
PRISMA diagram illustrating the literature screening process.
The evidence was extracted (1) identifying the content of the resource and (2) reporting any existing evaluation of its use. It was synthesised in a narrative style.17
The resources are descriptively summarised in the data extraction table (table 1).
Data extraction table
Results
We identified limited resources specifically developed to support an integrated SRH consultation, appropriate for users across the life-course. We found no consultation models designed for guiding the process of an integrated SRH consultation. We did, however, identify a number of tools, toolkits, frameworks and guidelines that have been designed for discrete aspects of sexual or reproductive/contraceptive health consultations, some of which have been adapted to include other aspects of SRH. In addition, we found several resources developed specifically to support SRH consultations with young people.
Tools
We identified five tools designed to improve consultations. Four are contraceptive decision-making tools while the fifth, an event history calendar tool, was designed to identify sexual risk.
Contraceptive decision-making tools
Four decision-making tools to support contraceptive consultations were found. The first of these is the WHO Decision-Making Tool (https://www.who.int/reproductivehealth/publications/family_planning/9241593229index/en)18 developed for global use and adaptable to individual countries. It is a double-sided, flip-chart-based tool, designed to be used within a consultation. One page faces the client (with simple information on key issues for the client to consider) and a corresponding page faces the provider (with key points and detailed reference information). This design indicates that it has been developed for use in resource-limited countries rather than specialist contraceptive services. Its use has been evaluated in Indonesia, Mexico and Nicaragua, and indicated that it improved providers' counselling behaviours, providing clients with information tailored to their needs, and it engaged clients more in decision making.19 20
‘My Birth Control’ (MBC) (https://clinic.mybirthcontrol.org/),21 ‘Birth Control Navigator’ (BCN) (https://mydoctor.kaiserpermanente.org/ncal/birthcontrol/)22 and ‘My Contraception Tool’ (MCT) (https://www.brook.org.uk/our-services/category/my-contraception-tool)23 are all web-based decision aids. The first two were developed in the USA and the third in the UK. They are intended to be used by women prior to a contraceptive consultation. Their purpose it to support effective contraceptive consultations by making the decision-making process transparent to the user and suggesting methods based on their own preferences.
Some pilot testing of MBC was undertaken as part of the development process. Using the tablet-based MBC decision aid prior to consultation, and then sharing the printout with the provider, was associated with greater client satisfaction, and most of the 41 women using it (96%) reported that it helped them choose a method.21
The BCN was developed by an integrated healthcare delivery service in California. There are no published reports of its usage although a small study, involving 21 women aged 18–29 years who were current users of that service, was conducted to assess the tool in terms of its perceived value for contraceptive decision making.22 The findings indicate the women valued the information content and reported that it would be useful in terms of narrowing options, and knowing what questions to ask when seeing a doctor.
MCT is a freely available web-based tool. The MCT tool is now accessible on the websites of two contraceptive and family planning organisation websites in the UK (Brook and FPA), where it allows users to narrow down their contraceptive choices, according to their expressed preferences and priorities. We found no evidence of its evaluation in the UK where it was developed but one small, unpublished project conducted in the USA reported some improvement in contraceptive continuation rates and follow-up appointment rates.24
Event history calendar tool
This tool was developed to be used with young people. Its purpose is to improve recall, report and discussion of sexual risk pattern behaviours in the context of the adolescent's life events, relationships and other risk behaviours.25 The tool is designed to be completed by the client immediately prior to consultation and then discussed with the healthcare professional within the consultation. It consists of a grid with four vertical time columns labelled with four sequential years across the top of the page. Down the left side of the page are nine horizontal history categories that ask about (a) life context, including age, grade level, friends and family members involved in the adolescent’s life, activities, and positive events (eg, awards) and negative events (eg, losses and violence), (b) sexual risk behaviours and (c) other risk behaviours (eg, drugs, alcohol and cigarette use). A mixed-method study of its use with males and females aged 15–19 years indicated that it facilitated communication and adolescent awareness of their sexual risk behaviours.26 Feasibility of the tool was assessed with the same group of adolescents and indicated it was acceptable to users and resulted in a more complete sexual risk history disclosure.26
Toolkits
We identified two toolkits, both developed in relation to young people's sexual health services. The first of these, ‘Sexual Health: An Adolescent Provider Toolkit’27 is a comprehensive document covering a wide range of aspects related to sexual health. Developed in the USA, it has sections on Practice Readiness (covering communication, consent, and adolescent development), Screening, Assessment and Referrals (covering STIs, pregnancy, sexual assault, sexual violence and sexual dysfunction) and Resources for Providers (giving information on types of contraception, sexual function and pleasure, and specific sections on safer sex, human papillomavirus (HPV) and paternity rights). It includes a sexual history taking template with suggested listed questions, and tips on communication style and relevant issues. The toolkit also provides guidance and handouts for young people, and guidance for parents.
The second, ‘Spotting the Signs: A National Toolkit',28 has a specific focus. It was developed to help health professionals identify young people at risk of child sexual exploitation and supports use of the ‘Spotting the Signs’ proforma’.29 The toolkit includes advice on confidentiality, epidemiology and law, and provides a template for areas to cover in history taking with a young person. It also gives some advice on what language to use and how to ask questions, as well as what to ask.
Frameworks
We identified two frameworks, both developed for contraceptive services. The 'Quality in Contraceptive Counselling Framework' is a theoretical framework developed by Holt et al.30 It focuses on the individual experience and synthesises concepts from family planning, broader healthcare and health communication, together with concepts from human rights guidance. Their framework covers the three stages of consultation: (1) Needs Assessment, (2) Decision-making Support and (3) Method Choice and Follow-up (1). There is emphasis on 'shared decision making' rather than pure ‘informed choice' and it includes ‘Foundational Relationship Building’ elements (Privacy, Confidentiality, Non-discrimination, Respect, Empathy, Trust) as underpinning concepts.
The FRSH 'Service Standards for Consultations in Sexual and Reproductive Health'31 is a practical, framework document. It provides quality standards for the consultation which include standards for confidentiality, the clinical environment (privacy and dignity), verbal and non-verbal communication skills, use of a chaperone, needs of special groups (including safeguarding) and child sexual exploitation.
Clinical guidelines
We identified four sets of clinical guidelines which provide guidance on clinical consultations, two non-age-specific and two relating specifically to consultations with adolescents and children.
The ‘2013 UK National Guideline for Consultations Requiring Sexual History Taking32 is similar to but has a wider remit than the ‘European Guideline for the Organisation of a Consultation for Sexually Transmitted Infections, 2012’,33 having been extended in 2014 specifically to incorporate a section on contraception and a range of other SRH aspects, in light of policy recommendations for integrated consultation. Its stated purpose is to "describe best practice for establishing the facts on which clinical decision making is based". It covers the components of a sexual history, then those of a contraceptive and reproductive health history, and finally aspects of history taking likely to be particularly important in an integrated contraception. As such, this document offers one of the most comprehensive resources in terms of coverage of the different aspects of SRH. However, while it does cover communication skills required for sexual history taking, it does not identify what consultation skills are required for an integrated SRH consultation.
The FSRH 'Clinical Guidance on Contraceptive Choices for Young People'34 provides guidance on legal and ethical frameworks, confidentiality and consent, addressing young people’s health concerns, risks regarding various contraceptive methods, and use of condoms to prevent STI transmission and STI testing. Brief guidance is also given on the conduct of the consultation process with regard to informing young people about confidentiality, creating a welcoming environment and avoiding barriers to communication.
The ‘United Kingdom National Guideline on the Management of Sexually Transmitted Infections and Related Conditions in Children and Young People’35 emphasises the detection and management of child sexual abuse (CSA). Other sections cover only briefly additional aspects of sexual history taking in young people, often simply signposting to other guidance, for example, National Institute for Health and Care Excellence (NICE) guidelines on the 'Prevention of STIs and Under 18 Conceptions'.
The guideline covers consent, confidentiality and child protection, the content of sexual history, screening and testing for STIs and, more briefly, risk assessment for pregnancy, contraceptive advice, health education/promotion, psychological well-being and management of specific groups.
Limitations
This scoping review was limited to papers published in English post-1998.
Discussion
In summary, a diverse range of resources exist to support SRH health consultations which can be broadly categorised in two groups: those specific to young people's sexual health services and those which are not age-specific. The group of resources specific to young people are most comprehensive in terms of both the types of resources and the nature of those resources. Tools, toolkits and guidelines all exist for young people's services. They are wide ranging in terms of coverage, and a key focus in all of them is on identification and reduction of risk and harm reduction.
Most of the non-age-specific resources are decision tools, developed to support contraceptive consultations by improving clients' contraceptive decision making. These tools reflect the preference-sensitive nature of a contraceptive consultation and the evidence that indicates women view decision making about contraception differently from that for general health, with a stronger preference for making their own choice about treatment and/or using shared decision-making processes to reach that choice.30 36–38 In contrast, two sets of guidelines developed to support an STI consultation follow a physican-led, diagnosis-focused medical style of consultation.32 33
These resources highlight the potential complexity of an SRH consultation which we suggest accounts in part for the problems that Boog et al reported.9 The effectiveness of an integrated SRH consultation relies not only on the ability of the clinician to address multiple issues within a single consultation, but also to change consultation style. While a medical model of consultation is likely to be most appropriate for effectively identifying and managing STIs and wider sexual health risks, a body of evidence indicates the importance of using a different model for contraceptive consultation. A shared decision model approach is widely acceptable to women39 40 and results in greater satisfaction with the contraceptive decision, than where decisions had been made either solely by the client or solely by the provider.30
Incorporating the use of a contraceptive decision tool within integrated SRH services could be helpful in terms of improving client involvement and addressing some of the problems reported by Boog et al.9 Dehlendorf et al suggested that their tool (MBC) can help with the time constraints of a shared decision-making consultation.21
The existing resources do not recognise or provide support for the need to be able to apply different consultation models within a single integrated SRH consultation. We suggest there is a need to better understand what happens in an integrated consultation in terms of whether clinicians can and do move between different models and what resources would be helpful to support this process.
Conclusions
We found no consultation model designed for guiding the process of an integrated consultation, in an integrated service providing both contraceptive care and sexual healthcare to all age groups. In view of the reported problems experienced by staff in integrated services, we feel that such a consultation model would help staff transitioning from a single to an integrated service. It has the potential to drive up the quality and patient-centredness of such consultations, and act as an educational resource for new staff. We intend to undertake the development of such a resource with the involvement of patients, staff and educators.
Acknowledgments
Mel Gee, information scientist, oversaw the search strategy and conducted the searches for this review. The authors are grateful to Dr Lesley Hoggart who assisted in the initial screening process.
References
Footnotes
Twitter @susanwalker67
Contributors SW, HP and KS conceived the review. Mel Gee advised on and carried out the literature searching. Dr Lesley Hoggart participated in the screening of titles and abstracts. Mel Gee, SW, HP, Dr Lesley Hoggart and FA participated in planning the review and the screening process. SW, HP, KS and FA contributed to the analysis and interpretation of the data and to the writing of the manuscript.
Funding This literature review was funded by an internal grant from Anglia Ruskin University.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.