Article Text

Abstract
Introduction Postpartum family planning (PPFP) is critical to reduce maternal–child mortality, abortion and unintended pregnancy. As in most countries, the majority of PP women in Rwanda have an unmet need for PPFP. In particular, increasing use of the highly effective PP long-acting reversible contraceptive (LARC) methods (the intrauterine device (IUD) and implant) is a national priority. We developed a multilevel intervention to increase supply and demand for PPFP services in Kigali, Rwanda.
Methods We implemented our intervention (which included PPFP promotional counselling for clients, training for providers, and Ministry of Health stakeholder involvement) in six government health facilities from August 2017 to October 2018. While increasing knowledge and uptake of the IUD was a primary objective, all contraceptive method options were discussed and made available. Here, we report a secondary analysis of PP implant uptake and present already published data on PPIUD uptake for reference.
Results Over a 15-month implementation period, 12 068 women received PPFP educational counselling and delivered at a study facility. Of these women, 1252 chose a PP implant (10.4% uptake) and 3372 chose a PPIUD (27.9% uptake). On average providers at our intervention facilities inserted 83.5 PP implants/month and 224.8 PPIUDs/month. Prior to our intervention, 30 PP implants/month and 8 PPIUDs/month were inserted at our selected facilities. Providers reported high ease of LARC insertion, and clients reported minimal insertion anxiety and pain.
Conclusions PP implant and PPIUD uptake significantly increased after implementation of our multilevel intervention. PPFP methods were well received by clients and providers.
- counseling
- contraceptive devices
- female
- family planning services
- reproductive health services
Data availability statement
Data are available in a public, open-access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Wall, Kristin, 2018, "Replication Data for: an interim evaluation of a multi-level intervention to improve post-partum intrauterine device (PPIUD) services in Rwanda", https://doi.org/10.7910/DVN/WLZ7PC, Harvard Dataverse, V1.
Statistics from Altmetric.com
Key messages
We developed a multilevel intervention to increase postpartum (PP) family planning long-acting reversible contraceptive (LARC) method supply, demand and sustainability in Kigali, Rwanda.
Uptake of PP implant and PP intrauterine devices significantly increased pre- versus post-implementation.
Providers reported high ease of PP LARC insertion, and clients reported minimal insertion anxiety or pain.
Introduction
Postpartum family planning (PPFP) is critical to improve birth spacing which reduces maternal–child mortality, abortion, unintended pregnancy, and improves family well-being.1 2 Some 61% of PP women aged 15–49 years across 21 low- and middle-income countries, including Rwanda, have an unmet need for PPFP.3 Among the few PP women who are contracepting, almost all (79%) use short-acting contraceptive methods, with relatively few using the more effective long-acting reversible contraceptive (LARC) methods.3 In Rwanda, the most densely populated country in continental Africa, the government has made scaling-up of PPFP an objective of their Family Planning 2020 Commitment, and LARC methods are prioritised.4 5
In response to this scale-up, researchers at Projet San Francisco developed and evaluated an evidence-based, multilevel intervention with the goal of increasing supply and demand for PPFP in Kigali, Rwanda. We previously published the effect of our multilevel intervention on PP intrauterine device (IUD) uptake and service delivery outcomes with data reported between August 2017 and July 2018. Briefly, we found that 29% of women who received our PPFP counselling selected a PPIUD (a 2749% increase in PPIUD insertions comparing pre- vs post-intervention).6
Here, in a secondary analysis, we describe PP implant uptake and service delivery outcomes among women who received our PPFP counselling between August 2017 and October 2018. We present updated PPIUD data (including both the previously reported PPIUD data and additional PPIUD data reported up until October 2018) for reference.
Methods
Informed consent and ethics
The Emory University IRB and the Rwanda National Ethic Committee approved the research component of this project (IRB 00001497). Prior to enrollment, written informed consent was obtained from all participants engaging in human subjects research. The Emory University IRB determined the programmatic service delivery component of this project was exempt from review.
Intervention development and design
We previously published methods regarding development and implementation of our multilevel PPFP service delivery model targeting supply, demand creation and sustainability.6 7 Briefly, our team’s experience implementing LARC programmes in Rwanda8–10 and formative work conducted from May to August 2017 by Emory University-affiliated, non-governmental organisation Projet San Francisco with nurses, providers, clients, community health workers and government stakeholders informed the development of an educational flipchart on the PPIUD for use in group and one-on-one counselling. Counselors used the PPIUD flip chart along with flipchart materials already in use in governmnet clinic FP departments which described other FP method options. Existing materials did not discuss PPIUD, which has different insertion procedures and side effects relative to interval IUD insertion, necessitating creation of the PPIUD flipchart. We trained providers in PPIUD insertion/removal. As providers had previously been trained in implant insertion/removal, we offered refresher training as needed. We reimbursed providers at a higher rate for the IUD compared with the implant (US$1.20 for PPIUD insertion vs US$0.62 for PP implant insertion) because of the additional training and certification required before providing PPIUDs to clients as has been described.11 Finally, we engaged Ministry of Health stakeholders at the outset and throughout the implementation.
Promoting PPFP
The PPIUD flipchart was administered in addition to standard FP counselling materials in two health centres and two high-volume hospitals including their affiliated health centres (six facilities in total). All PP contraceptive method options were discussed and made available. Notably, FP counselling is not systematically provided in Rwandan antenatal care (ANC), labour and delivery (L&D) and infant vaccination services, but rather women are referred to separate FP services. Therefore, our programme made efforts to increase uptake of all PPFP methods by integrating counselling into ANC, L&D and infant vaccination services. Study nurses and other trained staff delivered educational promotions on all PPFP methods to expectant mothers and new mothers (≤6 weeks PP) during their FP counselling sessions in ANC, L&D and the PP ward, and/or during infant vaccination appointments occurring within 6 weeks of delivery. In L&D wards in Kigali, we counselled women not yet in active labour in the L&D waiting room (women in active labour are moved to L&D beds and were not counselled). Study nurses delivered educational promotions about the entire contraceptive method mix in group settings first (20 min). Then, they held one-on-one promotions with any women from the group sessions who were interested in more information about any PPFP method (an additional 20 min of counselling including time for questions and discussion). Partners or fathers were included in these educational promotions, if present. If PPIUD clients did not receive an IUD within 48 hours PP, they could not receive an IUD until after 4 weeks PP as per World Health Oranization (WHO) guidance.2 PP implant clients were eligible to receive an implant any time within 6 weeks PP. All PPFP methods were provided at no cost to the client.
Service delivery outcomes
The service delivery outcomes of interest included (1) the number of participants who received the intervention (at least one promotion) and delivered at a study health facility, (2) the number of participants declining a PPFP method, (3) the number of PP implant insertions and (4) the number of PPIUD (ParaGard TCu 380A) insertions. Only PPIUD clients had a 6-week insertion follow-up to check for IUD expulsion or discomfort (we reimbursed PPIUD clients for travel to and from follow-up appointments). PP implant clients received either levonorgestrel-releasing (Jadelle) or etonogestrel-releasing (Implanon) implants. PPIUDs were the non-hormonal copper IUD. If a participant received one-on-one promotion(s) but delivered at a non-study facility or at home, we assumed no PP LARC uptake unless she returned to a study facility for infant vaccinations and then elected to receive a PP LARC method.
Patient and provider experiences
PP implant and PPIUD clients and providers (nurses and midwives) were surveyed about their anxiety and pain during insertion (clients) and ease-of-insertion (providers) using 10-point Likert scale measures.
Data collection
Study nurses assigned participants unique codes lacking personal information during their first one-on-one promotion. Nurses manually recorded promotions, insertions and follow-up data, including Likert score data, in government logbooks then subsequently (≤1 week) uploaded that information into tablets using Survey CTO (Dobility, Cambridge, USA). We recorded demographic information only for those receiving a PPFP method.
Requirement for patient and public involvement statement
Our intervention and outcome measures were developed after extensive formative work with pregnant and PP women.6–9 Participants were not formally involved in recruitment. Results will be disseminated to stakeholders to support improving PPFP services.
Results
PPFP promotions
Study staff delivered a total of 13 694 one-on-one PPFP promotions prioritising PPFP methods between August 2017 and October 2018. Most of these women (n=12 068) delivered in one of our selected six health facilities. Promotions were distributed over four different intervention timepoints: ANC (28.0%), L&D (23.9%), in the PP ward (37.3%) and at infant vaccinations ≤6 weeks PP (10.8%).
Most participants received only one promotion (89%), while 9% received two, and 1% received three or four promotions. The average number of promotions per client was the same between the two LARC methods (1.1 promotions/clients, SDPP implant=0.4, SDPPIUD=0.3) (table 1). Receiving more promotions was associated with client uptake for PP implants (test for trend, X2 =65.8, p<0.0001) and PPIUDs (test for trend, X2 =26.9, p<0.0001).
Service delivery outcomes and participant characteristics according to postpartum long-acting reversible contraceptive choice in Kigali, Rwanda, August 2017–October 2018 (among n=12 068 women who received our intervention and delivered at a study health facility)
LARC uptake and insertion timing
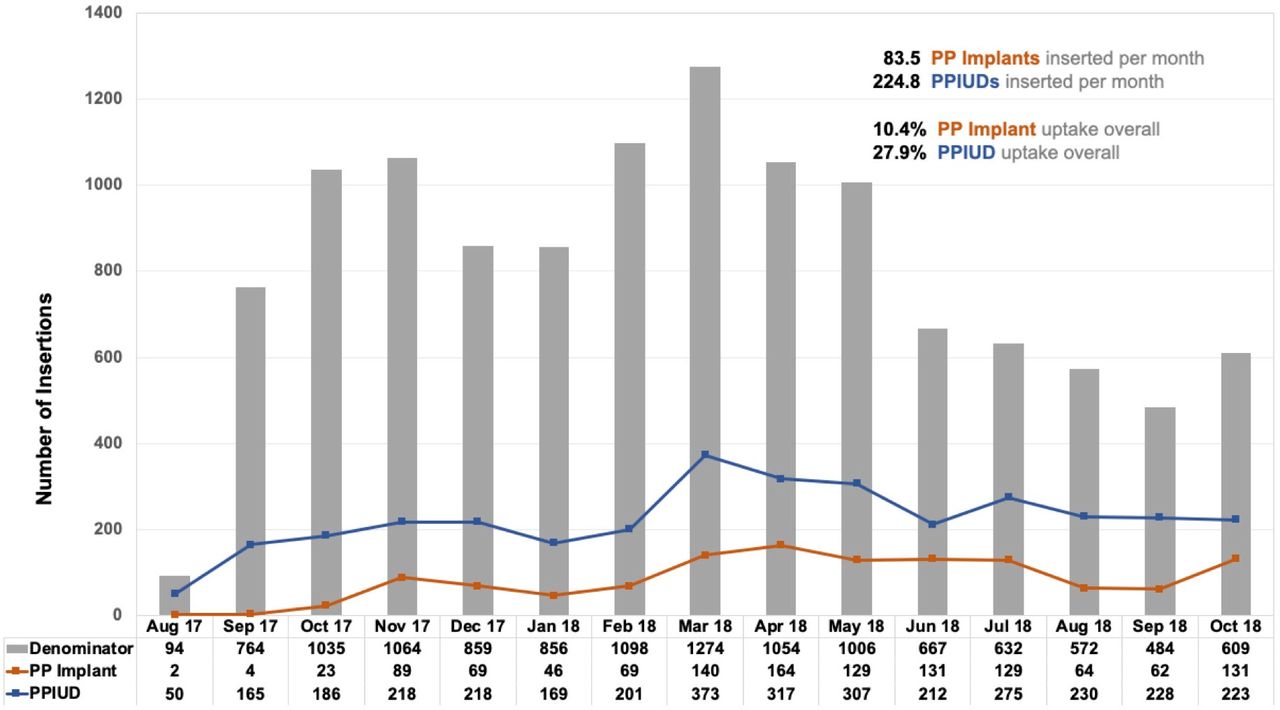
Of the 12 068 women who received our intervention and delivered at a study facility, 1252 chose a PP implant (10.4% uptake), 3372 chose a PPIUD (27.9% uptake) and 7444 declined a PP LARC method (61.7% non-uptake). Over the 15-month intervention period, providers at our intervention facilities inserted 83.5 (SD=51.9) PP implants/month and 224.8 (SD=75.3) PPIUDs/month . Notably, prior to our intervention, only 30 PP implant insertions/month and 8 PPIUD insertions/month occurred in our selected facilities. Figure 1 details insertions of the two PPFP methods over time.

{kind=link}
Postpartum implant (PP implant) and postpartum intrauterine device (PPIUD) insertions by month in Kigali, Rwanda, August 2017–October 2018 (among n=12 068 women who received our intervention and delivered at a study health facility).
PP implant insertions occurred more often before leaving the hospital (53%) versus within 6 weeks PP (47%) (table 1). In contrast, 91% of PPIUDs were inserted before the participant left the hospital while the remaining (9%) were inserted between 4 and 6 weeks PP. Promotions given during L&D (vs ANC) were associated with higher LARC uptake before women left the health facility after delivery (p<0.05). We observed a small but not statistically significant association between male presence and higher PP LARC uptake.
PP implant and PPIUD client demographics
On average, PP implant clients were 27.0 years old and PPIUD clients were 28.3 years old (p<0.0001). PP implant clients reported 2.3 (SD=1.3) previous live births on average while PPIUD clients reported 2.4 (SD=1.5) live births on average (not significantly different).
PP implant and PPIUD insertion outcomes
PP implant clients did not report any adverse reactions or discomfort due to their implants, and no PP implant client requested a removal measured up to the 6-week PP infant vaccination visit. Of the 77 women who experienced a PPIUD expulsion at follow-up, 12% elected to have a PP implant inserted while 60% chose to have an IUD reinserted (data not shown). All PPIUD expulsions were complete expulsions.
Using a Likert scale (where 1=no anxiety/pain and 10=maximum anxiety/pain), PP implant clients reported an average anxiety score of 2.1 (SD=2.6) and an average pain score of 2.0 (SD=2.6). Using the same scale, PPIUD clients reported an average anxiety score of 1.7 (SD=0.9) and an average pain score of 1.8 (SD=1.0). Reported ease-of-insertion by providers (where 1=maximum difficulty insertion and 10=no difficulty insertion) was high for both LARC methods (PP implants=9.9/10 (SD=0.7) and PPIUDs=9.2/10 (SD=1.0)) (table 1). There were no statistical differences in pain and anxiety score by timing of insertion.
Discussion
This article describes the uptake and service delivery outcomes of PP implants. We also present PPIUD uptake and outcome data with additional follow-up after our previous publication that focused only on the PPIUD.6
PP implant uptake was lower than PPIUD (10.4% vs 27.9%, respectively). In settings like ours, it is common for PP implants to be more popular than IUDs often due to concerns and lack of information about the less well-known IUD.12 13 However, our extensive formative work with clients before the intervention found that the non-hormonal nature and longevity of the IUD were desirable traits for potential clients and we also identified common concerns such as infection and side effects.7 In our intervention, we highlighted favourable aspects and discussed common concerns during educational promotion of all LARC and non-LARC methods. It is possible that the combination of evidence-based education about the IUD and access to trained providers certified in PPIUD insertion increased uptake of this method. Additionally, removing implants can be relatively difficult which may concern clients, and so it is critical that providers receive quality, specific training on implant removal for programmes to be effective.
Though most PP implant and PPIUD clients received an average of 1.1 promotions per person, there was a statistical relationship between having more promotions and electing to receive a LARC method. This finding suggests that repeat promotions may be important for uptake and is in line with a study from Nigeria which found multiple counselling sessions improved the use of modern PP contraceptive methods.14 Additionally, repeat promotions increases the opportunity for male engagement. In Rwanda, 80% of first ANC visits are attended by couples. We and others have found that male involvement in PP contraception discussions increases intention to uptake and actual uptake of PPFP in studies across sub-Saharan Africa.7 15–18
Our study demonstrated that PPFP services can be integrated into routine care within ANC, L&D and infant vaccination services. Other studies have focused on integration of FP services specifically within infant vaccination and have also found this to be a feasible and acceptable venue for services.19–24 We additionally demonstrate here that ANC and L&D are promising times to promote services, and that most PPFP uptake in our study occurred at L&D.
In previous in-depth interviews with key Ministry of Health stakeholders, it was generally agreed that reimbursing providers an additional amount for LARC provision was acceptable and ethical (as provision of PP LARC takes more training, skill and time than provision of other reversible methods). Moreover, we reimbursed providers at a higher rate for the IUD compared with the implant because of the additional training and certification required before providing PPIUDs. While this strategy was employed to remove any disincentive that providers may face in getting trained and providing PPIUDs, non-coercive provision of all contraceptive methods based on women’s preferences must always remain imperative and is a cornerstone of rigorous counselling procedures.
The only non-LARC methods available to PP (<6 weeks PP) breastfeeding women as per WHO recommendations are sterilisation, condoms and lactational amenorrhea (LAM).2 Women who are not breastfeeding may choose progestogen-only methods (eg, depot medroxyprogesterone acetate (DMPA) injectables) immediately PP. In our study, all pregnant and PP women were given counselling on condoms (with access to free condoms) and LAM. No women in our study selected immediate (before leaving the health facility) PP sterilisation, and no women stated that they did not intend to breastfeed.
Provision of integrated PPFP services was feasible and acceptable, and relied on ongoing stakeholder involvement for sustainability. The Rwandan Ministry of Health supported clinic staff to participate in PPFP training and helped to identify champions who oversaw clinical mentorship along with supportive clinic directors. To further support sustainability, we recently published a cost-effectiveness analysis of our intervention. The largest expense (34% of total) was personnel. Costs per insertion were $25/PPIUD and $77/PP implant and costs per couple-year of protection were $6/PPIUD and $21/PP implant.11 Kelly’s placental forceps were used for PPIUD insertion, and future studies may explore the expulsion rates and costs of using different insertion methods such as ringed forceps or dedicated inserters. These analyses are important to inform the cost of scaling up PPFP services and indicate that, when funding is limited, it may be more cost-effective to prioritise promotions and training for the PPIUD.
Limitations
We collected minimal demographic data during this service delivery intervention, and only for PP implant and PPIUD clients. As a result, we are not able to compare demographics between those who declined a LARC method to those who did not decline. We did not collect data on whether IUD expulsions were recognised by women or on use of non-LARC methods (sterilisation, self-reported condom use or self-reported LAM practices) after leaving the health facility which would have been informative. We also did not document reasons why women with a stated desire for a PPFP method did not receive one at a health facility, which is a future area of exploration. Finally, understanding the effect of engaging community health workers in creating demand and reducing misconceptions, which has shown promise in improving uptake of contraceptive methods,25 would be informative.
Conclusions
PP implant and PPIUD uptake significantly increased after implementation of our multilevel intervention focused on PPFP supply, demand and sustainability. The PPFP methods were well-received by clients and providers. With renewed interest in PPFP services, our comprehensive multilevel intervention, which is replicable and expandable, is extremely well-timed to make a significant impact on PPFP services in Rwanda and other countries.
Data availability statement
Data are available in a public, open-access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Wall, Kristin, 2018, "Replication Data for: an interim evaluation of a multi-level intervention to improve post-partum intrauterine device (PPIUD) services in Rwanda", https://doi.org/10.7910/DVN/WLZ7PC, Harvard Dataverse, V1.
Ethics statements
References
Footnotes
Contributors AM, LBH, VU, AT: made substantial contributions to the interpretation of data; drafted the work or revised it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. JN, JE, AH, JM, EK, RP: made substantial contributions to the design of the work; made substantial contributions to the analysis and/or interpretation of data; drafted the work or revised it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. KMW, RI, VDC, SA: made substantial contributions to the conception and design of the work; made substantial contributions to the acquisition, analysis, and interpretation of data; drafted the work or revised it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding This work was supported by the Bill & Melinda Gates Foundation (OPP1160661). Additional support came from the Emory University Research Council Grant (URCGA16872456), Emory Global Field Experience Award, the Emory Center for AIDS Research (P30AI050409), the National Institutes of Health (NIAID R01 AI51231; NIAID R01 AI64060; NIAID R37 AI51231) and Emory AITRP Fogarty (5D43TW001042).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.