Article Text

Abstract
Introduction This trial reports on use of the copper intrauterine device (IUD) after immediate compared with delayed insertion following medical abortion at 17–20 gestational weeks (GW).
Methods This randomised controlled trial was conducted at one tertiary hospital and five community healthcare centres in Cape Town, South Africa. Eligible consenting women were randomised to immediate (within 24 hours) or delayed (3 weeks post-abortion) insertion of the copper IUD. Follow-up was at 6 weeks, 3 months and 6 months. Main outcomes were use of the original IUD and use of any IUD, including replacement IUDs at 6 weeks post-abortion. Secondary outcomes included rates of expulsion and malposition at 6 weeks, use of any IUD at 3 and 6 months, and acceptability of the IUD.
Results We recruited and randomised 114 women admitted for elective medical abortion between August 2018 and June 2019. In the immediate and delayed study arms, respectively, 45/55 (82%) and 12/57 (21%) women received the IUD as planned. By intention-to-treat, 56% in the immediate and 19% in the delayed arms were using the original IUD at 6 weeks (p<0.001), and 76% in the immediate and 40% in the delayed arms were using any IUD (p<0.001). Complete expulsion or removal occurred in 32% in the immediate and 7% in the delayed arms (p=0.044).
Conclusions Insertion of an IUD immediately after medical abortion at 17–20 GW results in increased use after 6 weeks compared with delayed insertion, however expulsion rates are higher than with interval insertion.
Clinical trials registration NCT03505047), Pan African Trials Registry (www.pactr.org), 201804003324963
- abortion
- induced
- contraceptive Effectiveness
- intrauterine devices
- copper
- randomised controlled trial
Data availability statement
Data are available upon reasonable request. De-identified participant data will be made available on request by the first lead author, Dr Deborah Constant (deborah.constant@uct.a.za). Re-use of data is permissible for secondary analysis. Additional information available on request includes the study protocol and CRFs.
Statistics from Altmetric.com
Key messages
Insertion of an intrauterine device (IUD) immediately after medical abortion at 17–20 gestational weeks is more effective compared with delayed insertion.
Expulsion rates for immediate insertion are higher and additional contraceptive barrier protection may be recommended for the first 6 weeks.
Continuity of care is recommended to strengthen follow-up rates at 6 weeks for clinical assessment of IUD location.
Introduction
Globally there is a continued high unmet need for contraception.1 Long-acting reversible contraceptives (LARC) such as the intrauterine device (IUD) are one of the most effective contraceptive methods, but users face numerous barriers to access .2–6 In South Africa, two-thirds of women have had an unplanned pregnancy in the previous 5 years with only 1.6% reporting IUD use.7
Clinical trials show that IUD use is higher after immediate compared with delayed insertion after surgical and medical abortion in the first trimester, and surgical abortion in the second trimester, but that expulsion rates are often higher at later gestations.8–11 The evidence is conflicting with respect to immediate insertion after vaginal delivery, with expulsion or removal rates varying between 3% and 47%, but in most contexts the benefits of immediate contraception were found to outweigh the risks.12–14
It remains unclear whether the IUD can be effectively inserted after medical abortion in the second trimester.11 15 To our knowledge no studies have evaluated the risk–benefit ratio of immediate IUD insertion after medical abortion at 17–20 gestational weeks (GW) where a higher cumulative dose of the uterotonic misoprostol is often used.
The primary objective was to compare copper IUD use following immediate versus delayed insertion after medical abortion at 17–20 GW. The secondary objective was to compare acceptability of the IUD in these groups.
Methods
The study was approved by the Human Research Ethics Committee at the University of Cape Town (HREC 007/2018) and the Western Cape Provincial Government (WC_201804_006). The trial was registered at clinicaltrials.gov/ (ID NCT03505047) and www.pactr.org (ID PACTR201804003324963).
Study procedures
We performed a randomised controlled trial (RCT) at a tertiary level teaching hospital and five affiliated community healthcare facilities (CHFs) in Cape Town, South Africa between August 2018 and December 2019. Eligible women were ≥18 years old; undergoing medical abortion between 17 and 20 GW by ultrasound, the upper legal gestational limit; and opting and eligible for the copper IUD (NovaT380) as post-abortion contraception. Women were informed about the study during a group contraceptive counselling session prior to clinical evaluation for the termination. They were enrolled in the study after eligibility screening and giving informed consent. A researcher not involved in study procedures generated the randomisation sequence 1:1 in random permuted blocks of 4–6 and prepared sequential opaque sealed envelopes, stored in a locked box. Two field workers performed the randomisation allocation with the participant after admission to the gynaecological ward. The nature of the study did not permit blinding of study staff, clinical providers or participants. Between August 2018 and June 2019, we enrolled 114 women undergoing medical abortion with the mifepristone–misoprostol regimen.
All women received oxytocin 20 IU intravenous following fetal expulsion. For participants in the immediate arm, clinicians planned to insert the IUD within 24 hours of abortion completion and prior to discharge. The IUD was inserted by the on-call physician in the ward examination room as soon as feasible after spontaneous expulsion of the fetus and placenta, or in the operating theatre if vacuum aspiration for retained placenta was performed. It was not inserted in cases of prolonged rupture of membranes (>18 hours), heavy bleeding (>500 mL) at planned time of insertion, or signs of infection (fever or foul-smelling discharge) post-abortion. Women in the delayed arm were provided with 4 weeks of oral contraceptive pills and referred for insertion at their referral CHF. Delayed insertion was scheduled for 3 weeks post-abortion.8 IUDs were inserted by trained reproductive health nurses. All insertions were performed using a standard introducer without ultrasound guidance.
Participants were scheduled for an in-person follow-up visit including an ultrasound 6 weeks after the abortion with the study clinician at the tertiary hospital outpatient department. Participants not returning were reminded three times by message and voice call to complete study follow-up. Non-returnees were interviewed by telephone. Two subsequent follow-up interviews took place by telephone at 3 and 6 months. Non-responders were visited at their homes for interviews. Participants received a total of €30 compensation for participation in the study.
Patient and public involvement
The design and conduct of the study did not involve patient–public engagement; however, we explored participants’ and providers’ views on the impact of the trial processes and feasibility of the intervention in a separate process evaluation.
Outcomes
For our primary outcome we distinguish between use of the original IUD and use of any IUD, which includes replacement IUDs, at 6 weeks.
Use of the IUD was defined as an adequately placed IUD without clinical indication for removal. We determined that the IUD was adequately placed if it had an intrauterine location by ultrasound and did not cause symptoms warranting removal. If the IUD stem was visible in the cervix, it was considered intracervical and removed. IUDs with an intrauterine malposition (>2 cm from the fundal endometrium) associated with pain or abnormal discharge were removed.
Secondary outcomes were rates of complete expulsion, intracervical location, symptomatic malposition and IUD-related complications at 6 weeks (perforation and systemic infection), use of any IUD at 3 and 6 months, cramping at 3 months and pain on insertion measured on Likert scales, preference for immediate or delayed insertion, satisfaction with IUD, planned duration of IUD use, and pregnancy within 6 months.
Data capture and hierarchy
We recorded outcome data from ultrasound records, follow-up interviews, and paper and electronic medical records from CHFs for the whole Cape Town Metropolitan area. If e-records showed a participant visited a healthcare facility within 6 months of the abortion, her clinical chart was reviewed for relevance to the study outcomes or adverse events.
The presence of an IUD at 6 weeks was primarily determined by ultrasound. If participants did not come for follow-up, self-report was accepted. The absence of documented IUD insertion in medical records was interpreted as non-use, which minimised missing data for our primary outcome in the delayed group. Secondary outcome data were captured in interviews that were sometimes truncated, resulting in varying missing data frequencies.
Analysis
Main outcomes were assessed after 6 weeks in an intention-to-treat (ITT) analysis of all eligible randomised participants (n=112) and a non-randomised, observational comparison of all participants followed up, either in person, by interview or by record review, according to the intervention received. Secondary outcomes were assessed at either 6 weeks, 3 months or 6 months post-abortion, according to ITT or non-randomised comparison groups as appropriate.
Continuous outcomes were summarised using medians and interquartile range for non-normal distributions and compared group-wise using Wilcoxon rank-sum tests. Categorical outcomes were compared using Chi-square or Fisher’s exact test as appropriate. A sensitivity analysis was performed to control for uncertainty of data in cases where IUD use was based on self-report. Power calculations and analyses were conducted in STATA v.15 and significance levels are reported at p<0.05.
Sample size
Our sample size was determined in order to show a hypothesised two-fold increase (80% vs 40%) in IUD use at 6 weeks in the immediate compared with the delayed group, with anticipated loss-to-follow-up of 20%, 80% power and two-sided alpha of 0.05. To have sufficient power for a stratified subanalysis of participants undergoing vacuum aspiration, assumed to be 50%, we doubled the required sample size from 55 to 110.
Results
We screened 136 women fulfilling the primary inclusion criteria. A total of 114 eligible women were randomised, four of whom were discontinued prior to receiving their intervention. Two had a contraindication to the IUD, not identified during screening, and two changed their mind regarding participation. The two women recruited by error were excluded from the analysis and the two that changed their mind were included in the ITT analysis (n=112) (figure 1).

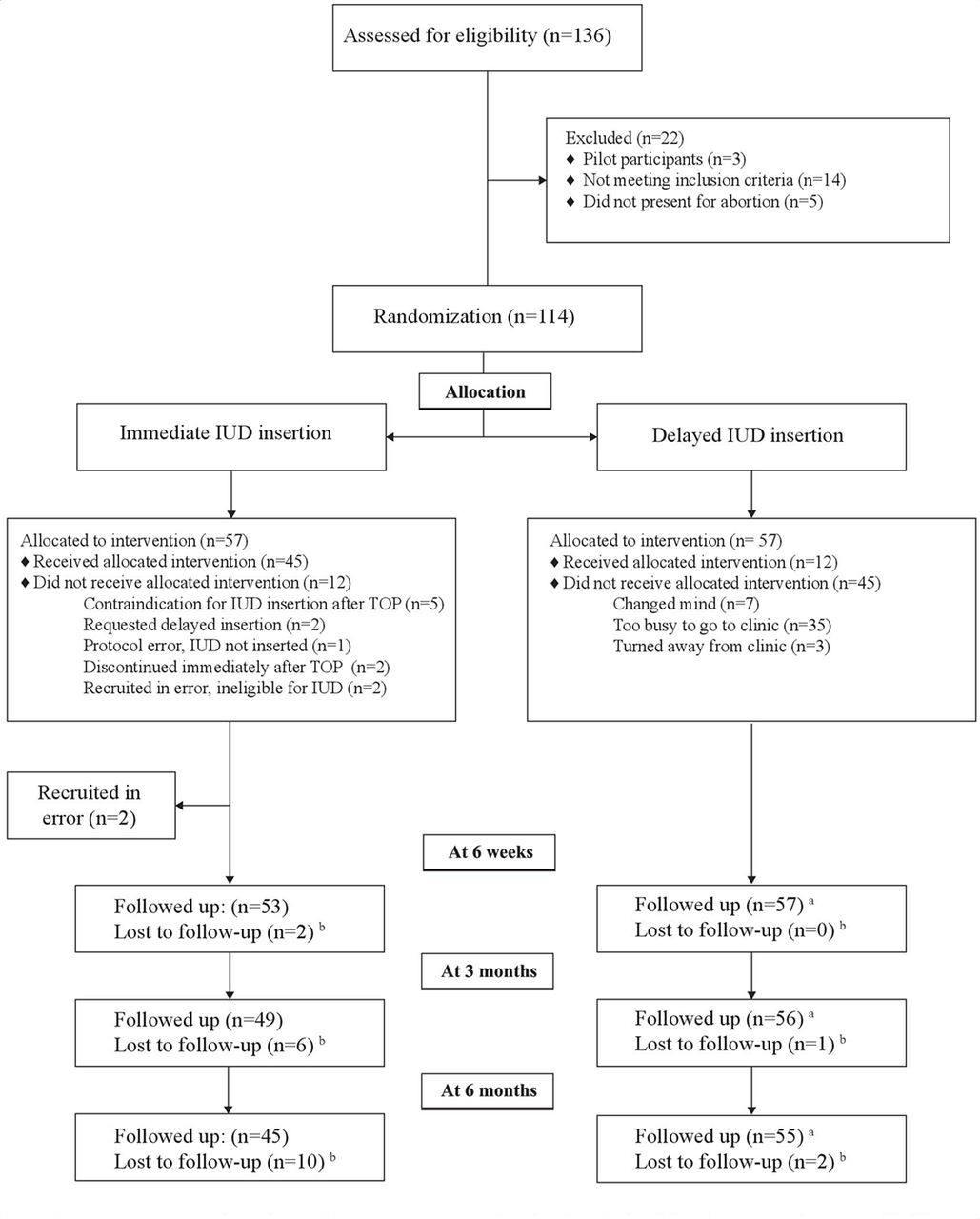{kind=link}
Flow chart for uptake and use of the copper intrauterine device according to intention-to-treat among participants allocated to immediate or delayed insertion after medical abortion at 17–20 weeks’ gestation. IUD, intrauterine device; TOP, termination of pregnancy.
Gestational age ranged from 17 weeks 1 day to 19 weeks 6 days. By ITT grouping, median gestational age was 19 weeks 0 days in the immediate group and 19w2d in the delayed arm (p=0.03), which was assessed as clinically insignificant. All other background parameters did not differ statistically between the study arms. table 1 shows the background and reproductive characteristics of participants according to ITT and non-randomised comparison groups. Abortion-related variables were not significantly different between groups (online supplementary table S1).
Supplemental material
Sociodemographic and reproductive characteristics of women allocated to immediate or delayed insertion of the copper intrauterine device after medical abortion at 17–20 weeks’ gestation
Intention-to-treat analysis
The ITT analysis included all eligible randomised women (n=112), 55 women in the immediate arm and 57 women in the delayed arm (table 2). In the immediate arm, 45 women (82%) received the IUD as planned. Eight women crossed over to the delayed arm (figure 1), and two changed their mind about study participation and were discontinued. Of 57 women in the delayed arm, only 12 (21%) had IUDs inserted as planned (figure 1).
Intention-to-treat analysis of continued use of the intrauterine device (IUD) among women randomised to immediate or delayed insertion of the copper IUD after medical abortion at 17–20 weeks’ gestation
Use of the original IUD at 6 weeks was 56% in the immediate group and 19% in the delayed group (p<0.001). At the end of the 6- week follow-up period, 42 women (76%) in the immediate arm, and 23 (40%) in the delayed arm were using the original or a replacement IUD (p<0.001). At 3 months, use of the original, or any IUD, was 49% and 69% in the immediate group and 18% and 37% in the delayed group, respectively. Corresponding figures at 6 months were 40% and 55%, and 14% and 26%, respectively. Decreasing rates for use were mostly due to loss-to-follow-up; one woman in the immediate and one in the delayed arm reported they had the IUD removed between the 6- week and 6-month follow-up.
In the sensitivity analysis we categorised self-reported use in the immediate group not corroborated by ultrasound (n=2) as “non-use” instead of “use”, and self-reported use not corroborated by medical records at 6 weeks in the delayed group as “use” instead of “non-use”. This resulted in 51% and 26% (p=0.01) use of the original IUD at 6 weeks in the immediate arm and the delayed arm, respectively. By subanalysis of women in the immediate arm, expulsion or removal of IUDs inserted after vacuum aspiration was not significantly different from those inserted without aspiration (32% vs 29%, p=0.81).
Non-randomised, observational comparison
A total of 29 of 43 women (67%) who received immediate insertion were using the original IUD at 6 weeks, and 40 women (93%) were using the original or a replacement IUD (table 3). Among 65 women planned for delayed insertion per non-randomised comparison, 14 women (22%) had an IUD inserted and 13 (20%) were still using it at 6 weeks.
Non-randomised, observational comparison of continued use of the intrauterine device (IUD) at 6 weeks among women who received immediate or delayed insertion of the copper IUD after medical abortion at 17–20 weeks’ gestation
Among women with immediate insertion not using the original IUD after 6 weeks, 6 (14%) had complete expulsion and 8 (18.5%) had the IUD removed because of intracervical location or symptomatic malposition. One woman with delayed insertion had the IUD removed because of symptomatic malposition. Two women had an unintended pregnancy in the 6 months following the abortion, both followed the delayed arm protocol. We identified no serious IUD complications among participants.
The rate of localised infection, persistent cramping, and satisfaction with the IUD at 3 months did not differ significantly between groups (online supplementary table S2). Some 87% of women who had immediate and 61% who had delayed insertion said they would have preferred immediate insertion, given the choice (p=0.02).
Supplemental material
Discussion
Main findings
Immediate IUD insertion resulted in significantly higher rates of use at 6 weeks, 3 months and 6 months compared with delayed insertion, despite higher rates of expulsion or removal. This study explored both efficacy measures, such as expulsion and removal rates, and effectiveness measures such as how immediate insertion affects continued use. We found that four out of ten women planned for immediate IUD insertion will either not have the IUD inserted, have the IUD removed, or expel the IUD. However, if a woman receives the IUD before she leaves the hospital, it is likely that she will continue to use the original, or a replacement IUD, if provided with continuity of care, as demonstrated by a 93% continuation rate at 6 weeks among women who received immediate insertion. Both groups predominantly experienced no or mild pain on IUD insertion and showed a preference for immediate insertion despite many in the immediate group needing removal and replacement of the original IUD. Two systematic reviews of immediate versus delayed IUD insertion after abortion in the first and early second trimester similarly concluded that immediate insertion was associated with higher expulsion rates but also higher rates of continued use.10 11
Immediate insertion was associated with higher rates of expulsion and removal due to malposition compared with delayed insertion. Interestingly, most women with intracervical IUD placement were asymptomatic. Some studies indicate that intracervical placement does not affect IUD effectiveness .16 17 It is possible that a string check at follow-up would have been sufficient and resulted in a higher continued use of the original IUD. A Finnish study found expulsion/removal rates after same-day insertion of 27.5% after later first-trimester abortion and 18.5% after early second-trimester abortion, although the study was underpowered for the second trimester group.15 Expulsion and removal rates have been estimated at 5% and 8.5% after first- and second-trimester surgical abortion, respectively, but these studies accepted self-report of IUD use, which may underestimate malposition rates18 19 It is possible that the high cumulative doses of misoprostol needed for medical abortion in the second trimester and a more dilated cervix contributed to the relatively higher expulsion/malposition rates. Studies on post-placental IUD insertion also indicate that insertion within the first 10 minutes of placental delivery is more effective than insertion at 10 minutes to 48 hours, which may also be true for post-abortion insertion and which this study cannot evaluate.13
Four of the six women with complete expulsion did not notice the expulsion and thus would be unknowingly unprotected from an unintended pregnancy had they not returned for follow-up. However, women in the immediate study arm were much more likely to follow up in person compared with the delayed arm.
The low rates of use in the delayed arm were because only one in five women presented at CHFs for IUD insertion. This was despite several study measures to facilitate interval insertion at CHFs. Interval initiation of contraception post-abortion and postpartum is known to be complicated by low adherence, which is a main rationale for quick-start contraception.8 20 Finally, two women who followed the delayed protocol had unintended pregnancies within 6 months. During the post-pregnancy period women are especially vulnerable to repeat pregnancy and this must be considered in the risk–benefit calculation of immediate and delayed IUD insertion.21
Strengths and limitations
Immediate insertion of the IUD after medical abortion at 17–20 GW has not to our knowledge been studied. Our estimated sample size did not accurately predict how many women would not receive an IUD in the immediate group or how many would fail to follow through for delayed insertion. Despite this, findings were statistically significant and loss-to-follow-up lower than predicted.
Currently, clinical services have little experience with IUD insertions. Therefore, all relevant staff members received structured mentoring sessions in IUD insertion after medical abortion prior to the study start. The feasibility of the intervention is being explored in a separate process evaluation.
Conclusions
Insertion of an IUD immediately after medical abortion at 17–20 GW results in increased use after 6 weeks, 3 months and 6 months compared with delayed insertion. Expulsion rates are higher than interval insertion and immediate insertion at earlier gestation but similar to immediate insertion after term delivery.
Data availability statement
Data are available upon reasonable request. De-identified participant data will be made available on request by the first lead author, Dr Deborah Constant (deborah.constant@uct.a.za). Re-use of data is permissible for secondary analysis. Additional information available on request includes the study protocol and CRFs.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DC and ME are shared first author.
Twitter @DrDGrossman
Contributors DC was the principal investigator from proposal writing up to final write up. ME was the co-principal investigator from research design up to final write up. DG participated in study design, analysis, manuscript preparation and editing. GP participated in study execution, manuscript preparation and editing. MP participated in study execution, manuscript preparation and editing.
Funding This study was funded by Anonymous donor (5290); National Research Foundation of South Africa/Swedish Foundation for International Cooperation in Research and Higher Education (170825260615/112631), Swedish Society of Medicine (SLS-783181), Swedish Society of Medical Research (P17-0214).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.