Article Text

Abstract
Background Globally, access to safe abortion is limited. We aimed to assess the safety, effectiveness and acceptability of harm reduction counselling for abortion, which we define as the provision of information about safe abortion methods to pregnant persons seeking abortion.
Methods We searched PubMed, EMBASE, ClinicalTrials.gov, Cochrane, Global Index Medicus and the grey literature up to October 2021. We included studies in which healthcare providers gave pregnant persons information on safe use of abortifacient medications without providing the actual medications. We conducted a descriptive summary of results and a risk of bias assessment using the ROBINS-I tool. Our primary outcome was the proportion of pregnant persons who used misoprostol to induce abortion rather than other methods among those who received harm reduction counselling.
Results We included four observational studies with a total of 4002 participants. Most pregnant persons who received harm reduction counselling induced abortion using misoprostol (79%–100%). Serious complication rates were low (0%–1%). Uterine aspiration rates were not always reported but were in the range of 6%–22%. Patient satisfaction with the harm reduction intervention was high (85%–98%) where reported. We rated the risk of bias for all studies as high due to a lack of comparison groups and high lost to follow-up rates.
Discussion Based on a synthesis of four studies with serious methodological limitations, most recipients of harm reduction counselling use misoprostol for abortion, have low complication rates, and are satisfied with the intervention. More research is needed to determine abortion success outcomes from the harm reduction approach.
Funding This work did not receive any funding.
PROSPERO registration number We registered the review in the PROSPERO database of systematic reviews (ID number: CRD42020200849).
- abortion
- induced
- patient safety
- abortifacient agents
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
This review article examines abortion harm reduction interventions, or the provision of information about how to safely induce abortion without the provision of actual medications.
Most pregnant persons who participate in these interventions use misoprostol to induce abortion.
Based on few studies of poor quality, it appears that persons who participate in these interventions have low complication and high satisfaction rates.
Introduction
Globally, access to safe abortion is limited. As a result, an estimated 25 million unsafe abortion occur each year, and at least 22 800 women die from resulting complications, almost all in low- and middle-income countries.1 This is often due to restrictive laws which prohibit abortion; but even in contexts where abortion is legal, other barriers, such as cost, distance and regulatory barriers, may limit access to services.2
One approach to mitigating the consequences of unsafe abortion where traditional clinician-directed abortion care is not an option has been to provide pregnant persons seeking abortion with harm reduction counselling. While the term ‘harm reduction’ is most often used in the context of substance abuse, it can be more broadly understood as a set of interventions that reduce the negative effects of certain health behaviours without seeking to completely eliminate those behaviours.3
In the context of abortion, the term has been used to describe interventions aimed at providing pregnant persons seeking abortion with information about how to safely self-administer abortifacient medications. This often includes risk assessment or screening and follow-up medical care, but does not include providing the actual medications.2 This strategy is considered promising because, while eradicating unsafe abortions may not be immediately feasible, particularly in legally restrictive settings, providing information to make abortions safer may reduce the burden of unsafe abortion morbidity.
In the early 2000s, physicians in Uruguay used a ‘risk reduction strategy’ to address the problem of maternal morbidity and mortality due to unsafe abortion. They offered women who were considering an abortion a ‘pre-abortion’ counselling visit, during which they imparted information about how to safely administer misoprostol, and a ‘post-abortion’ follow-up visit. They reported very low complication rates and used their programme to advocate for legal change in the country.4 The programme eventually served as a framework for providing safe abortion care once abortion was legalised.5
Other approaches to applying a harm reduction framework to abortion have included providing information through telephone hotlines,6 7 training pharmacists to assess for medical abortion eligibility,8 and distributing misoprostol through community-based organisations.9
In this review we focus on harm reduction counselling, which we define as the direct provision of information to pregnant persons seeking abortion. The purpose of the systematic review is to assess the safety, effectiveness and acceptability of harm reduction counselling for pregnant persons seeking induced abortion. This review is needed because there is increasing interest in using harm reduction approaches to improve access to abortion in legally and otherwise restrictive settings,2 but a thorough review of the evidence in favour of harm reduction counselling does not currently exist.
Methods
Search strategy
We conducted a systematic search of published studies in PubMed, Embase, Cochrane, Clinicaltrials.gov and Global Index Medicus. We also searched the grey literature for relevant studies (OpenGray, Google Scholar). We performed the initial search in July 2020 and did not exclude studies based on language, setting or timing of publication. We repeated the search and updated the study diagram in October 2021. We used search constructs appropriate for each database (see online supplemental file 1). We uploaded citations in Mendeley and removed duplicates prior to uploading citations to Covidence. Two researchers (BMS and RG) performed title and abstract screening of all studies, and full-text screening of studies that seemed to meet the inclusion criteria. We resolved any conflicts via discussion until reaching consensus, and a third researcher (CRK) intervened when conflicts could not be resolved by the first two researchers. We report our methods and results in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).10
Supplemental material
Study selection
We defined harm reduction in the context of abortion as the direct provision (by any kind of healthcare provider) of information about safe abortion methods to pregnant persons seeking induced abortion. We included published studies that were primary studies, including randomised trials, cohort and case-control studies and cross-sectional studies. We included studies that reported on outcomes relating to the effectiveness, safety and acceptability of harm reduction counselling; also studies of any sample size and with any type of comparison group, including no comparison group. Included studies had to report on our primary outcome, which was the proportion of pregnant persons who used misoprostol for abortion. We chose this as our primary outcome because we considered use of misoprostol to be the most important marker of safe abortion, and our primary objective was to evaluate harm reduction counselling as a strategy to reduce the harms of unsafe abortion. Our secondary outcomes were:
The proportion of users who had an abortion (utilising any method) after harm reduction counselling
The proportion of users who had a complete abortion after taking misoprostol
The proportion of users who had an aspiration procedure after taking misoprostol
The proportion of users who had complications, defined as infection not requiring intravenous (IV) antibiotics or hospital admission; haemorrhage or prolonged bleeding not requiring transfusion
The proportion of users who had serious complications, defined as infection requiring IV antibiotics or hospital admission; haemorrhage requiring blood transfusion or other complication requiring hospital admission, other than simply for aspiration
The proportion of users who attended a follow-up visit
The proportion of users who were satisfied with the harm reduction counselling they received
The proportion of users who were using a contraceptive method after harm reduction counselling
Ease of obtaining misoprostol
Location where misoprostol was obtained.
We excluded studies describing other approaches aimed at reducing the harms of unsafe abortion if they did not involve direct counselling of pregnant persons within the healthcare system (eg, the provision of information via hotlines or to pharmacists). We also excluded approaches that provided pregnant persons with the actual abortifacient medications or abortion procedures (eg, community-based distribution of misoprostol) as the purpose of this review was to evaluate the effectiveness of harm reduction counselling. We excluded commentaries, editorials, letters, advisories, conference abstracts and review articles.
Study synthesis and assessment
One researcher (BMS) extracted data on outcomes compatible with our predefined outcomes. We performed a narrative synthesis of the reported outcome results.
Two researchers (BMS and RG) independently conducted a risk of bias assessment for all included studies using the ROBINS-I tool for assessing risk of bias in nonrandomized studies of interventions (box 1). The tool includes seven bias domains: bias due to confounding, selection bias, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported result.11
ROBINS-I tool for assessing risk of bias in nonrandomized studies of interventions
Bias due to confounding
Bias in selection of participants into the study
Bias in classification of interventions
Bias due to deviations from intended interventions
Bias due to missing data
Bias in measurement of outcomes
Bias in selection of the reported results
For each domain, we rated the risk of bias as either low, high or unclear. Of note, for bias due to missing data, we selected a 25% lost to follow-up cut-off point for a definition of high risk of bias. Any conflicts between the two researchers were resolved by a third researcher (CRK). We searched for trial protocols and registration prior to making judgement on the reporting biases.
We could not perform a meta-analysis because of the overall quality and heterogeneity of the included studies, which differed significantly in terms of outcomes reported and means of assessing outcomes.
Registration
We registered the review in the PROSPERO database of systematic reviews (ID number: CRD42020200849). The review protocol is accessible through the database.
Results
Characteristics of included studies
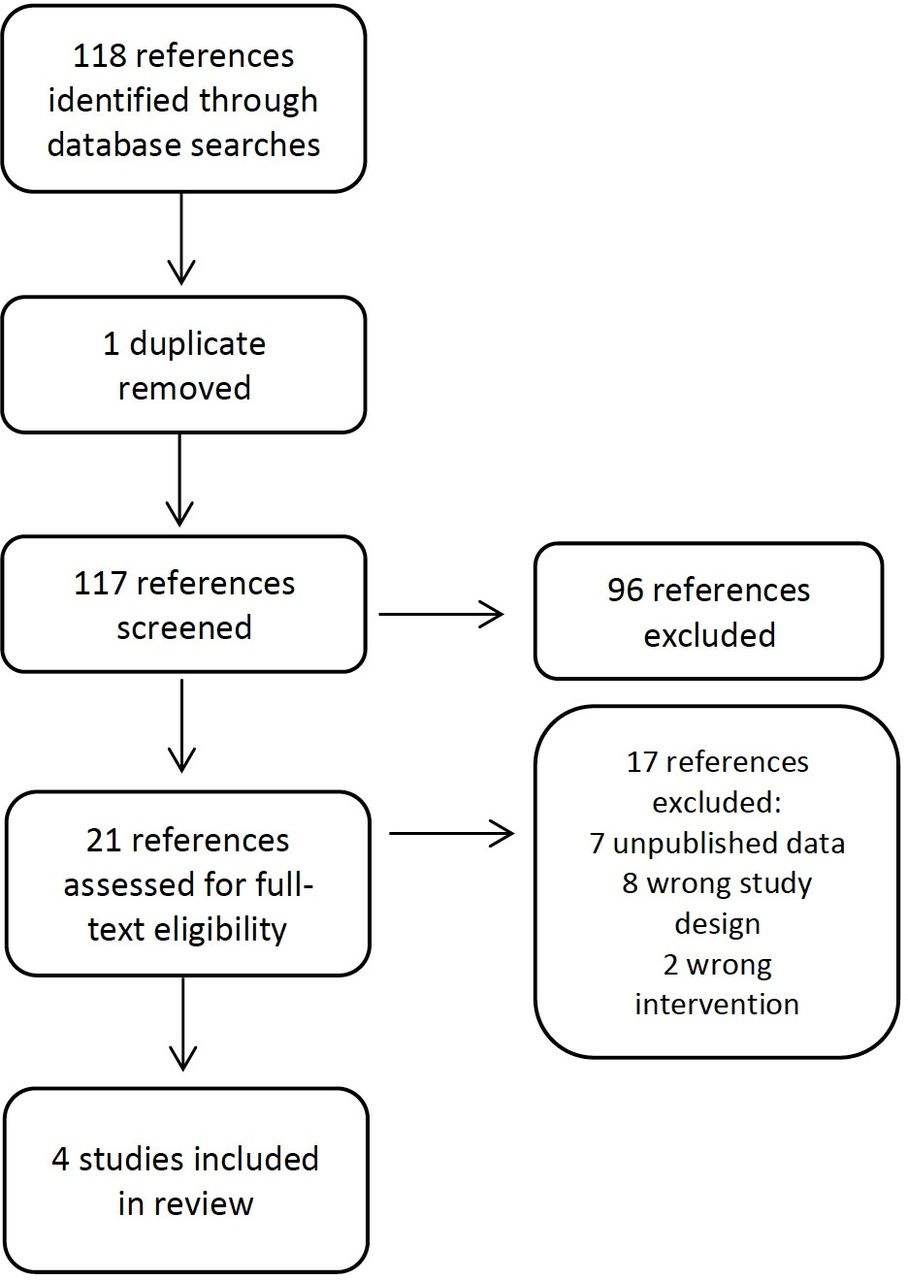
We identified 118 studies through database and grey literature searches. We excluded 96 references because they did not meet inclusion criteria, while 21 studies met criteria for full-text review. Of these, we excluded 17, as shown in the PRISMA diagram (figure 1). Of note, we excluded two articles that reported as their only outcome a changing rate in maternal mortality that coincided with the implementation of a harm reduction intervention.12 13 We included four studies in the review, which were conducted in three countries. All were observational studies with no comparison groups, and the harm reductions interventions were similar (table 1).
{kind=link}
PRISMA study flow diagram.
Characteristics of included studies
The first study was conducted at one public hospital in Uruguay and included 675 women who received harm reduction counselling, of whom 73% completed a follow-up visit.4 The intervention included pregnancy confirmation, gestational age assessment by ultrasound, and information about how to use misoprostol.
The 2016 study by the same group describes a scale-up of the same strategy to eight public health centres in four departments in Uruguay.14 Although 2717 women received the intervention, only 27% attended a follow-up visit. The authors did not state why the lost to follow-up rate was significantly higher than in their 2006 study.
The third selected study was conducted in Tanzania.15 The intervention differed in that ultrasound was only used to assess gestational age if the pregnant person did not remember the date of their last menstrual period. This study had a clinical follow-up component, and a separate survey of a convenience sample of 50 participants. Of the 110 patients enrolled, 50% completed follow-up.
The fourth study was conducted in Peru.16 The intervention was similar to that described in the Uruguayan studies, except that participants could select telephone or in-person follow-up. This study also included a survey and presented survey results separately from those of the clinical follow-up. Of the 500 patients included, only 35% completed in-person or telephone follow-up. Outcomes of interest to this review are reported for 253 of the 500 patients (51%) who completed the survey.
Synthesis of results
The four selected studies included a total of 4002 participants, but outcomes were only available for participants who completed follow-up,4 14 for participants who completed follow-up or responded to a research survey,14 or only for participants who responded to a research survey17 (table 2).
Summary of included studies by outcome reported
For the primary outcome, the proportion of pregnant persons who used misoprostol to induce abortion, rates varied from 79% (as reported in the survey component of the Kahabuka et al study) to 100% in the Briozzo et al 2006 study.4 14 Of note, 100% of the participants who completed clinical follow-up in the Kahabuka study used misoprostol.15
In terms of secondary outcomes, the proportion of participants who proceeded to induce an abortion after counselling ranged from 88% to 96%.4 15 16 All studies reported low complication rates, and none reported any deaths. A total of 71/4002 participants had complications (overall complication rate 1.8%) but only two had serious complications – hospital admission for treatment of infection. All other complications were considered mild and included post-abortion infection not requiring intravenous antibiotics or hospital admission, haemorrhage not requiring blood transfusion, pain, and prolonged bleeding. The complication rate ranged from 0.6% to 8% whereas the serious complication rate was 0%–1%.
Two studies reported uterine aspiration rates, which ranged from 6% to 22%.15 16 One study reported that the aspiration rate decreased over time, from 30% to 18%, but did not report an overall aspiration rate.4 The complete abortion without aspiration rate was only explicitly reported in one study16 and was 66%, but for 24/220 (11%) participants the outcome was unsure at the time of interview.
Two studies reported on the ease of obtaining misoprostol and found that 52%–87% of participants found it very or somewhat easy to obtain.15 16 The same studies also reported on the location where misoprostol was obtained and found that 80%–90% of participants obtained it from pharmacies.15 16
Three of the four studies reported on participant satisfaction with the harm reduction counselling intervention, with satisfaction rates ranging from 85% to 98%.14–16
Three of the four studies reported on contraceptive initiation rates after the harm reduction counselling visits: these ranged from 55% to 76% of participants using a contraceptive method.14–16
Quality of the evidence
We rated the quality of the evidence for all selected outcomes as low, because all the included studies were observational and did not include comparison groups. Further, the primary outcome, which was the proportion of pregnant persons who used misoprostol to induce abortion, was self-reported in all four studies. Because there were no comparison groups, we rated the risk of bias in classification of interventions as low for all studies. For several of the biases included in the ROBINS-I tool, the selected studies did not offer sufficient information to accurately assess the risk of bias.
Loss to follow-up rates were high in all four studies, which meant that bias due to missing data was high. Three of the four studies conducted some analysis of the participants lost to follow-up. For one of the studies conducted in Uruguay,14 the authors contacted a convenience sample of 94 of the 1988 women who did not return for follow-up and found that only 53.2% had a termination, while 21.3% chose to continue the pregnancy (the proportion who induced abortion among those who did follow up is not explicitly reported). The authors of the study conducted in Tanzania15 compared characteristics of the 55 users who did not follow up and the 55 users who did and found no statistically significant differences between the groups. The third study16 compared participants who followed up in person to those who followed up via telephone and to those who did not receive any follow-up. Participants recruited at a more rural site were less likely to follow up in person and more likely to follow up via telephone; those who did not follow up were less likely to have felt comfortable asking questions at the consultation and less likely to recommend the services to a friend or use it again if necessary.
Three of the studies did not have published research protocols, and we were therefore unable to assess the bias in selection of the reported results. For the remaining study16 we did find a conference abstract outlining the research protocol, based on which we rated bias in selection of the reported results as low. Table 3 summarises our risk of bias ratings for the selected studies according to the seven biases included in the ROBINS-I tool.
Risk of bias assessment according to the seven biases included in the ROBINS-I tool
Discussion
In this review we found that of the relatively few pregnant persons who followed up after receiving harm reduction counselling, most induced an abortion using misoprostol, and did so with extremely low complication rates. Where reported, patient satisfaction with this approach appeared to be high, and misoprostol appeared easy to obtain, mostly from pharmacies. Abortion completion and uterine aspiration rates, where reported, varied widely.
Although these results are limited by the quality of the studies included, they do align with previous studies which have reported on the overall safety and high patient satisfaction rates with medical abortion. It is well known that complication rates from medical abortion are low,18 19 even when misoprostol is used without mifepristone,20 as was the case in the four studies included in this review. Patient satisfaction tends to be high after abortion in general, regardless of whether the abortion is medical or surgical.21 When it comes to medical abortion, satisfaction is high regardless of the means by which the care is provided – in-person or telemedicine22 23 – or the type of provider.17
Harm reduction counselling as implemented in these studies is one of several strategies that have been used to support pregnant persons seeking abortion in legally or otherwise restrictive contexts. While this review focused on counselling by healthcare providers, other strategies exist, including hotlines,6 7 smartphone interventions,24 accompaniment networks25 and community-based distribution of misoprostol.9 The evidence base for most of these strategies appears to be limited, in part because many are implemented at the grassroots level rather than in academic circles, and in part because it is difficult to engage abortion patients in research, particularly in legally restrictive settings.26 This leads to high lost to follow-up rates, as we found in all the studies included in this review. A systematic review of telemedicine for medical abortion similarly reported high lost to follow-up rates (up to 57%) in the included studies. The authors commented that users who are lost to follow-up may have lower complication rates, and that studies conducted among patients who are accessing healthcare outside the formal health sector will inevitably have high attrition rates.22 Their conclusions are relevant for this review of harm reduction counselling, and we similarly caution policymakers to consider the best available evidence despite its limitations.
Another limitation of these studies is that there was significant heterogeneity in terms of how abortion completion was assessed. One study used an evidence-based questionnaire for self-assessment16 while another used a “medical examination”,15 and the remaining two did not specify if and how this outcome was assessed. Also, uterine aspiration rates were not universally reported. Where they were, they varied from 6% to 22%.15 16 The 22% aspiration rate is higher than what would be expected based on the reported efficacy of the misoprostol alone regimen for early medical abortion as reported in large clinical trials (84%–85%).27 Other studies have previously reported that aspiration rates for women who access telemedicine services for abortion vary according to their region of residence, with women in Latin America reporting high aspiration rates, even in the absence of symptoms.28 29 That the aspiration rate in Tanzania was significantly lower (6%) is an encouraging finding,15 suggesting that the need for uterine aspiration following harm reduction counselling and subsequent medical abortion may in fact be low. However, these results require further investigation.
Finally, the lack of comparison groups in these studies limit what can be said about harm reduction counselling’s ability to reduce the risks of unsafe abortion. However, given that all of these studies were conducted in legally restrictive settings, the lack of a comparison group is understandable as no comparison group could have been accessible or ethically included in research. A few articles which did not meet the study design inclusion criteria for this review describe nationwide decreases in maternal mortality rates (and particularly maternal mortality due to unsafe abortion) in Uruguay and Argentina, which coincided in time with the widespread implementation of harm reduction counselling for abortion.11 12 This finding is promising, but the implementation of harm reduction approaches cannot be isolated from other interventions which may also have contributed to a decrease in mortality due to unsafe abortion, such as the increase in availability of misoprostol and the use of telemedicine and telephone hotline services for medical abortion.29 30
Given the methodological limitations we found in the studies included in this review, we recommend a few strategies to improve the quality of the evidence in future studies on this topic. First, researchers should consider recruiting and following up with participants using various modalities, including smartphone applications or text messaging.26 Financial or other incentives may help improve follow-up rates where deemed ethically appropriate. Finally, researchers should report on study outcomes that are listed in the core outcome set for abortion research,31 and clearly outline how the outcomes are assessed.
Conclusions
Based on a synthesis of limited evidence with serious methodological limitations, provision of harm reduction counselling to pregnant persons seeking induced abortion seems to be highly acceptable to service users, and the reported complication rates are low. Ultimately, harm reduction counselling lies on a spectrum that goes from traditional clinician-directed, in-person care to complete self-management of medical abortion. Much like hotlines, pharmacist training, and community-based distribution of misoprostol, this strategy aims to provide some support to patients whose access to abortion would otherwise be limited. The available evidence does not allow us to compare harm reduction counselling to these other strategies that could be adopted in similarly restrictive settings. However, it does suggest that harm reduction counselling can safely be considered, particularly by clinicians who wish to provide some support to pregnant persons seeking induced abortion but are constrained by local laws and regulations.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the development of the review protocol. BMS performed the systematic search. BMS and RG assessed the studies for eligibility and conducted the risk of bias assessment. BMS performed the main analysis and wrote the first draft of the manuscript. RG and CRK contributed to the interpretation of the results and the revisions of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.