Article Text

Abstract
Background Understanding predictors of pain with gynaecological procedures may facilitate individualised counselling and pain management. We aimed to study the effect of dysmenorrhoea on intrauterine device (IUD) insertion pain.
Methods This was a planned secondary analysis of a randomised trial evaluating self-administered lidocaine gel versus placebo for IUD insertion pain. We included those participants who reported menses in the past 3 months. We assessed dysmenorrhoea (in the past 3 months) and procedural pain using a 100 mm visual analogue scale (VAS). We categorised dysmenorrhoea as none/mild (<40 mm), moderate (40–69 mm) or severe (≥70 mm). We assessed participant pain scores at speculum insertion, tenaculum placement, IUD insertion, and overall. We compared median procedural pain scores by dysmenorrhoea group with three-way and post hoc pairwise analyses.
Results We analysed 188 participants. Demographic characteristics were similar among the three dysmenorrhoea groups. Pairwise comparisons revealed higher median procedural pain scores in the severe dysmenorrhoea group compared with the none/mild dysmenorrhoea group at speculum insertion (25 mm vs 8 mm; p=0.007), tenaculum placement (51 mm vs 31 mm; p=0.04) and IUD insertion (74 mm vs 61 mm; p=0.04). Overall pain did not differ among the three groups (p=0.32).
Conclusions Patients with severe dysmenorrhoea experienced increased pain with all aspects of IUD insertion, including speculum and tenaculum placement, compared with those with only mild or no dysmenorrhoea. Clinicians may consider this finding when providing individualised counselling and pain management for patients undergoing IUD insertion and other gynaecological procedures. Larger studies are needed to validate the effect of dysmenorrhoea severity on pain throughout IUD insertion.
- contraceptive devices
- female
- counseling
- family planning services
- intrauterine devices
- long-acting reversible contraception
- patient reported outcome measures
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article.
Statistics from Altmetric.com
- contraceptive devices
- female
- counseling
- family planning services
- intrauterine devices
- long-acting reversible contraception
- patient reported outcome measures
Key messages
Severe dysmenorrhoea appears to be a risk factor for increased pain with all aspects of intrauterine device (IUD) insertion, including speculum and tenaculum placement.
This finding may assist clinicians in providing individualised counselling and pain management for patients with dysmenorrhoea undergoing IUD insertion and other gynaecological procedures.
Introduction
Intrauterine devices (IUDs) provide a highly safe and effective means of long-term, reversible contraception, and the American College of Obstetrics and Gynaecology recommends IUDs as a first-line option for contraception.1 Unfortunately, fear of pain with insertion remains a significant barrier to their use.2
Understanding predictors of IUD insertion pain may assist clinicians in providing individualised counselling and pain management. In a recent randomised controlled trial examining the effectiveness of self-administered vaginal lidocaine gel for IUD insertion pain,3 we identified dysmenorrhoea to be an independent predictor of pain with IUD insertion in a regression model, a finding consistent with other literature.4–7 The physiological basis by which dysmenorrhoea could exacerbate IUD insertion pain involves uterine hypercontractility, changes in uterine blood flow, and increased central nervous system response to pain.8 The 52 mg levonorgestrel intrauterine system (LNG-IUS) provides the non-contraceptive benefit of reducing menstrual pain, making it an ideal method for individuals with primary and secondary dysmenorrhoea.9 Gaining a better understanding of dysmenorrhoea as a risk factor for IUD insertion pain and finding an adequate pain control method for this population is therefore of the utmost importance.
The objective of this study was to determine the effect of dysmenorrhoea on pain experienced at various time points during the IUD insertion procedure.
Methods
We conducted a secondary analysis of a blinded, randomised controlled trial evaluating the effectiveness of self-administered lidocaine gel versus placebo at reducing IUD insertion pain.3 This secondary analysis was planned prior to patient recruitment, and dysmenorrhoea data were therefore collected upon study enrolment.
The methods of the primary study have been detailed previously.3 Briefly, we recruited patients 18 years of age or older undergoing LNG-IUS or copper IUD insertion in an outpatient setting between June 2016 and April 2017. Study approval was granted by the Stanford University Institutional Review Board (IRB-32825) and written informed consent was obtained from all participants prior to enrolment. We excluded participants who had an allergy to lidocaine, had a known uterine anomaly, had a history of cervical surgery, had taken misoprostol prior to their procedure, or who requested sedation or narcotic analgesics. Prior IUD use was not an exclusion criterion, and those participants undergoing IUD removal and reinsertion were included in the study. Similarly, we did not exclude participants who had used an alternative hormonal contraceptive method in the months leading up to the study.
For the present analysis, we included those participants who reported having a menstrual period in the past 3 months. Study coordinators administered a baseline questionnaire to collect demographic data, obstetric history, and a detailed menstrual history. They asked participants about the heaviness of menstrual bleeding, associated symptoms, need to take time off from work or school, need for pain medication, and duration of bleeding and dysmenorrhoea over the past 3 months. Participants were also asked whether they had previously received a diagnosis of dysmenorrhoea and whether they had ever received a recommendation to use an IUD for dysmenorrhoea. The study coordinators then asked in a standardised fashion “How much pain, on average, did you experience with your periods in the last 3 months?”. Participants rated the severity of their dysmenorrhoea on a 100 mm unmarked visual analogue scale (VAS) (0 being “no pain” and 100 being the “worst pain imaginable”). We then defined none/mild dysmenorrhoea as <40 mm, moderate dysmenorrhoea as 40–<70 mm and severe dysmenorrhoea as ≥70 mm. We chose these cut-off points based on prior literature that defined pain severity based on patient perception of pain and the amount of analgesic required to obtain pain relief.10–12
Using the same 100 mm VAS scale, participants were asked to rate their pain level at multiple time points throughout the IUD insertion procedure. Our primary outcome was pain at the time of IUD insertion, measured immediately after speculum removal; participants were asked “How was pain with insertion?” in a standardised fashion. Secondary outcomes included anticipated pain (measured immediately after gel insertion), baseline pain (measured immediately prior to the start of the procedure), pain with speculum insertion, pain with tenaculum placement, and overall pain (assessed post-procedure). These represent the same primary and secondary outcomes reported in the original trial.3
We recorded all participant data and VAS scores on an electronic tablet using Research Electronic Data Capture (REDCap) tools hosted at the Stanford Center for Clinical Informatics.13 We performed statistical analysis using IBM SPSS Statistics, version 25.0 (IBM Corp., Armonk, NY, USA). We set the statistical significance level at an alpha of 0.05 for all analyses. Given the non-normal distribution of VAS scores for pain, we analysed medians. The primary study was not powered to evaluate the association between dysmenorrhoea severity and IUD insertion pain; as such, this secondary analysis was not adequately powered to evaluate our stated objective, and this is therefore an exploratory paper.
We analysed baseline demographic and clinical characteristics among the three dysmenorrhoea severity groups using chi-square or Kruskal–Wallis tests where appropriate. Before pooling randomisation groups from the original trial for our secondary analysis, we conducted a two-way MANOVA to test for an interaction effect between randomisation group and dysmenorrhoea group. We also used the Mann–Whitney U test to assess whether the efficacy of lidocaine gel, as evaluated in the primary study, differed by dysmenorrhoea group. For each procedure time point, we compared median VAS scores among the three dysmenorrhoea groups using the Kruskal–Wallis test. We then performed pairwise analyses for all significant findings using the Dunn post hoc test with the Bonferroni correction for multiple comparisons.
Patient and public involvement
There was no involvement of patients or the public in the design or conduct of this study.
Results
We assessed 276 patients for eligibility for the primary study. We enroled 220 participants and included 215 in the primary analysis. Of these, 188 reported menses in the past 3 months and were therefore eligible for our secondary analysis (figure 1).
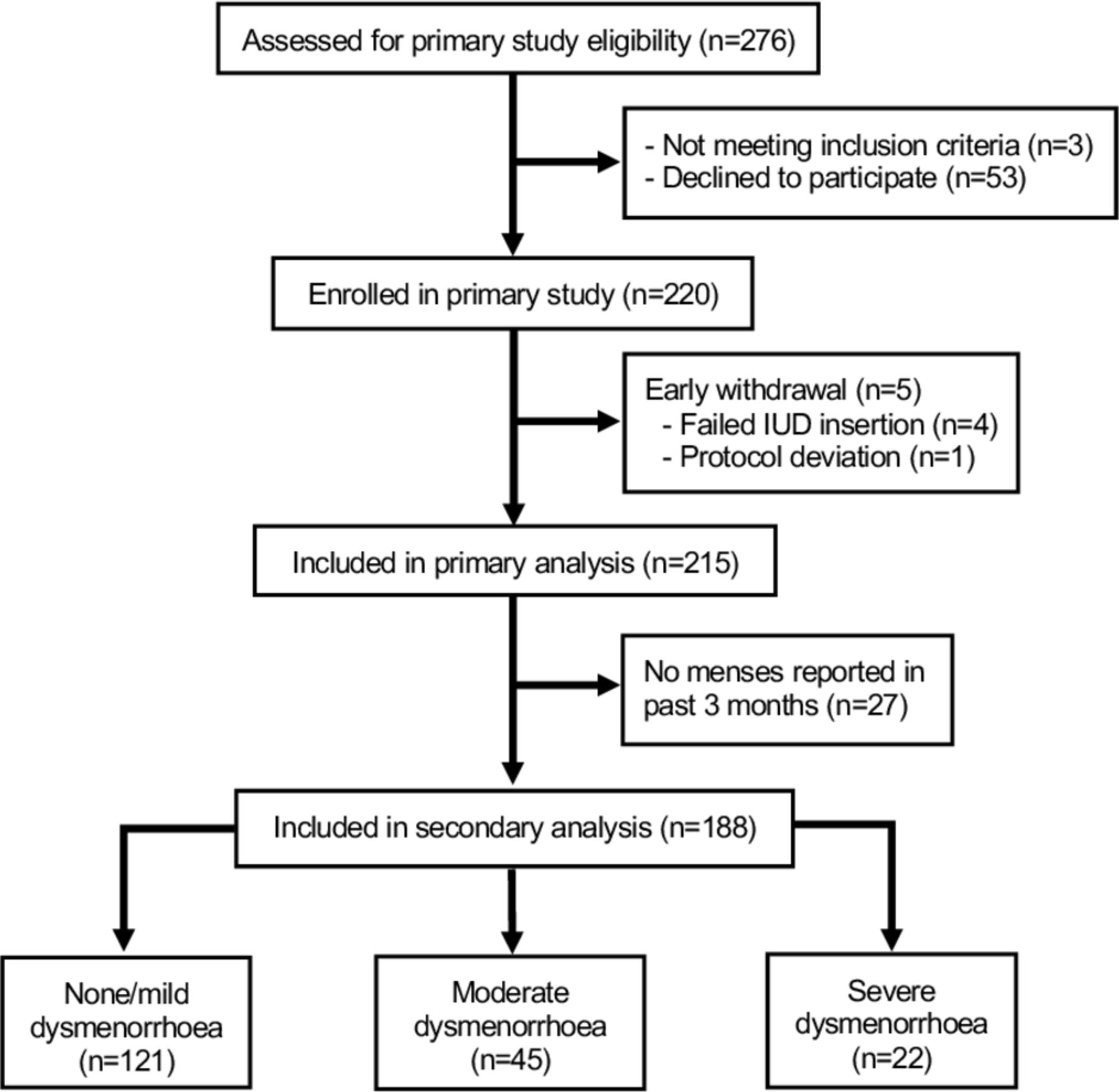
Flow of participants. IUD, intrauterine device.
Of those included in the secondary analysis, the majority (64.4%) reported dysmenorrhoea scores in the none/mild range, whereas 23.9% and 11.7% reported moderate and severe dysmenorrhoea, respectively. There were no significant differences in baseline demographic characteristics among the three dysmenorrhoea groups (table 1). Participants with increasingly severe dysmenorrhoea were more likely to report heavy bleeding and associated menstrual symptoms. Of those in the severe dysmenorrhoea group, 36.4% were recommended to use the LNG-IUS to treat their dysmenorrhoea (table 1).
Baseline demographic and menstrual characteristics of participants
In the primary study, self-administered lidocaine gel did not reduce pain with IUD insertion compared with placebo3; similarly, recognising lack of power, we found no benefit of lidocaine gel versus placebo when stratified by the three dysmenorrhoea groups. Two-way MANOVA showed no interaction between randomisation group and dysmenorrhoea group for IUD insertion pain (p=0.64). We therefore pooled participants in the lidocaine and placebo groups for our intended secondary analysis.
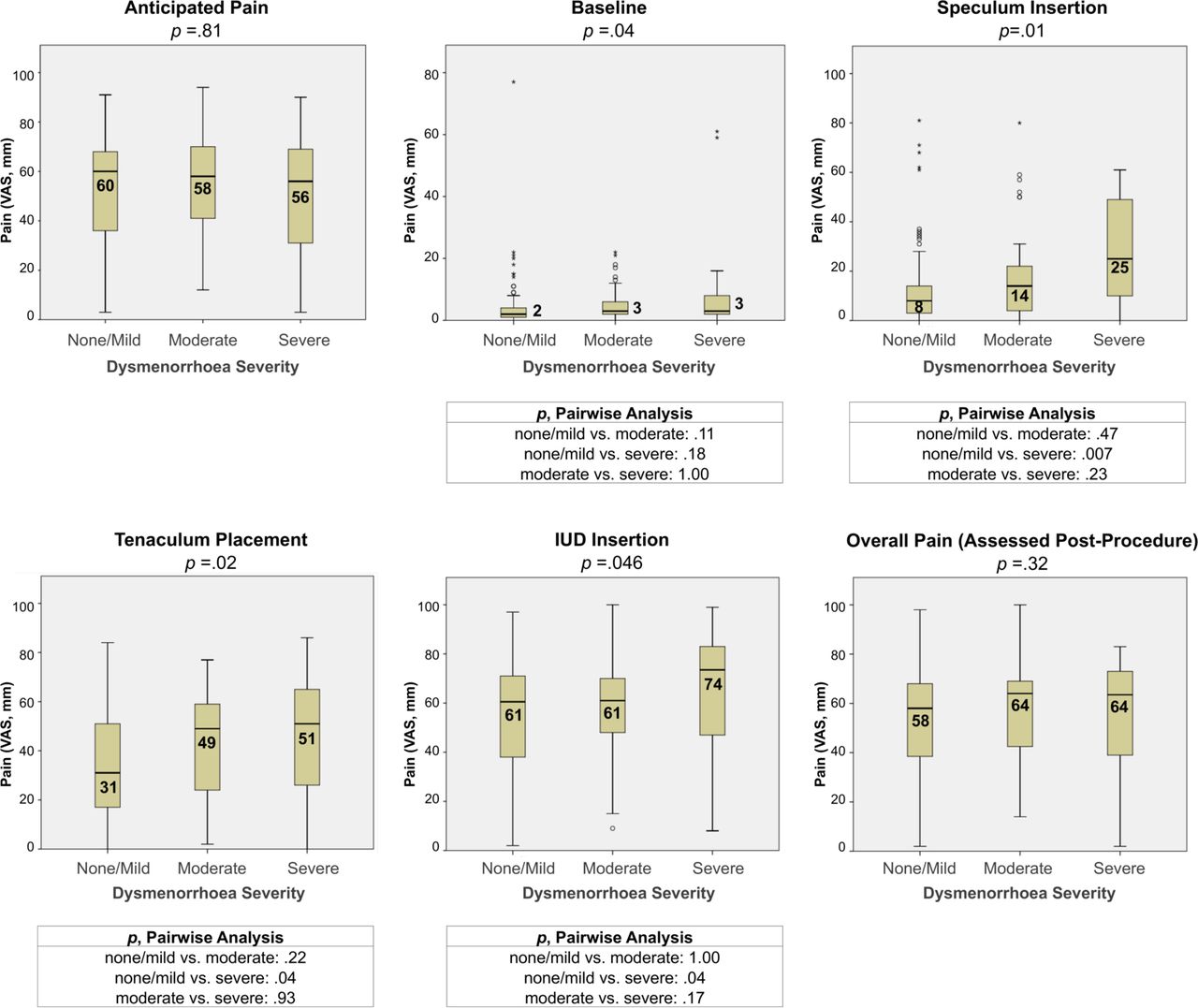
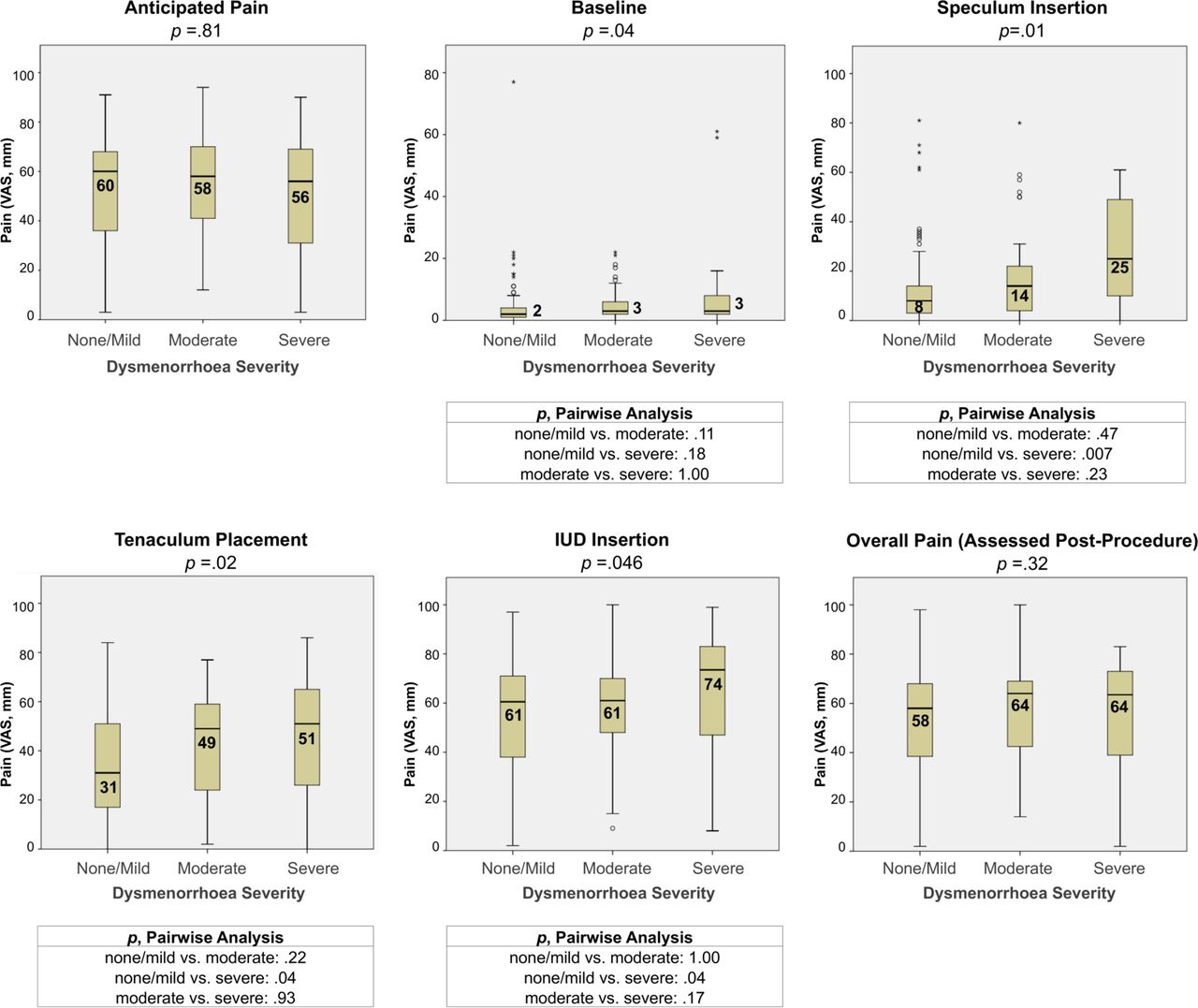
Three-way comparisons revealed statistically significant differences in median VAS scores by dysmenorrhoea group at baseline (p=0.04), speculum insertion (p=0.007), tenaculum placement (p=0.02) and IUD insertion (p=0.046) (figure 2). Further pairwise analysis revealed higher median procedural pain scores in the severe dysmenorrhoea group compared with the none/mild dysmenorrhoea group at speculum insertion (25 (range 0–61) mm vs 8 (0–81) mm; p=0.007), tenaculum placement (51 (0–86) mm vs 31 (0–84) mm; p=0.04) and IUD insertion (74 (8–99) mm vs 61 (2–97) mm; p=0.04) (figure 2). Although we observed a statistically significant difference for baseline scores overall, it was not clinically significant and was not maintained with pairwise analysis. VAS scores among the three dysmenorrhoea groups were similar for anticipated pain and overall pain.
{kind=link}
{kind=link}
Boxplots of median pain scores (VAS, 0–100) at various procedure time points by dysmenorrhoea severity. Three-way comparisons were performed using the Kruskal–Wallis test. Pairwise comparisons were performed for significant findings using the Dunn post hoc test with Bonferroni correction. IUD, intrauterine device; VAS, visual analogue scale.
Discussion
This secondary analysis adds to the growing body of evidence that dysmenorrhoea is a risk factor for pain with IUD insertion.4–7 Furthermore, we found that dysmenorrhoea was a predictor of increased pain at other procedure time points—speculum insertion and tenaculum placement—an important finding that may be relevant to other gynaecological procedures. At each step of the IUD insertion procedure, we observed that those with severe dysmenorrhoea (as defined by a score of at least 70 mm on VAS) were more likely to experience increased pain compared with those without dysmenorrhoea or only mild dysmenorrhoea (less than 40 mm on VAS). Interestingly, dysmenorrhoea was not found to be a significant predictor of “overall pain”, as measured in our post-procedure questionnaire. Ultimately, this recalled pain may be more relevant to a patient’s overall satisfaction with the procedure.
Individuals who suffer from dysmenorrhoea have unique physiological factors that may also predispose them to pain with IUD insertion. Dysmenorrhoea is associated with enhanced prostaglandin release leading to increased basal uterine tone, increased active uterine pressure, and uncoordinated uterine contractions.8 It is also associated with differences in uterine blood flow and steroid hormone biosynthesis.8 14–16 Furthermore, individuals with dysmenorrhoea have been shown to have a heightened sensitivity to pain both within and outside areas of referred menstrual pain, even during non-painful phases of the menstrual cycle.8 Repeated monthly painful menses may lead to changes in the central processing of noxious stimuli, or “central sensitisation”, resulting in hyperalgesia in the absence of any tissue injury or inflammation.8 17 Notably, this provides a mechanism by which those with severe dysmenorrhoea in our analysis experienced increased pain with speculum insertion. Given the results of our analysis, it is possible that individuals with severe dysmenorrhoea could experience more discomfort with all gynaecological procedures involving a speculum, tenaculum or instrumentation of the uterus with any device similar to an IUD inserter.
The amount of pain experienced with IUD insertion is highly variable and difficult to predict. In addition to dysmenorrhoea, factors that have been identified as predictors of increased IUD insertion pain include nulliparity,4 6 18 19 increased interval since last pregnancy4 20 or last menses,18 absence of current breastfeeding,18 20 the LNG-IUS (vs the copper IUD),6 19 age >30 years18 and anticipated pain.3 4 6 19 With a better understanding of these risk factors, providers have an opportunity to individualise their approach to counselling patients on what to expect with the procedure. Consensus recommendations presented in 201421 highlight the importance of anticipatory counselling as a non-pharmacological intervention for improving a patient’s overall experience with IUD insertion. Reducing uncertainty through effective counselling may alleviate pre-procedure anxiety,22 which itself has been shown to correlate with increased IUD insertion pain.23
As effective pain management options for IUD insertion become routinely available, providers may be more inclined to recommend such methods to patients with dysmenorrhoea and other risk factors for IUD insertion pain. Finding an adequate method of pain control for IUD insertion is of key importance for patients with dysmenorrhoea, especially since the LNG-IUS may eventually improve their menstrual symptoms.9 In our cohort, over one-third of participants in the severe dysmenorrhoea group had been recommended to use the LNG-IUS to treat their dysmenorrhoea. It is plausible that individuals with dysmenorrhoea, given their unique physiological characteristics, could respond more or less favourably to certain analgesic interventions. Our primary study did not demonstrate a reduction in IUD insertion pain with 2% lidocaine gel,3 and dysmenorrhoea severity did not alter the efficacy of this intervention. As research in IUD insertion pain management continues, studies should consider evaluating whether their analgesic interventions are beneficial for those with dysmenorrhoea. For instance, recent trials have demonstrated promising reductions in IUD insertion pain with a 1% lidocaine paracervical block and a 2% lidocaine intracervical block among nulliparas24–26; it would be valuable to examine whether these results are applicable to individuals with dysmenorrhoea (notably excluded from one of the studies), and whether the block itself causes more pain among this population.
Our analysis has multiple strengths. Our sample included both nulliparous and parous participants receiving all five types of IUDs currently approved for use in the United States. Another strength of our study is our categorisation of dysmenorrhoea severity into three groups using a 100 mm VAS (<40 mm=none/mild; 40–<70mm=moderate; ≥70mm=severe). The definition of dysmenorrhoea is vague, and there are currently no standardised methods for assessing dysmenorrhoea severity.8 Similarly, there are no universally accepted cut-off points to define mild, moderate and severe pain on VAS, and those used in the dysmenorrhoea literature are often arbitrary and inconsistent. After conducting an exhaustive review of the VAS literature, we chose our cut-off points based on studies that correlated pain scales with patient perception of pain severity10 as well as the amount of analgesic required for pain relief.11 12 Among the severe dysmenorrhoea group, menstrual characteristics reflected a significant impact on daily life, as would be expected for this population; a substantial proportion reported associated nausea (45.5%), vomiting (22.7%) and headaches (50.0%) with their menses, 45.5% reported needing to take time away from work or school, and 95.5% reported taking pain medication for their periods.
Our study is limited by the fact that our sample was comprised of mostly white nulliparas with a normal body mass index, and thus is not generalisable to large portions of the United States population. Another limitation is that our analysis does not distinguish between primary and secondary dysmenorrhoea, a distinction that is worth exploring in future studies. Finally, we did not power our original randomised trial to evaluate the association between dysmenorrhoea severity and IUD insertion pain; we would have required a much larger sample size to be adequately powered for the three-arm comparison within our secondary analysis. Of note, our severe dysmenorrhoea group only included 22 participants (11.7% of the total sample). If adequately powered, we may have detected additional statistically significant differences in our pairwise analyses. While our study suggests that dysmenorrhoea severity has a clinically significant effect on pain throughout IUD insertion, larger studies are needed to validate this concept.
In summary, we found that severe dysmenorrhoea was a risk factor for increased pain with all aspects of IUD insertion, including speculum and tenaculum placement. This information may aid clinicians in providing more personalised counselling and pain management to patients undergoing IUD placement and other gynaecological procedures. Future research should consider the effect of dysmenorrhoea on interventions targeted at decreasing gynaecological procedural pain.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors RS, KL, JC and KS all contributed to the study design. RS and KL were responsible for data collection and analysis.
Funding This work was supported by the Society of Family Planning Research Fund (Award SFPRF16-27) and the Stanford University School of Medicine Medical Scholars Fellowship Program.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.