Article Text

Abstract
Background Unsafe abortion is an important public health problem in Ghana, making significant contributions to the morbidity and mortality of reproductive-aged women. Although mostly used in explaining mortality associated with perinatal care, recent calls for research on induced abortion in Africa suggest that the Three Delays Model could be used to enhance understanding of women’s experiences and access to induced abortion care.
Methods We conducted 47 face-to-face interviews with women who had experienced unsafe abortions, with formal abortion providers (abortion providers in hospitals) and with informal and non-legal abortion providers (pharmacy workers and herb sellers). Study participants were recruited from selected hospitals, community pharmacies and markets within the Ashanti region of Ghana. We drew on phenomenology to analyse the data.
Findings The first delay (in seeking care) occurred because of women’s poor knowledge of pregnancy, the influence of religion, and as a result of women underestimating the seriousness of abortion complications. Factors including cost, provider attitudes, stigma, and the proximity of pharmacies to women’s homes delayed their access to safe abortion and resulted in their experience of the second delay (in reaching a healthcare facility). The third delay (in receiving appropriate care) was a result of hospitals’ non-prioritisation of abortion complications and a shortage of equipment, resulting in long hospital waiting times before treatment.
Conclusion This study has shown the value of the Three Delays Model in illustrating women’s experiences of unsafe abortions and ways of preventing the first, second and third delays in their access to care.
- qualitative research
- abortion
- induced
Data availability statement
No data are available. Not applicable.
Statistics from Altmetric.com
Key messages
Despite abortions being legally permissible, Ghanaian women mainly obtain abortions outside the formal health delivery system using unsafe methods.
Various individual, community and societal factors act as barriers, delaying Ghanaian women’s access to safe abortion care within the formal health delivery system.
The Three Delays Model can be used as a framework for understanding these delays experienced by women in accessing abortion care.
Introduction
In Africa, 8.3 million abortions occur annually, with African women experiencing the highest risk of induced abortion-related mortality than women anywhere in the world.1–3 Based on current estimates, some 16 000 African women die each year from unsafe abortion-related complications, and an estimated 1.6 million women experience morbidities as a consequence of unsafe abortions.4 In Ghana, legal abortions are allowed in cases of rape, incest, fetal anomalies, and to protect the physical or mental health of the pregnant woman; this notwithstanding, unsafe abortion is a significant public health problem.5–7
Formal Ghanaian healthcare is mainly provided by the Ghana Health Service and healthcare delivery is structured into primary, secondary and tertiary care.8 However, access to safe abortion care in these facilities is not readily available.9 In a national study on maternal health including induced abortions, the majority of women were reported to have ended their pregnancies outside the formal health system with medical abortifacients containing either misoprostol alone or a combination of misoprostol and mifepristone.7
While Ghanaian research has presented women’s abortion experiences,7 10 there is limited evidence from Ghanaian abortion providers, including pharmacy workers and herb sellers. Given the role providers play (formal and informal) in abortion safety, and women’s experience of delays, an exploration of their perspectives is important.
The Three Delays Model has been used to explain maternal mortality related to perinatal care, but not with induced abortions.11 The model proposes that delays experienced in deciding to seek healthcare, reaching a healthcare facility, and receiving appropriate care are important contributory factors to maternal mortality.11 Recent calls for a research agenda on induced abortion have suggested that using the Three Delays Model and exploring specific populations, such as healthcare providers, could enhance our understanding of women’s unsafe abortions.12
This article, from a wider study exploring providers’ and women’s unsafe abortion experiences, aims to provide evidence for the utility of the Three Delays Model as a framework for understanding women’s experiences of unsafe abortion in Ghana.
Methods
We conducted the study in the Ashanti region of Ghana, the most populous region, with significant prevalence of induced abortions.7 13 Women and formal abortion providers were recruited from three hospitals. Informal abortion providers (pharmacy workers and herb sellers) were recruited from eight pharmacies and three markets within the wider community between June 2017 and March 2018.
Women were eligible for the study if aged between 18 and 49 years and reporting to participating hospitals after complications from unsafe abortions. The single inclusion criterion for abortion providers was abortion provision.
We utilised purposive sampling in recruiting women and formal abortion providers from the hospitals. In recruiting the women, advertising materials were placed on notice boards and at vantage locations within hospitals. Study materials were also left with healthcare workers, who advised women meeting the inclusion criteria about the study. Women who expressed interest in participating were approached by the lead researcher (MNAO). Only women treated and ready for discharge were enrolled in the study to avoid situations in which women felt their participation could influence care. The lead researcher explained the purpose of the study and sought both verbal and written consent. Participants were made aware of the voluntary nature of participation and all underwent a confidential interview in Twi (the local language) using an interview guide (online supplemental file 1).
Supplemental material
Formal abortion providers were recruited through one-on-one promotion of the study. Following explanation of the voluntary nature of participation and consent, confidential interviews with providers were conducted after their hospital shift (online supplemental file 2).
Supplemental material
With informal abortion providers, due to the sensitivities surrounding illegal activities, initial attempts at recruitment failed. MNAO therefore recruited a respected community leader who facilitated the process to reach these individuals.14 After initial informal abortion provider interviews, we used a ‘snowballing’ technique to recruit the remainder of the sample (online supplemental files 3 and 4).
Supplemental material
Supplemental material
We used thematic semi-structured interview guides. Interviews were a one-off encounter and interviewees were assured that data were stored confidentially and in an anonymous form. Participants were further assured that their location would not be identified. Each interview lasted between 30 and 75 min and was conducted and audio-recorded by the lead researcher in Twi, the local language. Both verbal and written informed consent were obtained.
This qualitative study drew on phenomenology, which studies patterns of peoples’ lived experience and how they have explained it, to enable detailed analysis of participants’ abortion experiences.15 Data analysis commenced with cleaning and transcribing of interviews into English. Coding was an inductive process during which the research team read and re-read the interview transcripts to generate and finalise codes for onward categorisation.15–17 To validate and enhance a more comprehensive understanding of unsafe abortion, we triangulated the data of women with providers (formal and informal).17 During data analysis, the research team identified women experiencing delays in their decision to seek, reach and receive care after unsafe abortions, for which we found the Three Delays Model a good fit to explain what was occurring. All names used in this article are pseudonyms.
Results
Participant characteristics
We interviewed 47 participants: 24 women mostly from low-income households and employed in their own small businesses, 10 formal abortion providers who were mainly midwives and 13 informal abortion providers, comprising eight pharmacy workers and five herb sellers (tables 1 and 2).
Characteristics of women seeking care following informal abortions (n=24)
Characteristics of abortion providers (n=23)
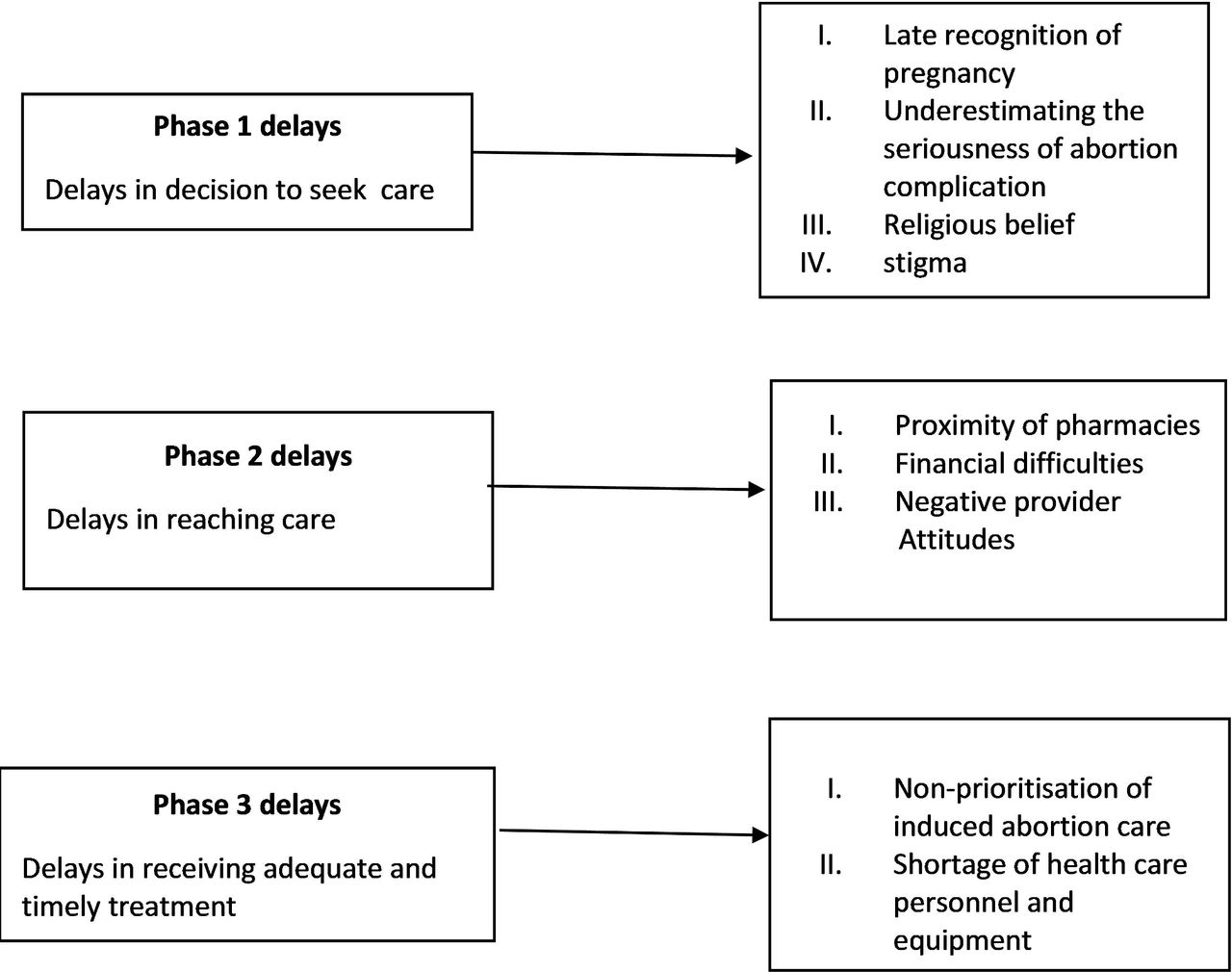
We present the results of the study highlighting the first, second and third delays women experienced in their unsafe abortion journey. All delays represented in figure 1 emerged from the experiences of the women in this study.

{kind=link}
The Three Delays Model applied to unsafe abortion prevention.
First delay
In this study, women experienced the first delay when they delayed their decision to seek abortion or post-abortion care due to late recognition of pregnancy, underestimating the seriousness of an abortion complication, and concerns about suffering stigma from breaching religious norms. Women’s poor knowledge about reproductive health led to delayed testing and late recognition of pregnancy signs, resulting in abortions at higher gestations, with greater risks to the lives and health of women. Patricia delayed her decision to seek abortion care because she did not recognise she was pregnant until her pregnancy was well advanced:
… I used to get tired easily, but I thought it was because of the kind of work I did … I also noticed that the number of days I menstruated had reduced from 7 days to 3 days, but I did not think it was pregnancy… [Patricia, aged 44 years]
Similarly, other women spoke of delays in their decision to seek care due to poor education around pregnancy:
… the pregnancy resulted from my first sexual intercourse; I did not know I could get pregnant the first time. [Leticia, aged 19 years]
After undergoing an unsafe abortion using a herbal abortifacient, Juliana thought the bleeding she was experiencing would resolve on its own and hence delayed seeking care till her situation worsened:
… abortion occurred after using herbs. … the blood was still coming. I thought it was normal and would resolve on its own. … fainted and was brought here. … they told me I was anaemic and there were still some products of conception. … they evacuated it at the theatre. [Juliana, aged 24 years]
The strong influence of religion also caused delays in women’s decision to access care:
… Most of our women know that they can come to the hospital for safe abortion, but they would not, with our Christian life. We think we are so Christian that the thing is wrong. [‘Aunty’ Vida, midwife]
Second delay
The second delay in this study is defined by difficulties in reaching care. Financial difficulties, stigma, prejudice, power imbalance, local pharmacy access and patriarchal attitudes contributed to women’s experience of the second delay. Women’s financial resources played an important role in their experience of this delay: the inability to pay for safe abortion was a barrier to care, resulting in abortions at higher gestations and reliance on inexpensive unsafe methods:
… he gave me fifty cedis … it was not enough … I bought an abortifacient from the market. [Beatrice, aged 28 years]
… the herbs are not expensive but very efficacious … many buy. [‘Sister’ Gifty, herb seller]
… she will sit at home and save till she gets the two hundred cedis or use an unsafe means which is cheaper. [‘Aunty’ Mary, midwife]
Because pharmacy provision is illegal and unregulated, pharmacy workers could adjust the costs as they please:
… usually, I look at the person coming to buy if they appear rich… I increase the price a bit. [Bra George, pharmacy shop assistant]
Women denied access to care due to poverty may not only experience delays but could also die:
It was after she died that the sonographer working with us mentioned that the girl came to enquire from him the cost of an abortion. … she had only thirty cedis … he told her to go and raise the additional money and then come. Since the girl could not raise the extra money, she opted for the cheaper option which led to her death. [‘Aunty’ Charlotte, midwife]
Women also delayed reaching the formal health system due to the ease of local pharmacy access:
… they go to the pharmacy to buy medicines rather than … the hospital. … pharmacy it is fast you buy, and you are off unlike the hospital where you have to be registered and wait your turn to see the doctor. [Dr John, general practitioner]
… I told the person … at the pharmacy I wanted medabon and he brought it. I paid and left; he did not ask any questions. [Sarah, aged 21 years]
Though without training, some pharmacy workers took it upon themselves to treat women with complications, an act which delayed women from accessing hospital care:
… I tell them that if the bleeding is usually long … they should come back so I give them something to stop the flow. [‘Bra’ Josh, pharmacy shop assistant]
Third delay
The third delay occurred when women arrived at the hospital with post-abortion complications. Women sometimes reported waiting for very long periods because of negative provider attitudes, stigma or abortion being treated as the lowest priority in obstetric care. This sometimes led to situations whereby women with life-threatening complications were not treated as an emergency and were made to undergo cumbersome administrative processes:
… I was bleeding all this while … but was not attended to until my husband did the paperwork … when he finished a nurse sent me to the ward and administered IV fluids. I was very weak I bleed so much. … you see how white my palms have become it is now even better. [Patricia, aged 44 years]
There are also instances where women experienced delays after reporting to hospitals for treatment due to limited supply of equipment:
… the doctor wanted me admitted at the ward but there were no beds… [Matilda, aged 31 years]
Discussion
As far as we are aware, this is the first study to use the Three Delays Model in relation to induced abortion care.11 The model proposes that abortion-related maternal morbidity and mortality can be classified in terms of delays in seeking, reaching and receiving appropriate treatment at health facilities.11 Our study, conducted in the Ashanti region of Ghana, illustrated that interwoven factors within women’s individual level of education, together with their communities and wider structural environment, contributed to the first, second and third delays. As this research involved only women who sought hospital care after experiencing abortion complications, it may not be representative of all women seeking abortion. Community-based studies could further enhance an understanding of the delays experienced by women and explore differences in abortion provision by herb sellers and pharmacy workers.
Many women who participated in this study did not recognise the signs of pregnancy until their pregnancies were more advanced, at which point terminating the pregnancy not only carried greater health risks but was also more expensive. Though available evidence suggests that adolescents are more likely to delay abortions due to late recognition of pregnancy,18 in this study women who had experienced a number of pregnancies and births also delayed accessing care due to late recognition of pregnancy.
Despite pharmacy provision of medical abortion being illegal in Ghana, a significant number of women in the study used it. Like other low-resourced settings, women who accessed pharmacy abortions were either given no or limited information on the safe use of the abortifacients.19 20 Though available evidence highlights the contribution of pharmacy provision of medical abortion to maternal mortality reduction,21 22 inadequate information about the safe use of these abortifacients could result in incorrect dosages and unsafe abortions.23 Additionally, pharmacy workers in this study described providing on- and off-label treatment to women with complications. This is not only inimical to women’s lives as pharmacy workers are not trained in this management, but could delay sick women from accessing appropriate care promptly. This indicates a need for legalisation around pharmacy supply; in this way pharmacy workers can be given the necessary training to safeguard the lives of women and be monitored for safe and effective practice.
Despite prompt treatment being a major determinant of the health outcomes after unsafe abortion,24 medical care for women with abortion complications in hospitals was not deemed urgent. Their delayed care may reflect healthcare provider and wider societal attitudes towards women who abort their pregnancies. Evidence of obstetric violence25 and the mistreatment of women seeking treatment for abortion complications has been reported in Ghana and elsewhere.24 26 Delayed access to treatment may have also been influenced by limited healthcare equipment and personnel.27
Conclusion and recommendations
This study explored the applicability of the Three Delays Model in studies on unsafe induced abortions and enhanced understanding of ways in which women’s abortion experiences impacts their access to care. This study was conducted in Ghana and may therefore not reflect the pattern of delays experienced by women in other settings. Negotiating access to discussions on abortions among women and providers within the Ghanaian context where abortion is stigmatised is a major strength of this study. To help prevent unsafe abortion, there is a need for more sexual and reproductive health school-based education together with public health campaigns to equip women to make informed decisions. Campaigns targeted at reducing abortion-related stigma are also important. Pharmacy provision of medical abortions should be legalised, and its role monitored. In addition, there is a need for regular training of pharmacy workers on safe dispensing of medical abortifacients, as well as signs of abortion complications, in order to safeguard the lives and health of the women they serve. The Three Delays Model is an important framework that can be used to identify where delays occur for women seeking induced abortion care.
Data availability statement
No data are available. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the La Trobe University Human Ethics Committee (HEC17-009) in Australia and Komfo Anokye Teaching and the School of Medical Sciences, Committee on Human Ethics Research and Publication (CHRPE/AP/547/17) in Ghana.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MNAO designed and collected data for the study. Data were analysed by MNAO with input from all authors regarding interpretation of the results. MNAO prepared the first draft of the manuscript. All authors contributed to revising the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement No patients or members of the public were involved in this study
Provenance and peer review Not commissioned; externally peer reviewed.