Article Text

Abstract
Background Intrauterine devices (IUDs) are highly effective contraception. IUDs inserted directly following delivery provide immediate birth control and may decrease unintended pregnancies, including short-interval pregnancies, thereby mitigating health risks and associated economic burden.
Methods This systematic literature review included published global data on the utilisation, effectiveness, and safety of postpartum intrauterine devices (PPIUDs) of any type. English language articles indexed in MEDLINE, Embase, and Cochrane from January 2010–October 2021 were included.
Results 133 articles met the inclusion criteria (46% interventional studies; 54% observational; n=87 from lower-income countries; n=46 from higher-income countries). PPIUD use was low in higher-income countries (6/10 000 US deliveries in 2013–2016) and varied widely in lower-income countries (2%-46%). Across both higher- and lower-income countries, in most studies (79%), >80% of women with PPIUDs had an IUD in place by 3 months; at 6 and 12 months, 76% and 54% of included studies reported that >80% of women had an IUD in place; reason for discontinuation was infrequently reported. Pregnancies were rare (96 pregnancies across 12 191 women from 37 studies reporting data) and were generally unrelated to device failure, but rather occurred in women no longer using a PPIUD. Expulsions occurred mainly in the early outpatient period and ranged widely (within 3 months: 0–41%). Abnormal bleeding, infections, or perforations were rare.
Conclusions PPIUDs are safe and effective. Long-term follow-up data are limited. Future research elucidating reasons underlying lack of PPIUD use is warranted.
- long-acting reversible contraception
- intrauterine devices
- patient safety
- contraceptive effectiveness
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Intrauterine devices (IUDs) inserted early postpartum provide the advantage of immediate contraception.
Immediate postpartum contraception may decrease unintended pregnancies and short-interval pregnancies, potentially lessening both economic burden and poor maternal and infant health outcomes.
What this study adds
This systematic literature review suggests that early postpartum IUD use is effective and safe, but it is an underutilised contraceptive method in both higher- and lower-income countries.
How this study might affect research, practice or policy
Studies to further the understanding of reasons for low utilisation are warranted.
Introduction
Unintended pregnancy (UIP)1 2 rates have declined over the past three decades, decreasing from 79 pregnancies per 1000 women of reproductive age worldwide from 1990 to 1994 to 64 per 1000 women from 2015 to 2019.3 Still, approximately 121 million UIPs occur annually,3 accounting for over half of all yearly pregnancies globally.4 UIPs are associated with substantive individual and societal economic burden5 6 and disproportionately occur in low-income countries and among women of colour within the USA.3 7 Use of long-acting reversible contraception (LARC), although more effective than other forms of birth control,8 9 is also less prevalent in low- versus high-income countries7 and among African American versus white US women. Intrauterine devices (IUDs) can be inserted during a caesarean delivery or immediately following a vaginal delivery, but are typically placed 4–6 weeks post-delivery.9 10 Insertion delay mainly reflects concerns of expulsion risk. Inconsistent findings regarding expulsion risk for postpartum intrauterine devices (PPIUDs) have been reported. In two systematic literature reviews (SLRs) that included all study types, early-placed IUDs posed greater expulsion risk compared with those placed 6–8 weeks postpartum,11 12 while an earlier Cochrane meta-analysis that included randomised controlled trial (RCT) data suggested similar occurrence of expulsions for early versus later insertion.13 PPIUD insertion protects against short-interval pregnancy and attendant risk for poor maternal and birth outcomes.14 Given that prior SLRs are dated, have focused solely on expulsions,11 12 and do not include the impact of country-level economic factors on IUD use and outcomes, we sought to characterise current global evidence regarding PPIUD utilisation, safety, and effectiveness.
Methods
The SLR methodology followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidance.15 Embase, MEDLINE, and Cochrane CDSR and CENTRAL were searched for English language publications indexed from 1 January 2010 to October 2021 meeting protocol-defined eligibility criteria (search strategy in online supplemental table 1). Bibliographies of relevant SLRs were hand-searched for additional citations.
Supplemental material
Articles were included if they met predefined PICOS (Population, Intervention, Comparison, Outcomes and Study) criteria:
Population: Females undergoing PPIUD placement
Intervention/comparator: No limits
Outcomes:
IUD utilisation and/or safety within 12 months
Efficacy/effectiveness (UIPs within 18 months)
Study design: Interventional or observational studies
Abstracts and full-text publications were independently screened by two investigators (KK, EGE), with discrepancies adjudicated by a third investigator (BAM). Data were extracted by one researcher and validated by a second researcher. The American College of Obstetricians and Gynecologists (ACOG) endorses a best practice for immediate PPIUD as placement ‘in the delivery room, within 10 min of placental delivery in vaginal and caesarean births, when possible’,16 and the WHO advises insertion at <48 hours or >4 weeks. In an effort to capture all peri-delivery, in-hospital, IUD insertions we a priori defined PPIUD as that occurring up to 72 hours following delivery, while in hospital; studies describing IUD insertion as ‘immediate’ but without a specific timeframe reported were also included.
Results were qualitatively summarised within country income strata, based on 2021 World Bank classifications.17 Groups were defined on a gross national income per capita basis using the World Bank Atlas method in 2019 US$ (per person in 1 year (2019): low income: ≤$1035; lower-middle income: $1036–$4045; upper-middle income: $4046–$12 535; high income: >$12 536).17 Two income groups were defined: ‘lower income’ for low- and lower-middle-income countries and ‘higher income’ for upper-middle and high-income countries.
Risk of bias/quality assessment
Two investigators independently performed quality assessment of included studies using best-practices instruments18–23; discrepancies were adjudicated by a third investigator.
Patient and public involvement
No patient involvement.
Results
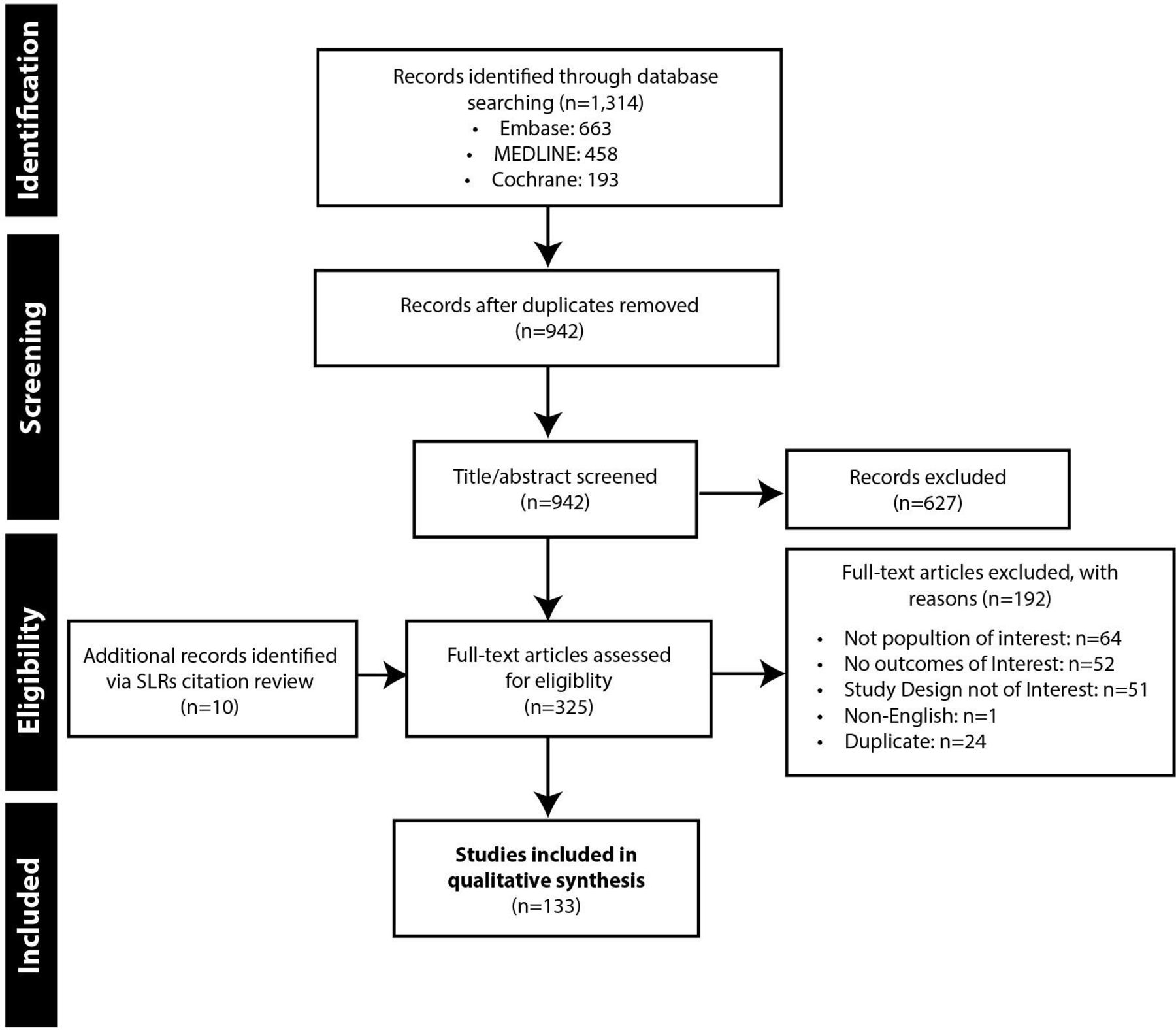
Nine hundred and forty-two unique records were identified via database searches and screened; 325 full-text publications were reviewed, including 10 records identified from the SLR bibliography searches; 133 publications were included (figure 1).

Study selection flow diagram. SLR, systematic literature review.
Study characteristics
Slightly more than half of included studies were observational (n=72; 54%) and 46% were interventional (n=61) (online supplemental table 2). Studies were conducted worldwide, with India (n=35) and the USA (n=23) having the largest representation; data were captured between 1995–2020. Most studies (n=87) were conducted at a single centre, while 44 studies included multiple centres (2–137 sites); two studies used data from claims databases. Twelve studies were from low-income countries, 75 from lower-middle-income countries, 15 in upper-middle-income countries, and 31 studies were from high-income countries (figure 2).

{kind=link}
{kind=link}
Geographic distribution of included studies by economic status. World Bank Country and Lending Groups Country Classification for the fiscal year 2021. Low-income economies are defined as those with a gross national income per capita of $1035 or less in 2019; lower middle-income economies are those with a gross national income per capita between $1036 and $4045; upper middle-income economies are those with a gross national income per capita between $4046 and $12 535; high-income economies are those with a gross national income per capita of $12 536 or more. *Some studies report on more than 1 country in different economic groups.
Quality assessment
RCTs followed best practices for random sequence generation, with low likelihood of attrition bias; however, in three studies,24–26 attrition information was not reported. Of the non-randomised interventional studies, 90% were good quality overall (online supplemental table 3a-e), with outcomes reliably measured and appropriate statistical analyses conducted. The main limitation in those studies was lack of a control group. In observational prospective studies, many women were lost to follow-up (only 20% of studies reported completed follow-up), with greater attrition as follow-up time increased, but despite this attrition, the studies were generally of good quality. In retrospective studies, participant eligibility and inclusion/exclusion criteria were adequately described, and valid statistical techniques were used with justification of the analyses conducted. Almost all (88%) of the cross-sectional studies were good or fair quality (30% considered good quality) with objective, standard criteria used for outcome measurement. No studies were excluded based on quality.
Population characteristics
Data from 4 200 343 women worldwide were included. Mean age ranged from 18.3 to 37.5 years. Studies in the lower-income group tended to have younger participants. Sample size across studies varied greatly, with the largest samples from lower-income countries.
The proportion of women with vaginal versus caesarean deliveries was similar across income strata.
In terms of timing of PPIUD placement across the included studies, in 125/133 (94%) IUD timing was explicitly ≤48 hours. In seven studies, while the timing was not reported in terms of hours or days, it was inferred by the timing description that insertion was within 48 hours (eg, ‘immediately after childbirth’, ‘immediate post-pregnancy IUD placement’). In one study the IUD insertion time was potentially beyond 48 hours,27 as the authors reported: ‘Inpatient postpartum refers to insertions of IUDs and implants occurring during the same hospitalisation as a delivery up to 7 days after delivery.’ Table 1 displays the definitions used in each of the 133 studies.
Sample characteristics of included studies in the global systematic literature review examining postpartum intrauterine device use and effectiveness and safety outcomes (n=133)
PPIUD utilisation
Higher-income countries
A study utilising US claims data suggested that in-hospital PPIUD insertion has increased over time (0.10/10 000 deliveries from 2001 to 2002,28 0.55/10 000 deliveries from 2007 to 2008,28 and 6/10 000 from 2013 to 2016).29 Evidence from two non-randomised interventional studies in Scotland between 2015–2019 suggested higher utilisation of PPIUD following caesarean (12.9%30) versus vaginal (4.7%31) delivery. In contrast, in a prospective observational study conducted between 2006–2008 in Guatemala, none of the women who had a caesarean delivery opted for a PPIUD compared with 0.16% of women with a vaginal delivery (table 2).32
Postpartum intrauterine device use utilisation and continued use at 3, 6, and 12 months post-insertion
Lower-income countries
Across 38 studies from lower-income countries, PPIUD utilisation ranged from 2.1%33 of all the deliveries in Nepal during 2015–2017 to 46% of 127 women in Kenya participating in an RCT in which intensive or usual family-planning counselling was given.34 An analysis of multiple countries in Africa found an increase in the proportion of women choosing PPIUDs over time, from 8.6% (748 of 8687 women receiving PPIUD counselling) in 2014 to 22.7% (1521 of 6707 women counselled) in 2015.35 Likewise, in a large real-world retrospective study in India, PPIUD use increased from 4.7% (1264 of 26 678 deliveries at a single hospital) in 2010 to 21.4% (5974 of 27 939 deliveries) in 2017.36 An analysis of PPIUD use across Sri Lanka, India, Nepal, Bangladesh, Tanzania, and Kenya revealed country-level differences in utilisation; considering all deliveries from 2014 to 2017 from participating hospitals, PPIUD use was similar in Nepal (2.1%; 2503/119 884 deliveries), Kenya (2.3%; 1651/72 340 deliveries), and Sri Lanka (2.7%; 8055/291 861 deliveries); slightly higher in Bangladesh (5.9%; 5255/87 951 deliveries); and much higher in India (23%; 16 643/72 195 deliveries) (table 2).33
Continuation of IUD use within 3, 6, and 12 months postpartum
Continuation of IUD use over the 12 months following immediate PPIUD insertion was reported in 67 studies and appeared similar across country-level income groups. The proportion of women with PPIUDs in place at early follow-up periods tended to be high, with a decrease by 12 months. In 41 of 52 (79%) studies, regardless of income group, >80% of women still had their IUD in place by 6 weeks to 3 months post-insertion; by 6 and 12 months, the proportion of studies reporting that >80% of women had their IUD in place was 76% (35 of 46 studies) and 54% (13 of 24 studies), respectively. However, only 24 studies reported utilisation beyond 6 months (table 2).
Higher-income countries
Across 16 studies from higher-income countries, 44–100% of women who had an immediate PPIUD inserted continued to have an IUD at 6 weeks to 3 months post-insertion (in 14 of 16 studies, >80% of women had an IUD in place between 6 weeks and 3 months). Across 24 studies, IUD utilisation at 6 months post-insertion ranged from 56–100%. Across the 11 studies from higher-income countries in which it was reported, IUD utilisation at 12 months ranged from 29–87%.
Lower-income countries
Across 36 studies from lower-income countries, 44–99% of women who had an immediate PPIUD continued to have an IUD at 6 weeks to 3 months following insertion (in 27 of 36 studies, >80% of women had an IUD in place for 6 weeks to 3 months). Across 22 studies, IUD utilisation at 6 months post-insertion ranged from 75–97%. Across the 13 studies from lower-income countries in which it was reported, IUD utilisation at 12 months ranged from 60–97%.
PPIUD effectiveness
Pregnancies following PPIUD insertion were reported in only 37 studies, and only two studies had follow-up data up to 18 months; the remaining studies reported pregnancies occurring by 12 (n=11), 6 (n=17), and 3 (n=7) months following PPIUD insertion. Across 15 studies from higher-income countries, including a total of 2516 women with a PPIUD, 60 pregnancies occurred and appeared to arise following IUD removal rather than device failure. Across 22 studies from lower-income countries in which pregnancies were reported, 36 pregnancies occurred among 9675 women who received PPIUDs. Similar to higher-income countries, pregnancies following PPIUD placement were more commonly associated with subsequent removal, not device failure (online supplemental table 4).
PPIUD expulsions
Across studies from both higher-income and lower-income countries, data on expulsions (either partial or complete) were most often reported at 6–8 weeks following PPIUD insertion. In our synthesis we categorised expulsions occurring by 3, 6, and 12 months. Across the 137 arms in which expulsions were reported, most (102/137 (74%)) were reported by ≤3 months; in 59 and 23 study arms, expulsions occurring by 6 months and 12 months, respectively, were reported. Only 11 studies reported all three time points, allowing for a direct comparison in expulsion timing. From those 11 studies, results suggested expulsions occur earlier rather than later after insertion. Specifically, the proportion of women with expulsions ranged from 0–23% by 3 months compared with 0–14.5% and 0–11.3% by 6 and 12 months, respectively. Corroborating those results, the data from all study arms (ie, including those in which all three time points were not reported in the same study) also suggested a greater proportion of expulsions by 3 months (0–46.2%) versus 6 (0–26.7%) and 12 months (0–11.3%) (online supplemental tables 5 and 6).
Safety
PPIUDs were associated with infrequent occurrence of abnormal bleeding, uterine infections, or perforations.
Abnormal bleeding
Definitions and severity of bleeding events following PPIUD insertion varied across studies and included spotting to haemorrhage. Bleeding complications following PPIUD insertion were infrequent across the 42 studies in which they were reported; most studies reported occurrences in <10% of women. Bleeding complications appeared more frequent in lower- versus higher-income countries.
Higher-income countries
Bleeding complications were reported in 11 studies (three RCT, two non-randomised interventional, four prospective cohort, and two retrospective cohort studies). Overall, the proportion of women experiencing bleeding at any time point ranged from 0–10%. In one RCT, a case of postpartum haemorrhage occurred in the operating room following IUD placement and hysterotomy closure.37 In that same RCT, five women (10%) underwent IUD removal due to side effects (primarily bleeding, pelvic pain, or both).37 In another RCT, a woman had a retained clot with bleeding immediately on placement of the PPIUD; no further bleeding occurred following IUD removal at approximately 5 min after initial placement.38 In a retrospective study, IUDs were removed in three of 169 women (2%) due to postpartum haemorrhage.39 No other peri-insertion bleeding events were reported. In an RCT from Australia, ‘frequent’ bleeding (not further defined) occurred at 6 weeks of follow-up in 12 of the 24 women with intra-caesarean insertion and available follow-up data, and in 26% and 9.5% of the women at 3- and 6-month follow-up, respectively. Other bleeding events at 3 months reported across three studies included spotting (1%), ‘bothersome bleeding’ (3%), and bleeding associated with an IUD rotated to transverse position (2%). At 6 months post-insertion, bleeding events were reported in five studies, including abnormal bleeding (0–3% of women), removal of IUD due to bleeding (1–4%), IUD rotation to transverse position with bleeding (4%), and the aforementioned ‘frequent bleeding’ (9.5%). At 12 months post-insertion, bleeding was reported in one study and occurred among 2% and 5% of women with caesarean and vaginal deliveries, respectively.
Lower-income countries
Thirty-one of 33 studies from lower-income countries reported bleeding complications in <20% of women; most bleeding events were not well defined. Exceptions arose from one study from India in which 89% of 680 women who had copper IUDs inserted reported ‘spotting’ (blood-stained vaginal discharge apart from menstruation).40 In that study, 10% of women requested IUD removal due to bleeding. Another study, involving 3753 women who received copper IUDs, reported that 28.1% had ‘irregular bleeding’.41
Infections
Evidence from 53 studies indicated infrequent development of infections following PPIUD insertion.
Higher-income countries
Across 14 studies reporting infections, the proportion of women with infections ranged from 0–3% in 12 of the 14 studies. In one of the remaining two studies, four (5%) women had infections (type not defined)42 and in the other, 10 women (11%) had cervicitis or pelvic inflammatory disease (PID): seven women received empiric treatment for cervicitis or PID, and three women reported having an infection that was diagnosed outside of the study centre.43
Lower-income countries
Infection following PPIUD use was reported in 39 studies from lower-income countries. In the eight studies reporting immediate PPIUD insertion infections data, two studies reported wound infections immediately after insertion of a copper IUD during caesarean deliveries (in 1.7%44 and 10% of women45) while the remaining six reported no infections. Within 3 months post-insertion, across 21 studies, the proportion of women with infections ranged from 0% (eight studies) to 7.5%.41 By 6 months follow-up, the proportion of PPIUD-related infections was very similar to earlier follow-up, from 0% in five studies to 5.4%.46 The latter was reported in a retrospective study that included all postpartum genital infections in 128 women in Ivory Coast.46 In the few studies (n=5) in which infection occurrence at 12 months was reported, the proportion of women with infections was ≤3.3%.26
Perforation
Across 41 studies reporting on this outcome, perforations following PPIUD insertion were rare. Seven perforations were reported: three from real-world studies after copper IUD insertion, and four in an RCT using copper IUDs. The reported cases include perforations with delayed diagnoses, but details on the perforations were largely missing.47 48
Higher-income countries
Across twelve studies from higher-income countries, two perforations were reported and both were diagnosed at 6 months post-PPIUD insertion. One of the affected women required laparoscopic removal49; in the other, the copper IUD was found, by ultrasound, to be partially perforated through the anterior lower segment of the uterus following insertion.47
Lower-income countries
Across 29 studies from lower-income countries, one of 736 patients from a retrospective study in India experienced a perforation diagnosed at the 6-week follow-up visit, with the device located in the abdominal cavity.48 In one RCT from Pakistan using copper IUDs, it was reported that three (2%) of 76 women who underwent vaginal delivery had perforation, and one of 75 (0.7%) women who underwent caesarean section had perforation50 51
Discussion
Results from this SLR of globally published data on PPIUD use suggest an increase in PPIUD utilisation over time in both higher- and lower-income countries, with a greater increase in lower-income countries. This trend may reflect more concerted focus on promoting PPIUDs in lower-income countries; promotion of PPIUDs was the aim of 21% of the lower-income country group studies versus only 6% of the higher-income country group studies. Still, PPIUD appears to be underutilised. LARCs are significantly more effective at preventing UIPs versus other contraceptive methods,8 are recommended for use by the WHO, and are categorised in the top tier of contraceptive effectiveness by the US Centers for Disease Control and Prevention.9 However, in 2019, only 6.5% of reproductive-age women in higher-income countries and 3.0% of women in lower-income countries used an IUD.7–9 In several studies, the proportion of women consenting to PPIUD insertion prenatally was higher than the proportion later receiving the intervention; better characterisation of reasons for opting against PPIUD use is needed.
Increasing IUD use may help mitigate the excessive economic burden of UIPs. In the USA, 2011 annual direct medical costs of UIPs were estimated at $4.6 billion; half of the costs were attributable to imperfect contraceptive adherence.6 Direct medical costs of UIPs to the National Health Service in the UK were estimated at >US$300 million in 2010.8 Use of PPIUDs may also improve subsequent clinical outcomes. Postpartum is a particularly crucial time for contraceptives, as short-interval pregnancies are associated with poor maternal and birth outcomes. The ACOG recommends avoiding interpregnancy periods shorter than 6 months and considering the benefits of waiting ≥18 months between pregnancies, while the WHO recommends a 24-month interval between a live birth and next pregnancy.14 52 53 Whether to use contraception and the type and timing of contraception is a woman’s personal choice and may be influenced by factors such as healthcare access, socioeconomic status, culture, and perceptions regarding various contraceptive options.
Our findings suggest that increasing time from PPIUD insertion is associated with a decrease in PPIUD prevalence, although long-term follow-up data were limited. Nonetheless, reported pregnancies across studies were very low. A limitation to the effectiveness information is the sparse availability of published data out to 18 months. Whether an IUD was not in place due to expulsion or voluntarily removal was inconsistently reported. In lower-income countries, the most common reason for IUD removal was inclination to other methods.54 The occurrence of IUD expulsions varied widely across studies; however, the timing of expulsions was consistently primarily in the early postpartum period. In one trial, the mean time to expulsion was 12.6 days.37 In another trial, all expulsions occurred by 3 months post-insertion.55 In a prospective cohort study, median time to expulsion was 4.1 weeks.56 Another observational prospective study found that 86% of expulsions occurred within 6 weeks.57 In one study, 88% of women with expulsions requested re-insertion.58
A limitation in some studies was conducting follow-up appointments via the phone, and, in some cases, ultrasounds were not routinely offered unless there were symptoms indicative of expulsion or misplacement. Consequently, continuation of IUD use over time may not be accurately reported, and expulsions may be under-recognised and under-recorded. A Cochrane review of RCTs did not find evidence supporting a significant difference in expulsion rates based on timing of insertion.13 Likewise, in a recent SLR and meta-analysis including observational and interventional studies, there was no significant difference in expulsions between IUDs placed from >10 min to <72 hours versus >4 weeks post-delivery, although IUD placement ≤10 min was associated with a significantly increased risk of expulsion versus >4 weeks.11 A recent estimate suggested immediate insertion would prevent an additional 88 UIPs per 1000 women over 2 years compared with routine placement.59 Thus, the benefit of earlier insertion likely outweighs a potential small increased expulsion risk. Additional evidence points to a variety of factors that may affect expulsion risk, including the device type, delivery mode, age, parity, and provider experience.11 12
The data compiled suggest that PPIUDs are associated with infrequent occurrences of abnormal bleeding, uterine infections, and perforations. A limitation to the safety data includes inconsistent definitions of safety events across studies. Additionally, follow-up was often conducted with the IUD user, sometimes over the phone; accordingly, reported outcomes would need validation by a healthcare professional. As with any literature review, relevant studies may have been missed; similarly, the exclusion of non-English language papers may have omitted relevant data. Our analysis of IUD perforation rates does not distinguish between complete perforations (which resulted in the IUD moving to the abdominal cavity and required surgical management for removal) and partial perforations (which may have been managed in an outpatient setting). It also includes reports where the event was detected at later timepoints. Uterine perforation may occur, most often during insertion, but may not be noticed until much later since it can be asymptomatic. It is therefore possible that the limited follow-up in the studies may have led to underestimation of the event rate, as a relevant portion of women present with little or no symptoms and may only be diagnosed after several years of use or when presenting for IUD removal60—emphasising the need for appropriate patient counselling and surveillance.
Conclusion
Evidence from this SLR suggests that IUDs inserted in the immediate postpartum period are safe and effective. Future research to better characterise reasons for opting against PPIUD use is needed to permit development of more effective interventions to increase appropriate utilisation of PPIUDs.
Additional resources
Faculty of Sexual and Reproductive Healthcare (FSRH) clinical guideline: contraception after pregnancy. (January 2017, amended October 2020) (https://www.fsrh.org/standards-and-guidance/documents/contraception-after-pregnancy-guideline-january-2017/).
American College of Obstetrics and Gynecology (ACOG) Committee Opinion No. 670: immediate postpartum long-acting reversible contraception. Obstet Gynecol 2016;128(2):e32–7.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EG-E, BM, and KK participated in developing the study methodology, study conduction, and reporting. KRB planned the study, provided epidemiologic review, and submitted the study. YW planned the study and provided medical expert review. NW provided medical expert review. JL planned the study and provided medical expert review. SJ provided compliance review. FP provided statistical review.
Funding This study was funded by Bayer HealthCare.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests EG-E reports personal fees from Xcenda LLC, during the conduct of the study. JL reports personal fees, non-financial support and other from Bayer US LLC, outside the submitted work. KRB, YW, NW, and FP are all employees of Bayer, which manufactures IUDs among its portfolio of products.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.