Article Text

Abstract
Introduction The objective of this study was to compare ever-in life contraception use, use of contraception at current conception, and planned use of contraception after an induced abortion, among three groups of women: migrants, second-generation migrants and non-migrant women, and to compare the types of contraception methods used and intended for future use among the three groups of women.
Methods The cross-sectional study administered a questionnaire face-to-face to women aged 18 years and older who were seeking abortion care at one of six abortion clinics in Stockholm County from January to April 2015.
Results The analysis included 637 women. Migrants and second-generation migrants were less likely to have used contraception historically, at the time of the current conception, and to plan to use contraception after their induced abortion compared with non-migrant women. Historically, non-migrants had used pills (89%) and withdrawal (24%) while migrants had used the copper intrauterine device (24%) to a higher extent compared to the other two groups of women. Both the migrants (65%) and second-generation migrants (61%) were more likely than the non-migrants (48%) to be planning to use long-acting reversible contraception.
Conclusions Lower proportions of contraception use were found in migrants and second-generation migrants than in non-migrants. In addition, there were significant differences in the types of contraception methods used historically and intended for future use.
- induced abortion
- contraception
- counselling
- ethnic minority migrants
Statistics from Altmetric.com
Key messages
The overall use of contraception historically, at conception, and planned use after an induced abortion was lower among migrants and second-generation migrants.
Historically, the use of pills and withdrawal was higher among non-migrants and the copper intrauterine device among migrants.
Planned use of long-acting reversible contraception was higher among migrants and second-generation migrants.
Introduction
In both western Europe and the USA, migrant women have a higher frequency of induced abortion than do the majority of the female population.1–4 Previous research from Sweden has also found that migrant women, including adolescents, are more likely to have an induced abortion than are Swedish-born women,5 and that migrants had less experience using contraceptives than Swedish-born women.6
In Sweden, 35 000‒38 000 induced abortions are performed annually, translating into an abortion rate of 20.8 per 1000 women of reproductive age, which is higher than in other western European countries.7 Women aged 20‒29 years have the highest rate of induced abortion in Sweden7 and Stockholm County is one of three counties that have the highest abortion rates.8 Swedish legislation states that all women regardless of citizenship should be able to have an induced abortion on request up to 18 weeks of gestation.
The reasons suggested for higher frequencies of induced abortion include language barriers, lack of knowledge regarding contraception, limited access to contraception or information about contraception, ambivalence regarding sexuality, factors related to relationships with partners, and uncertain living conditions.1 2 Multiple factors determine contraceptive uptake and use, and easy access, good counselling and the availability of effective, acceptable methods are prerequisites to preventing unintended pregnancies in general.6 9
In Sweden, contraception counselling is free of charge for all women. In the area of study, copper intrauterine devices (IUDs) are free of charge. Hormonal contraception methods such as the patch, vaginal ring, injection, intrauterine system (IUS), implant and most hormonal pills are partially subsidised for women under the age of 26 years and may even be free of charge for women aged under 21 years, depending on their region of residence. The unmet need for contraception has been estimated as being 9% among all Swedish women and 13% among Swedish women aged 21‒30 years.10 However, women who did not understand Swedish were not included in the study.10 Among women who used a method of contraception, 24% used long-acting reversible contraception (LARC), including copper IUDs, the levonorgestrel-releasing IUS or a subdermal contraceptive implant.10 LARC methods are highly effective and reduce the risk of contraceptive failure, unintended pregnancy, and both first and repeat induced abortions when compared with other methods, including pills, patches, vaginal rings and injections.11–13
The United Nations’ Sustainable Development Goals state that by 2030 all women should have rights and access to sexual and reproductive healthcare, including contraception.14 One goal of Sweden’s public health policy is to achieve equal healthcare for the entire population.15
Achieving these global and national goals requires increased knowledge of migrant women’s contraception use today, especially since migrant women have a higher risk of repeated abortions.6
Consequently, the current study sought to compare the methods of contraception used by migrant, second-generation migrant and non-migrant women. Specifically, the study identified the methods used historically and at conception and the methods intended for use after induced abortion among these three groups of women.
Methods
Study design and population
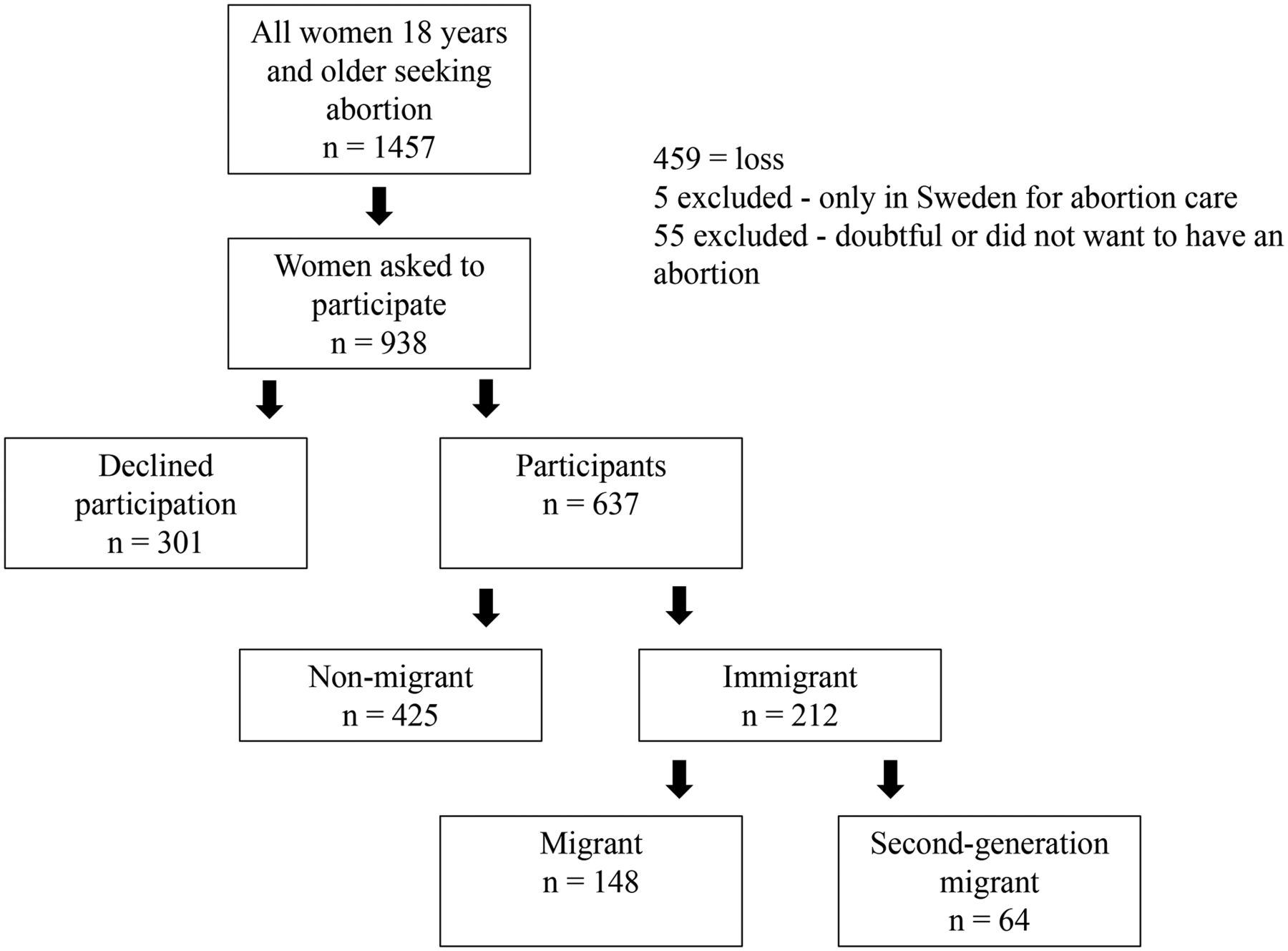
The study used a cross-sectional design, which was applied using a questionnaire administered during a face-to-face interview with the midwife at the abortion clinic. The study was conducted at six abortion clinics in Stockholm County, Sweden that collectively account for approximately 55% of all abortions in the county. The study used consecutive enrolment, and data collection took place from January to April 2015. The eligible women were at least 18 years old and had sought and decided to have an induced abortion. The outcome measures were: i) the historical use of contraception and the methods used, ii) the method used at conception, and iii) the methods intended for use after the abortion. The study included both migrant and second-generation migrants and non-migrants. Migrants was defined as born abroad while second-generation migrant status was defined as having been born in Sweden to two parents who were born abroad.16 Adopted women were defined as non-migrants if they were born abroad to one or two parents who were born in Sweden. Figure 1 outlines the sampling procedure.

{kind=link}
Flowchart of eligible, enrolled women and the final study population.
Data collection
Each interview took place after the woman’s first appointment at the abortion clinic. If the woman gave her consent, the healthcare provider conducted a face-to-face interview to allow the women to answer the questionnaire. The same healthcare provider also provided contraceptive counselling, and prescribed and inserted, if needed, contraceptives after the abortion. The questionnaire contained questions related to sociodemographic background and experiences with and planned use of contraception. The majority of the questions had been used in a previous Swedish study.9 Before the study commenced, the questionnaire was pilot tested on six women: three migrants, one second-generation migrant and two non-migrants. Two professional interpreters were used. The pilot test did not lead to any changes in the questionnaire. The written information used in the study was translated into the seven languages most commonly used by patients at the clinics, and a professional interpreter was used when needed. Ethical clearance for the study was obtained from the regional ethics committee in Stockholm (Dnr 2014/1191-31/5).
Data analysis
The data were analysed using SPSS Statistics version 23. The researchers assumed that 20% of the women seeking abortions would be migrant and that the differences in the historical use of contraceptives between migrants and non-migrants would be 10%. These assumptions are based on data from a previous study.6 To achieve a power of 80%, the researchers aimed to recruit 1300 women. However, the study was only able to include 637 participants (figure 1). Fisher’s exact test, for some calculations obtained through a Monte Carlo simulation, and Chi-square tests were used to compare the sociodemographic characteristics, contraception use and contraception methods of the migrants, second-generation migrants and non-migrants. A p value of less than 0.05 was considered statistically significant.
Patient and public involvement
Patients were not involved.
Results
Study population
During the study period, 1457 women sought abortion care at the clinics. Of these, 459 were not asked to participate in the study, five were excluded because they were in Sweden only for abortion care and 55 were excluded because they expressed doubt that they would have an abortion or had decided not to have one. Of the 938 women who were invited to participate, 637 agreed, of which 67% were non-migrants, 23% were migrants and 10% were second-generation migrants (figure 1).
Differences in sociodemographic characteristics were observed, and among migrants, the largest age group was 30‒34 years, while the non-migrants and second-generation migrants were younger (table 1). The migrants were more likely to have children than the women in the other two groups. In all three groups, the majority had a secondary school education and were employed at the time of the survey (table 1).
Sociodemographic characteristics of non-migrant, migrant and second-generation migrant women seeking abortion care in Stockholm County
Sexuality education and contraception counselling
The migrants were less likely to have received any sexuality education in schools (63%) than the non-migrants (98%) and the second-generation migrants (94%) (online supplementary tables). The migrants also were less likely to have received contraception counselling (87%) compared with the non-migrants (99%) and second-generation migrants (97%) (online supplementary tables). Of those who had received contraception counselling, the migrants were more likely (48%) to have received it from midwives at primary healthcare clinics in Sweden, and the majority of the non-migrants (73%) and second-generation migrants (60%) had received it at youth clinics. The migrants were more likely to state that they did not have sufficient knowledge to choose a method of contraception to use after their abortion (19%); only 10% of non-migrants and 13% of second-generation migrants gave these responses.
Supplemental material
Previous contraceptive use
In total, 96% of the respondents had used contraception at some point in their lives, but there were significant differences between the three groups, with non-migrants reporting the highest use (99%), second-generation migrants reporting the second-highest use (95%) and migrants reporting the lowest use (89%). In all groups, the most common contraception methods used were oral contraceptives, which were used by a significantly higher proportion of non-migrants (89%) than migrants (63%) and second-generation migrants (80%). The migrants were significantly more likely to have used copper IUDs (24%) than second-generation migrants (10%) and non-migrants (17%). In each group, about one-third stated that they had ever used LARC contraceptive methods (table 2A).
Contraceptive methods previously used by non-migrant, migrant and second-generation migrant women seeking abortion care in Stockholm County (multiple choices possible)
Contraceptive use at conception
At the time of conception, 32% had used a contraception method. Non-migrants used contraceptives at conception to a higher extent (34%) compared to migrants (25%) and second-generation migrants (30%), indicating the highest contraceptive failure among non-migrants (online supplementary tables). The most common methods in all three groups were condoms (38%) and pills (24%). There were no significance differences between the methods used at conception (table 2B). The most frequently stated reasons for contraceptive failure were lack of compliance (24%) and condom failure (22%). The migrants were more likely to report miscalculation of days (20%) as a reason for the failure than were non-migrants (10%) and second-generation migrants (11%) (online supplementary tables).
Contraceptive method used at time of current conception by non-migrant, migrant and second-generation migrant women seeking abortion care in Stockholm County
Intended future use of contraception
Of all the women, 93% planned to use contraception after their induced abortion. Among women aged 20‒24 years, the percentage rose to 98%, and for women aged 25‒29 years it fell to 92%. In particular, second-generation migrants aged 25‒29 years were less likely (78%) to be planning to use contraception after their abortion than women in either of the other two groups. The most common contraception method chosen by both the migrants and second-generation migrants was a hormonal IUS, and among non-migrants it was pills (table 3).
Type of contraceptive method planned for use post-abortion by non-migrant, migrant and second-generation migrant women seeking abortion care in Stockholm County
Important factors in choosing a contraceptive
For all women, the most important factor when choosing the method to use after abortion was that it did not have side effects (31%). Using a long-acting contraceptive was also more important to migrants (12%) than to non-migrants (8%) and second-generation migrants (9%) (online supplementary tables). Low-dose or hormone-free methods were mentioned as a factor by 19% of second-generation migrants, 18% of non-migrants and 11% of migrants. In addition, non-migrants (13%) were more likely to state that amenorrhea, or the cessation of regular bleeding, was an important factor than were migrants (7%) and second-generation migrants (4%). No participants stated cost as a factor in whether they planned to use a specific contraception method after their abortion (online supplementary tables).
For all groups, the proportion who had previously used LARC (32%) was significantly lower than the proportion who planned to use it after their abortion (53%). In particular, the proportions of both migrants (65%) and second-generation migrants (61%) who planned to use LARC were significantly higher than the proportion of non-migrants (48%) who intended to use it. Non-migrants aged 20‒24 years were the least likely (42%) to report planning to use LARC after their abortion.
Partner involvement in contraception decisions
In all three groups, slightly less than one-third of the women reported that their partner was involved in the decision about using contraception after the abortion. The non-migrants were more likely to state that their partner wanted them to use contraception after the abortion (86%) than were the migrants (73%) and second-generation migrants (82%). Furthermore, the migrants were more likely to state that they did not know if their partner wanted them to use contraception (22%) than were non-migrants (10%) and second-generation migrants (10%).
Discussion
Main findings
Among women seeking abortion care, both migrants and second-generation migrants were less likely ever to have used contraception previously than were non-migrants. These three groups of women also differed as regards the types of contraception methods they had used previously. Interestingly, the results indicated that migrants and second-generation migrants were more likely than non-migrants to be planning to use a LARC method after their abortions.
Findings in context
At the time of the current conception the migrants and second-generation migrants were less likely to have been using any method of contraception, while the non-migrants were more likely to have experienced failure of the contraception method they were using. Earlier research have pointed out the importance of improved counselling and access to LARC methods for nulliparous and young women, given the current low uptake of LARC among these groups.17 Structured contraception counselling can support women during their decision-making process and can increase the acceptance, selection and use of a contraception method, as well as adherence to it.18 19 The Contraceptive Health Research of Informed Choice Experience (CHOICE) method of contraception counselling has been shown to be effective for both short- and long-acting reversible forms of combined hormonal contraceptives and has been shown to both influence the method chosen and improve adherence to it.11 20–22 Studies that have evaluated the CHOICE method have found increased uptake of LARC and higher patient satisfaction with LARC methods compared with short-acting methods.23 24 LARC use among Swedish women aged 16–49 years is reported to be 24%.10 In the present study, non-migrants aged 20–24 years were less likely to report planning to use LARC after their abortion. Despite this, in this study the planned use of LARC increased by more than 20% in all age groups under 30 years compared with the historical use of LARC. Choosing a LARC method is in line with Sweden’s recommendations for contraceptive use.25
The findings of the present study indicate that pre- and post-abortion contraception counselling must be person-centred in order to acknowledge the womens’ needs. We found that migrants were more likely to state that they did not have sufficient knowledge to choose a contraception method after their abortion and that only 63% of the migrants had received sexuality education in schools. These findings are in agreement with the experience of abortion-care providers who have recounted their challenges in finding adequate time in which to provide sufficient counselling.26 From a public health perspective, it is important to increase both women’s and men’s access to person-centred information and shared decision-making.27 In Sweden, contraception counselling usually takes place in a one-on-one meeting, which may be a challenge for migrants from societies that are more collectivist.28 One potential approach to both increasing contraception use and decreasing unintended pregnancies may be to include both women and men in contraception counselling.29 Healthcare providers who counsel migrants have reported that cost and the presence or absence of regular bleeding are two important factors in their choice of contraception methods.30 However, the present study did not observe this among migrant and second-generation migrant women. Sweden’s national public health goal is to make the social conditions necessary for good health available to the entire population on equal terms. To do this, it is very important to be aware of health differences in the population, such as, for example, people with foreign backgrounds.31
Strength and limitations
A strength of the present study is its intention to include all women who were seeking abortion care, including those from various ethnic backgrounds. Previous studies have excluded migrants due to language barriers. The proportion of women never asked to participate in the study could be explained by a high workload at the clinics according to the healthcare providers. However, some midwives mention that due to language barriers, which made the encounters longer, migrants who did not speak Swedish might have been asked to participate to a lower extent. Consequently, there might have been more women from the migrant groups that were lost. It might be that those who were lost or who refused to participate used contraceptives at a lower rate than those who did participate, and that therefore although this might not have changed the results significantly, the ‘true’ use of contraceptives might actually be lower than that indicated by the present study. Some of the measured variables that were not significant might have been if the study had reached the intended sample size. We have compared contraceptive use among abortion-seeking women, and contrasted the use between the three groups. Consequently, we cannot say whether or not the observed differences are also valid had we compared contraceptive use among the three groups among women who had not sought abortion care. The participating clinics are the largest abortion clinics in Stockholm County and are geographically distributed in the whole county. All women in Stockholm County, regardless of their residence, could visit any of the clinics, therefore we do not believe the sample would be different even if there were more participating clinics. However, this was not a population-based study and selection bias cannot be ascertained. Due to the small number of women in the different groups within the study, we could not make stratifications of sociodemographic characteristics. This would have been interesting in a larger sample to strengthen the study’s validity.
Conclusions
In order to provide equitable, person-centred care, pre-abortion contraception counselling must recognise that knowledge and motives differ among women. Both migrants and second-generation migrants seem to have less knowledge of contraception and to be less likely to use a contraception method, and this should be taken into consideration when counselling these women. In addition, LARC uptake among non-migrants can be improved. The clinics offering comprehensive abortion care have an important role in contraception counselling for all women.
Acknowledgments
The authors would like to thank all who contributed to this study, especially the women, the providers and the abortion clinics. They would also like to thank Gaetano Marrone for his assistance with statistical analysis and Sebastian Emtell for entering the data.
References
Footnotes
KEI and ECL contributed equally.
Contributors KEI designed and implemented the study at the clinics, collected the data, cleaned and analysed the data and wrote the manuscript. ECL designed and implemented the study at the clinics, collected the data, cleaned and analysed the data and wrote the manuscript. KG-D secured the funding and revised the draft paper. BE secured the funding, designed the study and revised the draft paper. MK-A secured the funding, designed the study and revised the draft paper.
Funding This work was supported by FORTE Dnr 2013-2025 and FORTE Dnr 2016-01063.
Competing interests Dr. Emtell Iwarsson reports non-financial support from Bayer AB, non-financial support from RemovAid AS, outside the submitted work; Dr. Larsson has nothing to disclose. Dr. Gemzell-Danielsson reports personal fees from Bayer Ag, MSD/Merck, Exeltis, Gedeon Richter, Actavis, Ferring, HRA-Pharma, Exelgyn, SunPharma, Natural Cycles, outside the submitted work; Dr. Essén has nothing to disclose. Dr. Klingberg-Allvin has nothing to disclose.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper was first published online, a duplicate reference 25 has been deleted and a line from the supplementary file title has been removed.