Article Text

Abstract
Introduction Insertion of intrauterine methods of contraception (IUC) carries an inherent but small risk of perforation of the uterus, usually quoted at 2 in 1000. If perforation occurs, it is usually discovered either when a patient presents with ‘missing threads’ or with an unplanned pregnancy. Rarely, if the IUC has perforated bowel, patients can present acutely unwell although this sometimes occurs years after insertion. Asymptomatic perforation of the bowel (with IUC insertion or otherwise) is not common.
Case history In January 2018, a 41-year-old woman attended our community sexual and reproductive health service requesting removal of her intrauterine system (IUS). The clinic nurse performed this and during the consultation the patient revealed that several days earlier she had passed a previous ‘lost’ intrauterine device (IUD) when she opened her bowels. She came to believe this was an IUD inserted in 2006 that had been ‘lost’ and resulted in a pregnancy with her third child. We counselled her about her options and she had the IUS removed as she was worried this could happen again and opted to use condoms.
Conclusion This case reports an unusual presentation of a delayed and importantly ‘silent’ perforation of the uterus and bowel on insertion of IUC. The case highlights the importance of cross-specialty communication when an IUD has perforated or expelled resulting in a continuing pregnancy, so that appropriate imaging can be arranged following delivery of the baby.
- education and training
- family planning service provision
- intrauterine devices
- intrauterine systems
- long-acting reversible contraception
- case report
Statistics from Altmetric.com
- education and training
- family planning service provision
- intrauterine devices
- intrauterine systems
- long-acting reversible contraception
- case report
Case history
In January 2018, a 41-year-old woman attended our community sexual and reproductive health service requesting removal of her intrauterine system (IUS). During the consultation the patient revealed that some days earlier she had passed a previously ‘lost’ copper intrauterine device (IUD) in a bowel movement.
In September 2006, 3 months after delivery of her second child, the patient had attended a satellite clinic of our service for insertion of a Nova T380 IUD. Insertion was uneventful and the patient did not recall any significant pain in the following months. She had a longstanding irregular bowel habit and lower back pain, both predating her first pregnancy. Four months after the IUD insertion she missed a period and a pregnancy test was positive. She was referred to an early pregnancy unit to exclude ectopic pregnancy as it was assumed that the IUD was still in situ. Ultrasound scans confirmed intrauterine pregnancy but failed to demonstrate the IUD, and it was presumed that it had been expelled. No further abdominal or pelvic imaging was arranged. She opted to continue the pregnancy and had a vaginal delivery in September 2007. Her partner had a vasectomy and they relied on this for contraception until the relationship ended.
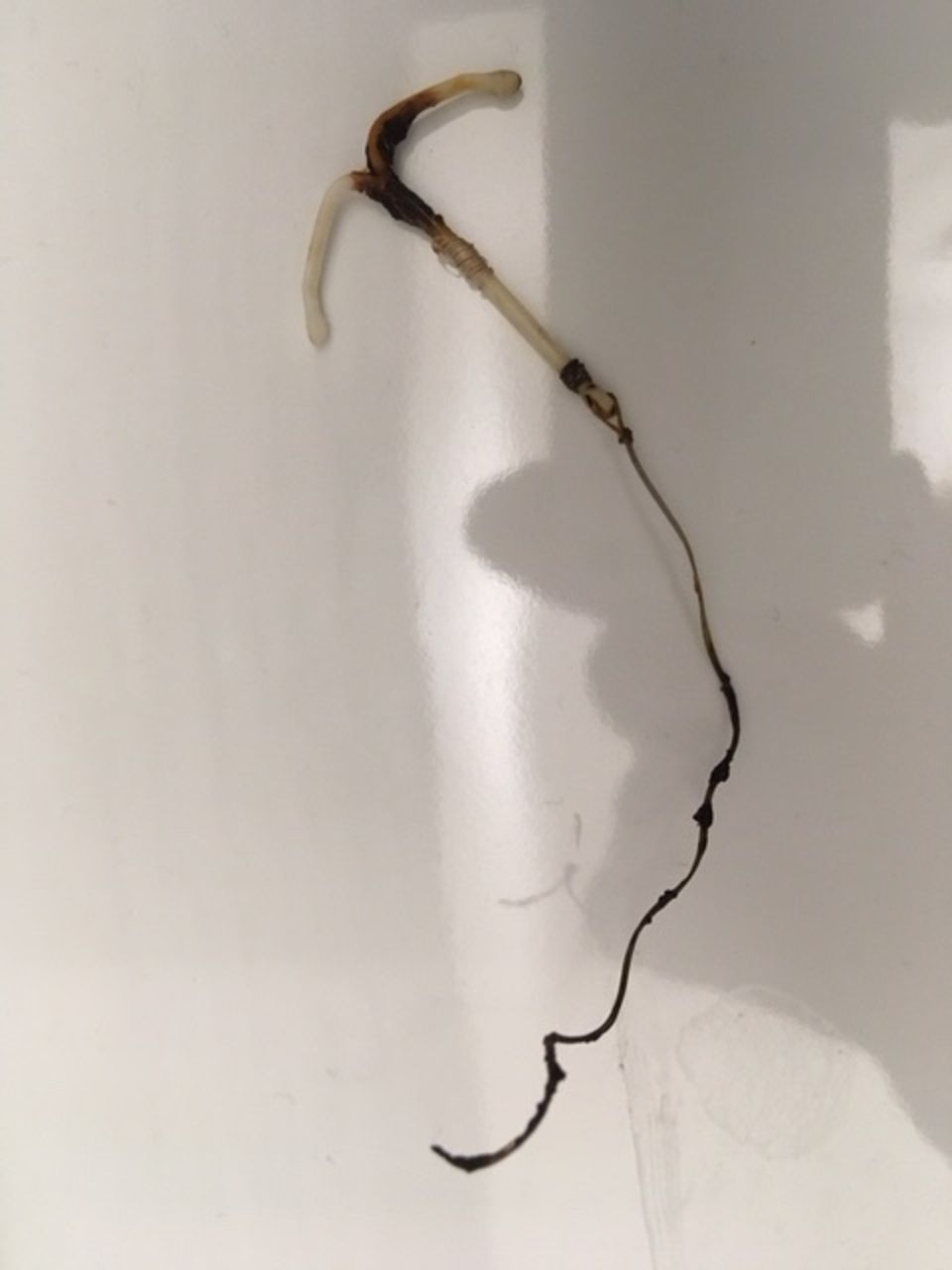
On meeting a new partner in September 2011, she had an IUS inserted for contraception until August 2013, when it was removed in order to conceive her fourth child. Following delivery of this baby she had a further IUS inserted and used this until she presented in clinic in January 2018, requesting its removal. She stated that after being constipated for 48 hours, she had passed a painful stool and on looking into the toilet bowl she saw what she described as ‘a piece of plastic sticking out’. She retrieved the stool and on closer inspection saw an IUD within it (figure 1). A self-performed thread check confirmed that her current IUS was in situ. She concluded that the IUD was the one that had been inserted in 2006 that had been ‘lost’, and she attended our service for removal of her IUS due to concern that this could happen again.
{kind=link}
Intrauterine device immediately post-expulsion in stool, photographed by patient.
After discussion the patient had the IUS removed and opted to use condoms. Following this history a pelvic ultrasound scan was performed, which was normal. On the advice of consultant colleagues in radiology and colorectal surgery, a magnetic resonance imaging (MRI) scan of her pelvis was performed to exclude any fistulae or diverticulosis. This was also normal.
Discussion
This case demonstrates an unusual presentation of a delayed and, importantly, ‘silent’ perforation of the uterus and bowel following insertion of intrauterine contraception (IUC). Perforation of the bowel with an IUD is rare, but when it does occur patients usually present with faecal peritonitis. There can be a prolonged period of time between IUD insertion and bowel perforation occurring.1 2 One possibility is that the IUD perforated the uterus but not the bowel upon insertion, and remained in the peritoneal cavity, resting on the bowel and slowly eroding through to the lumen, with the bowel re-epithelialising behind it.
The outcome of this case emphasises the importance of cross-specialty communication when an IUD is not identified during early pregnancy, so that a plain-film abdominal X-ray can be arranged following conclusion of the pregnancy. In the case of this patient, following the delivery of her third child, an X-ray would have located the IUD within the abdominal cavity and appropriate management could have been arranged.
Perforation into the pouch of Douglas, bowel and urinary tract are all recognised complications of insertion of IUC.3 Insertion in the postpartum period carries an increased risk of perforation from 4 to 36 weeks after delivery.4 However, evidence suggests that this risk is mitigated when insertion takes place in the immediate postpartum period (less than 48 hours after delivery) using an altered technique.5 Immediate postpartum insertion in this patient could potentially have avoided this outcome.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.