Article Text

Abstract
Objectives (1) To identify pregnancies associated with the use of the contraceptive implants Implanon and Nexplanon in the UK during two 5-year reporting periods. (2) To classify the possible reasons for device failure in cases reported for each implant. (3) To examine any differences between reasons for pregnancies associated with these products.
Study design Extraction of data from the UK spontaneous reporting system for adverse drug reactions in relation to etonogestrel implants. Reports indicating pregnancy were identified for the periods 2005–2009 (Implanon) and 2012–2016 (Nexplanon). Possible reasons for failure of the method in each reported case were assigned to one of eight predetermined categories.
Results After exclusions, 229 Implanon and 234 Nexplanon cases contained sufficient information for analysis. True method failures accounted for a majority of the pregnancies in those using contraceptive implants (58%); the next most common cause was missing implants (26% of pregnancies). In all categories of cases, there was no difference in frequency of pregnancy when the two time periods were compared.
Conclusions There is still potential for greater avoidance of pregnancies associated with etonogestrel implant use.
Implications This study underscores the continuing need for taking a full drug history, timing the insertion on days 1–5 or according to recommended quick starting routines and palpating the arm after implant insertion.
- contraceptive implant
- pregnancy
- non-insertion
- drug interaction
Statistics from Altmetric.com
Key messages
Although etonogestrel implants are a highly effective form of long-acting reversible contraception, unintended pregnancies continue to be reported in postmarketing use.
The main reasons for contraceptive failure of etonogestrel devices in ‘real-life’ use include true method failure, missing implants (most likely due to non-insertions) and drug interactions.
The proportion of failures for each device was not significantly different for Nexplanon when compared with Implanon.
Introduction
Etonogestrel implants (Implanon and Nexplanon or Implanon NXT) are highly effective methods of contraception with a licensed lifespan of 3 years. Combined data from 13 clinical trials of Implanon showed no pregnancies during 4103 woman-years of exposure; the Pearl Index observed was 0.00 (95% confidence limits: 0.00 to 0.09).1 Despite being a highly effective form of long-acting reversible contraception with a failure rate of less than 1 pregnancy per 1000 implants inserted over 3 years,2 pregnancies are regularly reported in postmarketing use.
Concerns about the failure to locate etonogestrel implants after insertion have highlighted the risks of deep insertion, migration in the arm and intravascular embolism.3 4 Impalpable implants may confer a risk of pregnancy if the implant has not been inserted5–7 or has been extruded/expelled.8–12 Previous pharmacovigilance reviews, mainly of Implanon, revealed that some pregnancies were associated with missing implants due to non-insertion: that is, failure to insert the implant and failure to recognise that this has happened.13–15 Non-insertion has been estimated in a prospective study of Nexplanon, with follow-up to 42 months, to occur in 0.1 per 1000 insertions.16
The single-rod etonogestrel implant Implanon was available in the UK between 1999 and 2010. In 2005, publications from spontaneous reporting in Australia and France were the first to identify the issue of missing implants.13 14 The development of a modified radiopaque implant and applicator (proprietary name Nexplanon) licensed in the UK in 2010,17 made imaging and evaluation of these ‘lost implants’ more straightforward. Pregnancies in etonogestrel implant users are rare but continue to be reported to the UK’s Yellow Card Scheme (https://yellowcard.mhra.gov.uk/). There is little information reported so far on failures of Nexplanon.
In this study, a comparison of spontaneous reports of unintended pregnancies associated with Implanon and Nexplanon devices during two 5-year periods was undertaken to investigate whether problems with insertion, in particular, non-insertions, have been resolved by the introduction of Nexplanon and its modified applicator. During this time, it is estimated that more than 150 000 implants were prescribed in the UK each year.18
Methods
Individual case reports of suspected adverse reactions are sent to regulators spontaneously by healthcare professionals and patients through the UK’s Yellow Card Scheme.19 Clinical information provided in these reports is analysed by the UK Medicines and Healthcare products Regulatory Agency (MHRA) and used to detect possible links between a medicine and an adverse effect.20 Data derived from Yellow Cards and pharmaceutical companies are publicly available for each medicine in the form of interactive Drug Analysis Profiles (https://yellowcard.mhra.gov.uk/idap). The inclusion of a reported reaction in a Drug Analysis Print does not necessarily mean it has been caused by the medicine, only that the reporter had a suspicion it may have been.
Cases of pregnancy in association with the use of Implanon and Nexplanon reported to the MHRA were identified for the periods 2005–2009 (Implanon) and 2012–2016 (Nexplanon). Since Nexplanon was launched towards the end of 2010 in the UK, the first quinquennium of reporting comprises solely Implanon devices and the second quinquennium comprises almost entirely Nexplanon devices.
Patient and public involvement
As the study was conducted based on secondary data, contraceptive users and the public were not involved in the design of the study.
Inclusion and exclusion criteria
All UK spontaneous reports in the MHRA database were screened to identify reporting of pregnancy, from any source – for example, healthcare professionals, patients or the pharmaceutical industry - occurring with etonogestrel devices. Pregnancy may have been diagnosed clinically at any time, or by the reporter stating that a miscarriage, ectopic pregnancy, termination of pregnancy or delivery had occurred.
The following reports were excluded:
All reports from other countries.
UK reports where the type of device was not specified.
Duplicate entries.
Assessment of reports
All cases were reviewed in accordance with a predefined standard operating procedure developed prior to the start of assessment. Two assessors (EC and MH-W) were involved in retrospectively reviewing spontaneous reports of pregnancy associated with either device during the two reporting periods. All cases were reviewed independently by at least one assessor and a subsample were assessed by two assessors to ensure consistency of assessment and decision-making. A third assessor (SR) was used for consultation on more complex cases. Reports were assessed to determine whether there was sufficient information to meet the following criteria:
Sufficient evidence of pregnancy (cases where patients reported symptoms, but a pregnancy test was negative or never confirmed were excluded).
The estimated conception date was after the date of implant insertion (cases where conception occurred prior to implant insertion were excluded).
The following additional aspects of each report were considered to determine the possible reason for failure of the implant:
Concomitant medication: all reported medications (prescribed and non-prescribed) were reviewed, along with the dates of administration.
Absence of the implant: evidence that the implant was missing included information about being unable to palpate the implant, imaging results and/or blood etonogestrel levels being negative. In the absence of such information, the implant was assumed to be present.
For the remaining cases, reasons for failure of the method were placed into predetermined categories (see table 1) and statistical comparisons (using χ2 and Fisher’s exact tests) were made between the Implanon and Nexplanon groups.
Summary of the reasons for implant failure during postmarketing use of Implanon (2005–2009) and Nexplanon (2012–2016)
Results
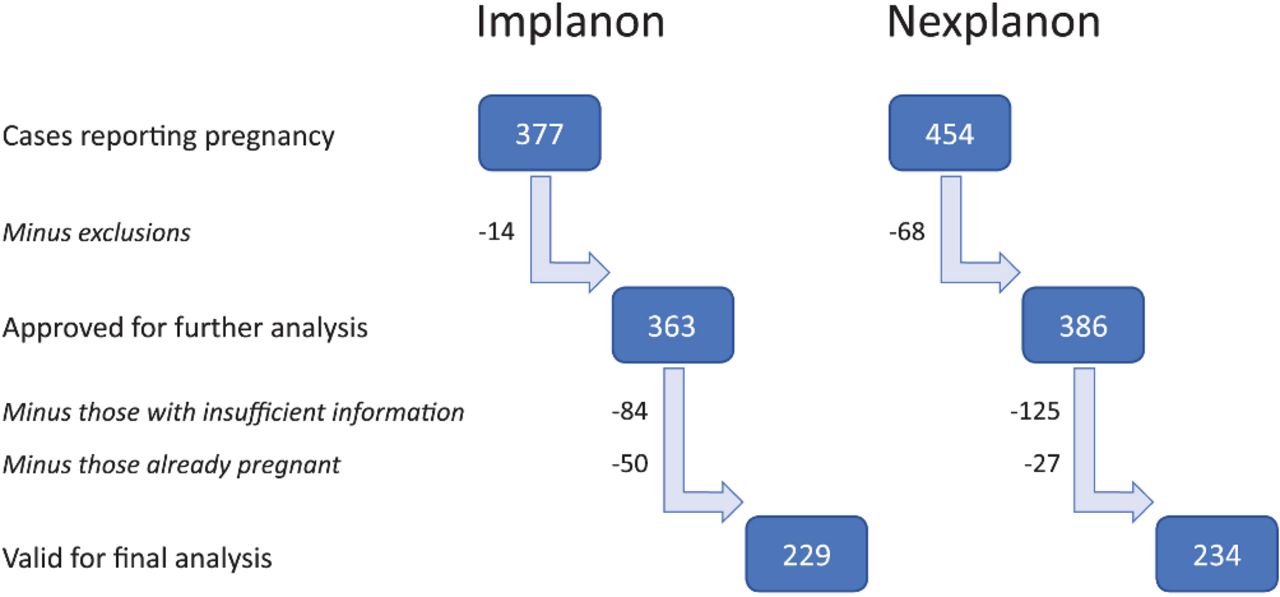
A total of 831 cases reporting pregnancy (377 for Implanon and 454 for Nexplanon) were retrieved from the database and reviewed. Of these, 463 (229 for Implanon and 234 for Nexplanon) were suitable for analysis (see figure 1).

{kind=link}
Cases suitable for analysis.
A summary of the reasons for implant failure for both devices is presented in table 1. True method failures accounted for the majority of pregnancies, with the next most common cause being missing implants. The frequency of each category of pregnancy cause was not significantly different when Implanon and Nexplanon were compared (table 1).
Missing implants
Of 68 missing Implanon cases, only 11 contained information about palpation of the implant after insertion and in 3 of these, the implant was never palpable. In addition, eight cases reported infection at the site of insertion; in five of these cases, the implant was palpable after insertion.
Of the 52 missing Nexplanon implant cases, 13 contained information about palpation of the implant after insertion. In five of these cases, the implant could not be palpated; in seven of the eight cases, in which the implant was palpable, an infection at the site of insertion was also reported.
Drug interactions
Of the 22 cases reported as possible drug interaction with Implanon, the drugs involved were carbamazepine, topiramate, rifampicin, St John’s wort and HIV medicines. Of the nine cases of drug interaction associated with Nexplanon, the most commonly reported suspect drugs were HIV medicines, carbamazepine, rifampicin and St John’s wort. The reports did not provide detailed information on the constituent drugs in HIV medicines.
Other categories of device failure
Other device failures were applicable to Nexplanon only (n=7, 3% of Nexplanon reports). Two reports indicated that the implant had been expelled and four cases reported a damaged or broken implant. In one case, a placebo device had been inserted in error.
Discussion
The source data for this study comprising 10 years’ experience of UK spontaneous reporting for etonogestrel implants and analysis of 463 reports of device failure make it the largest study of its kind to date. Continuing reports of unintended pregnancy show how ‘real-life’ use of etonogestrel implants is not associated with the zero-failure rate seen in the clinical trials and how contraceptive failures still occur, despite familiarity of clinicians with the method and design changes to the implant/applicator in 2010. Reasons for device failure included failure to exclude pregnancy prior to insertion, failure to quick start correctly,21 non-insertion and recognised drug interactions, which are all avoidable causes of pregnancy during implant use.
It has been postulated that human factors may be at work in cases of non-insertion.22 These types of medical errors could include a ‘learning curve’ effect, implying that as soon as clinicians become familiar with the method, errors will tend to diminish. Risk management programmes have been set up23 and ‘top tips’ offered to address this24 25 but our study suggests problems with implant insertion have persisted with the redesigned Nexplanon device.
Missing implants
In the 10-year reporting period of this study, there were only two reports of device expulsion and, even then, there was some doubt about these two cases being true extrusions because of lack of information in the reports. This is consistent with the understanding that extrusions/expulsions of etonogestrel implants are rare causes of pregnancy and that spontaneous expulsion of a device after correct insertion is close to impossible.26 Studies showing expulsion rates above zero have all been on levonorgestrel multiple-rod implants.27 Factors that have been proposed as predisposing to expulsion with levonorgestrel implants are incomplete insertion, wound infection, instances where the insertion procedure is a reinsertion in the same site, physical activity or low body mass index (BMI).
Non-insertion appears to be a more common phenomenon than extrusion. In our study, 30% of Implanon and 22% of Nexplanon cases were due to missing implants—that is, the implant could not be located at the time pregnancy was confirmed. Missing implants were a significant issue with Implanon6; the redesign to Nexplanon was intended to address this and facilitate their location.17 The proportion of cases associated with Nexplanon was not significantly different than with Implanon, suggesting the problem remains essentially unaltered.
Drug interactions
There is accumulating evidence from published reports of pregnancies occurring after concomitant use of potent enzyme inducers (see table 2). In this study, known drug–drug interactions were identified in 10% of Implanon and 4% of Nexplanon cases. While the proportion of these pregnancies was numerically lower for Nexplanon, the difference between the groups was not significant (see table 1). Ongoing reports with both devices suggest that the awareness of drug interactions among prescribers needs to be repeatedly reinforced.
Published reports of drug interactions resulting in pregnancy with the etonogestrel implant
Obesity
Although information regarding BMI was missing from most reports, in 27 cases (11 Implanon and 16 Nexplanon), the only reason identified for contraceptive failure was obesity. The current product information states that28:
Plasma levels of etonogestrel are inversely related to body weight and decrease over time.
Although clinical experience is limited, the contraceptive effect in heavier women during the third year of use may be lower than for women of normal weight.
Earlier replacement of the implant in heavier women may need to be considered.
Professional guidance points out that no increased risk of pregnancy has been demonstrated in women weighing up to 149 kg.29 This guidance also states that plasma levels high enough to block ovulation are not the only parameter that should be taken into consideration, as the method has other contraceptive mechanisms of action.29 In clinical trials, in which there was a zero failure rate, 175 of 1716 women (10%) weighed 70 kg or more, of whom 102 continued use beyond 2 years.1 Also, in the CHOICE study, failure rates did not vary by BMI.30
Almost half of these pregnancies (13 of 27 Nexplanon reports) were reported within 2 years of insertion, but there was not enough data in the reports for a more thorough assessment. In nine of the obesity cases, the women were morbidly obese (BMI>45 kg/m2 or weight>110 kg). Thus, although no other factor could be identified for these pregnancies other than obesity, some could also be classified as true method failures. Therefore, because of the uncertainties mentioned, cases referring to obesity in this study were classified as true method failures in table 1.
Broken implants
In four Nexplanon cases, it was reported that the implant was damaged, and this was classified as the reason for device failure (see ‘Other’ category in table 1). There are very limited other published data on this issue, although a pharmaceutical company response to an earlier case report suggested that breakage of an implant should not result in implant failure.31 Analysis of more cases of broken implants would be required to assess this further.
Self-removal
Missing implants have previously been attributed to self-removal32 (although the number of cases is very small). There have also been isolated reports of unsuccessful33 and successful34 35 self-removal of implants by the woman herself after the implant had been in place for some time, not immediately after insertion before the wound is fully healed. In this study, there were no reported cases of implant self-removal but this may be a phenomenon that is not spontaneously reported on Yellow Cards, as it is not a product problem or clinician error.
Conclusions
Main findings
The results of this study show that the most common reason for reported failure of etonogestrel implants is true method failure, a diagnosis of exclusion after assessment of other possible reasons for unintended pregnancies. Other reasons identified for device failure in this series included missing devices. A key finding was that the proportion of devices reported missing at the time of failure was similar for Implanon and Nexplanon. Our assessments suggested that non-insertion of the implant was a reason for the missing products, which is consistent with previous studies.13 One intended benefit of Nexplanon was a reduction of the risk of non-insertion22 (with the introduction of a ‘next-generation applicator’) but it appears that this aim has not been achieved.
More work, including continuing education of clinicians doing insertions, is needed on the prevention of avoidable causes of unintended pregnancies (eg, failure of insertion and drug interactions) associated with etonogestrel implants.
Strengths and limitations
The strengths of this study are
The largest and most recent study to report postmarketing experience of etonogestrel contraceptive devices.
Detailed clinical assessment of several hundred reports provides important information about reasons for failure of etonogestrel devices in real-world use.
Independent study using nationwide data.
The limitations of the study are
It is based entirely on spontaneous reporting data and could not assess overall rates of failure (ie, per 100 woman-years of use) in real-life use, as utilisation data were not available for the full period of review.
The amount of information for assessment was insufficient on many reports, with proportionally more instances for Nexplanon, and these cases had to be excluded from the analyses.
Implications for clinical practice
History-taking must always include a detailed drug history, including non-prescription medicines. Timing of insertion must be confined to days 1–5 of the cycle, or other times as recommended in professional guidelines, or the woman must have been using effective contraception during the whole of the insertion cycle.
Palpation of the implant in the arm by clinicians has become a routine in clinical practice. Nevertheless, women themselves should be strongly encouraged to palpate their arm after any dressing is taken off and report any difficulty in identifying the presence of the implant. Women using contraceptive implants need to be told that they should at all times be able to feel the implant in their arm and that they should question the suitability of concomitant prescribed medicines.
Implications for policymakers and manufacturers
There is a potential for greater avoidance of pregnancies associated with etonogestrel implant use. Policymakers need to ensure that health budgets are adequate to fund clinician updating. Manufacturers should strive further in the design of applicators to minimise human factors interfering with the successful delivery of implants into the arm.
Acknowledgments
We thank Dr Jane Woolley, MHRA, for her helpful comments on the manuscript. We also thank Professor Peter Thomas, Bournemouth University, for statistical advice.
References
Footnotes
Presented at This study was first presented as a poster at the 18th Annual Meeting of the International Society of Pharmacovigilance, Geneva, Switzerland, November 2018.
Contributors SR conceived the idea for this study. All three authors contributed to the study design. EC extracted the data. All three authors were involved in the data analysis. SR wrote the first draft of the manuscript and all the three authors contributed to subsequent drafts. All three authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the UK Medicines and Healthcare products Regulatory Agency.
Competing interests SR has received fees for acting as a trainer and for giving lectures on behalf of companies that market contraceptive implants.
Patient consent for publication Not required.
Ethics approval Not necessary. All data accessed were anonymised.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.