Article Text

Abstract
Background Youth involved in the juvenile justice system have high reproductive health needs and, on exiting detention, face the challenging transition of reentry. We conducted a systematic literature review to describe what is known about youths’ reproductive health needs during community reentry after incarceration.
Methods We searched PubMed, CINAHL, Cochrane Library, and Google Scholar for articles containing key words with the concepts ‘child or adolescent’, ‘incarcerated’ and 'reentry'. In the search, we defined the concept of ‘reentry’ as within 1 month prior to release (to include interventions involving pre-release planning) and up to 18 months after release from incarceration.
Results Our search yielded 2187 articles. After applying all exclusion criteria, 14 articles on reproductive health remained for extraction. The articles provided data on the following aspects of youths’ reproductive health: frequency of condom use (eight articles), sexual risk behaviours other than lack of condom use (seven articles), and prevalence of sexually transmitted infections (three articles).
Conclusions The literature on the reproductive health needs of youth undergoing reentry is extremely limited. Current intervention studies yield mixed but promising results and more intervention studies that address both pre-release reentry planning and the post-incarceration period are needed. Given incarcerated youths’ well-documented reproductive health disparities compared with non-incarcerated adolescents, the identified gaps represent important opportunities for future research and programmatic emphasis.
- juvenile justice
- incarcerated youth
- reentry
- reproductive health
Statistics from Altmetric.com
Key messages
Youth undergoing community reentry after incarceration have high reproductive health needs.
The limited available research focuses on frequency of sexual risk behaviours, such as lack of condom use, as well as prevalence of sexually transmitted infections.
A literature gap exists on hormonal contraceptives for youth undergoing reentry. Additionally, existing intervention studies are few, but promising; more intervention studies are needed.
The literature suggests that developing and implementing gender-specific interventions can potentially improve the reproductive health outcomes of youth underoing reentry after incarceration.
Introduction
Reproductive health needs of incarcerated youth
Worldwide, incarcerated youth, defined as young people less than 18 years of age who are involuntarily detained, face disproportionate medical morbidity and mortality compared with non-incarcerated peers.1 2 Addressing their reproductive health needs represents a crucial opportunity to improve their overall health.3 A nationally representative United States (US)-based study found that one-third of incarcerated girls reported ever being pregnant,4 compared with 2% of US adolescent girls aged 12–17 years, generally.5 The same study reported that 12% of incarcerated girls and boys were expecting a child.6 Rates of sexually transmitted infections (STIs) among incarcerated youth are also high. In the US, mean prevalence rates for chlamydia and gonorrhea are three and two times as high among incarcerated girls and boys, respectively, as among girls and boys from the general adolescent population.7 Although detention facilities address youths’ reproductive health needs while they are detained, although to varying degrees, the extent to which they access care on release is unclear.8
Underlying inequities in social determinants of reproductive health and care access contribute to high vulnerability among these young people.9 10 Most incarcerated youth come from racial and ethnic minority groups and return to communities strongly impacted by disparities in healthcare access.11 12 Within the US, despite the significant decline in the number of youth in custody over the last decade, the detention rate of youth of colour in 2015 remained more than three times that of white youth.12 Further, many racial and ethnic disparities overlap with socioeconomic disadvantage, which may have direct effects on youths’ reproductive health. For example, girls from racial and ethnic minority groups are less likely to receive birth control than White girls,13 and lower average household income is correlated with higher teen birth rates.14 Additionally, rates of prior adverse childhood experiences, such as sexual abuse, are high among incarcerated youth15 and link to negative reproductive health outcomes, such as increased rates of STIs.16 High rates of mental health disorders and substance use in the incarcerated youth population also increase reproductive health risk.17 Thus, incarcerated youth face a combination of risks that adversely affects their reproductive health.17
The reentry period
Youths’ abrupt transition from incarceration back to the community, often termed reentry, is challenging.18 Recently incarcerated youth reentering their community represent a population often overlooked in the health literature.9 In 2016, over 65 000 youth were sentenced to juvenile justice residential facilities in the US alone.12 The average duration of youth incarceration in the US is 3 months, and many youth cycle in and out of detention facilities that disrupt their schooling, healthcare access, and community connections.19 20
During the reentry period, youth and their families navigate multiple bureaucratic systems (eg, child welfare, school, health, immigration) while simultaneously contending with juvenile court and probation systems.21 Many become re-exposed to home or neighbourhood violence, heightening the chances of recidivism and adverse health outcomes.18 Most incarcerated youth express plans to reform, but successful transitions require multiple levels of support – support that systems of care often fail to provide.22 Studies have found that up to 75% of released adolescents are re-arrested within 3 years.23 During reentry, many youth engage in substance use and unprotected sexual activity that increase their risk for poor health outcomes.18 Understanding and addressing youths’ reproductive health needs during reentry is crucial to improving the health outcomes and life trajectories of these young people.
Given the high reproductive health needs observed in incarcerated youth and the strong potential impact of intervention in this area,24 this area is an important focus. Yet the intersection between youths’ reproductive health needs and reentry is underexplored.18 The objective of this systematic literature review was therefore to describe the reproductive health needs of youth undergoing reentry after incarceration.
Methods
Search strategy
We identified peer-reviewed original research studies published in English-language sources using the online databases PubMed, CINAHL, Cochrane Library, and Google Scholar. Search dates were from inception of the PubMed, CINAHL and Cochrane Library to 20 January 2017. The inclusion data for the Google Scholar search was the period 11 January 1990–20 January 2017. The search terms used to identify relevant articles included keywords related to the concepts: incarceration child or adolescent, and reentry. This approach enabled us to capture all articles relevant to health in the databases. We developed the search terms in close consultation with a biomedical librarian at our university. We ran several combinations of terms to identify the search terms that would result in the most inclusive search.
The final search terms did not miss any of our ‘test’ articles that we knew to be relevant before running the search. However, to ensure completeness of the search, we additionally searched the terms ‘reentry’ and ‘youth’ in the ‘What Works’ database in the Reentry Clearinghouse of the US federally-funded National Criminal Justice Reference Service. We also hand-searched the reference lists of relevant review articles to identify articles potentially missed by our electronic search. Finally, to further ensure the search had not missed articles, an expert academic reviewer and correctional health policy leader external to the research team reviewed our list of included articles and provided feedback to the study team.
Selection criteria
Using broad criteria, we conducted a systematic search for English-language, peer-reviewed publications reporting on the reproductive health of youth exiting incarceration. Once we had identified all the articles relevant to health, we manually conducted title and abstract review to identify articles potentially relevant to ‘reproductive health’, applying the World Health Organization (WHO) definition of reproductive health.25 Specifically, we defined ‘reproductive health’, in accordance with the WHO definition, as encompassing physical, mental and social well-being, as well as the absence of disease, in all matters relating to the reproductive system.25
The population of interest included all youth up to 18 years of age who had previously been incarcerated and were in the reentry period. Here, we defined the reentry period as within 1 month prior to release (given the reentry planning that occurs prior to release) and up to 18 months after release from incarceration (given the decline in data collection after 18 months post-release among intervention studies). Studies that focused on individuals over 18 years of age were excluded because individuals older than 18 are generally processed through the adult justice system rather than the juvenile justice system. We focused on identifying youth reentry studies regarding any aspect of reproductive health. We sought articles on both young men and young women; we did not apply a gender distinction during the search process. The online supplementary appendix 1 provides Boolean search terms for each database.
Supplemental material
Exclusion criteria
We excluded studies based on the following criteria: (1) study focused solely on individuals 18 years or older; (2) data collection occurred outside the reentry period of 1 month prior to and 18 months after release from incarceration; (3) study did not address any aspect of reproductive health (ie, focused only on other aspects of physical health, mental health, or substance abuse); (4) publication was not a research study (eg, literature reviews or book chapters); (5) data were collected in a country that was not part of the Organisation for Economic Co-operation and Development (OECD), given the chosen emphasis to focus on youth justice systems in developed countries; and (6) abstract not available or non-English.
Data extraction
Two team members (AS, whose work was verified by EB) applied a structured instrument to extract key information from the included articles. The instrument was derived from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist26 and the Cochrane Handbook. 27 Extracted information for each study included the following: title; authors; study type; study population; intervention design; study population, including age, gender, race/ethnicity, and inclusion and exclusion criteria; duration and frequency of data collection; and data pertinent to ‘reproductive health,’ as per the WHO definition of reproductive health.25 During extraction, we extracted data on gender-specific findings, when relevant, according to the gender classifications (eg, ‘boy’ or ‘girl’) applied in each study.
Study quality assessment
Methodological quality was assessed for each article by a research team member (AS) and verified by EB using the validated Hawker et al appraisal checklist to systematically review disparate data.28 29 Given the multidisciplinary nature of the literature regarding youth reentry, this checklist was chosen for its adaptability in assessing quality of heterogenous studies, including across data type and disciplines. Assessed areas included: abstract and title; introduction and aims; method and data; sampling; data analysis; ethics and bias; results; transferability or generalisability; and implications and usefulness. Each area was associated with a numerical score of 1 to 4 (1-very poor, 2-poor, 3-fair, 4-good) for a summed score ranging from 9 to 36.28
Results
The search yielded a total of 2187 articles. After applying exclusion criteria, 13 articles remained (search and extraction process detailed in figure 1). After expert review and checking the reference lists of relevant review articles uncovered in the search, one additional article was added. Thus, a total of 14 articles were included for data extraction. The 14 articles addressed frequency of condom use (eight articles), sexual risk behaviours other than lack of condom use7 and STI prevalence.3 The definition of ‘sexual risk behaviours’ applied in the review was based on the emergent articles and included: unprotected sex, sex while under the influence of alcohol or drugs, exchanging sex for drugs or alcohol, multiple sexual partners, or multiple sexual acts. The articles varied in quality, with Hawker scores ranging from 25 to 34 (out of 36); all but two of the articles were rated as fair or good quality. table 1 summarises information about authors, study population, study location, type of study, and Hawker scores. All 14 articles of the studies emergent from the search were conducted in the US.
Summary of articles on youths’ reproductive health needs during reentry
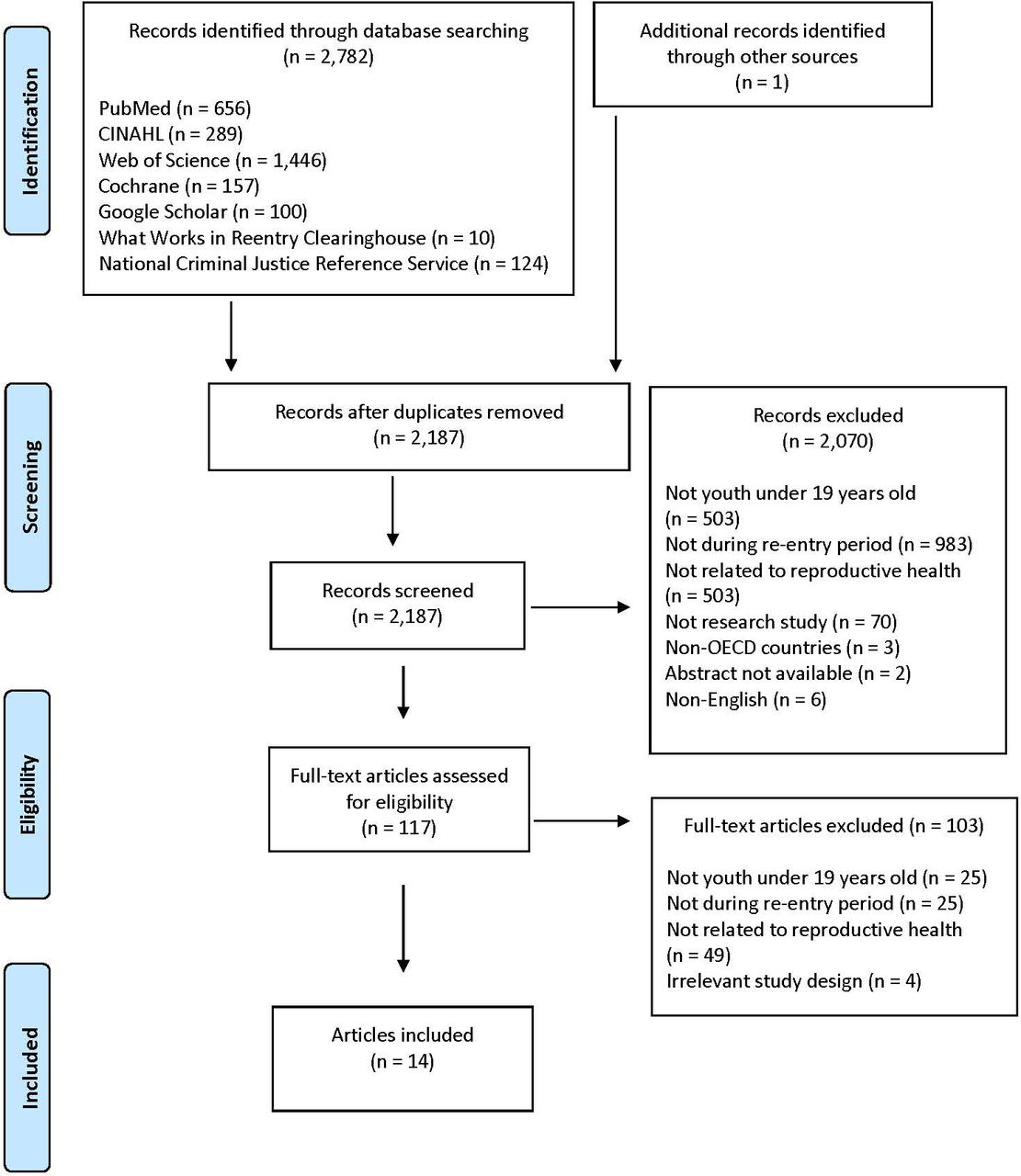
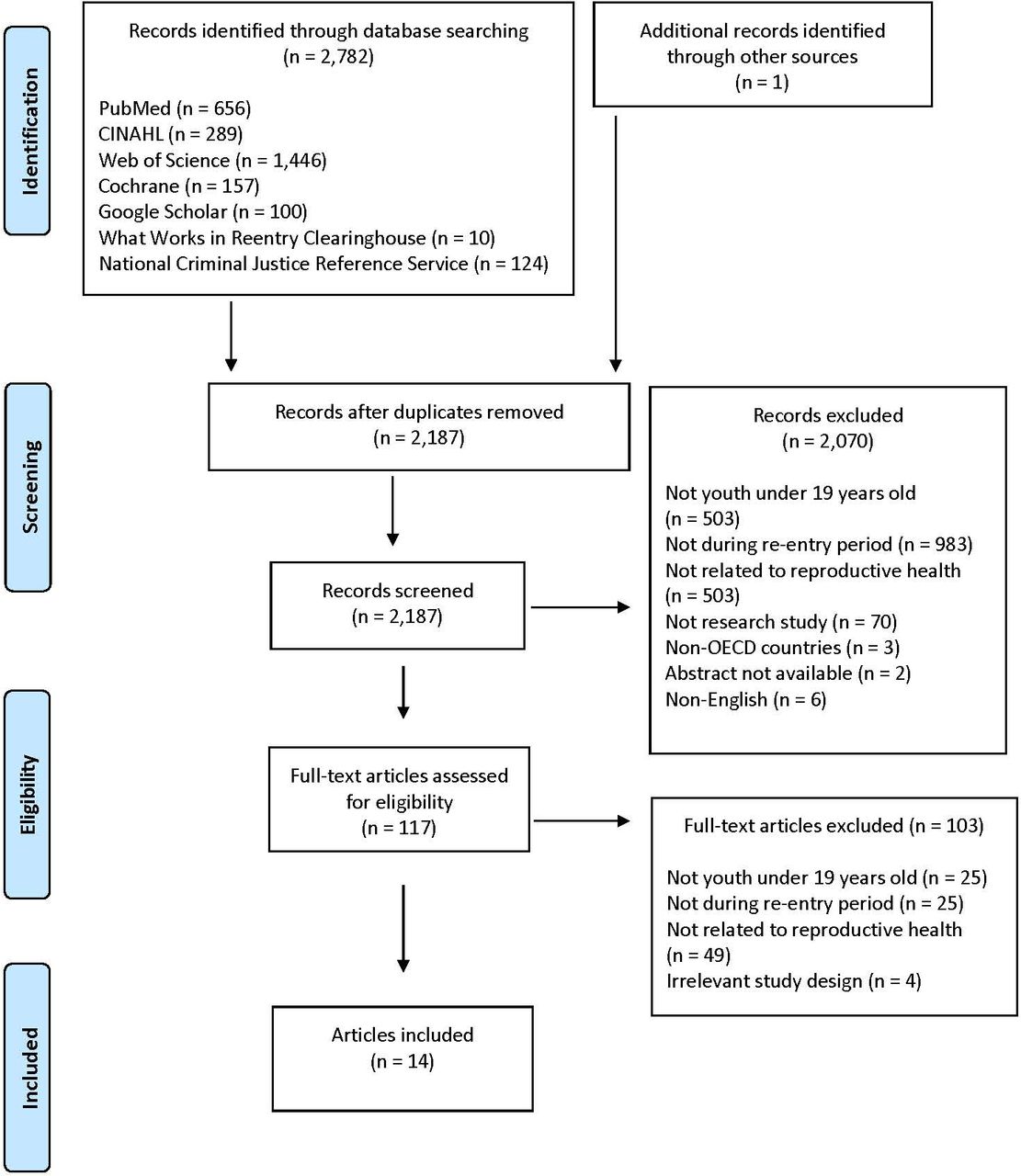{kind=link}
PRISMA diagram of article exclusion and inclusion. OECD, Organisation for Economic Co-operation and Development.
Reproductive health needs of youth undergoing reentry
Most data on reproductive health needs originated from articles on HIV/STI risk reduction interventions. Of the nine articles reporting quantitative data on reproductive health, eight articles reported data on condom use/unprotected sex and seven reported data on other sexual risk behaviours (table 2).
Quantitative studies on youths’ reproductive health needs during reentry
Of the four articles that included data other than sexual risk behaviour, three reported on STI prevalence. Of the 14 included articles, five reported qualitative data on reproductive health issues specific to youth undergoing reentry (table 3).
Qualitative studies on reproductive health needs of youth during reentry
STI prevalence
Although reported STI prevalence rates ranged from 0%–20%, there was general consensus across the articles on the relatively high STI morbidity of youth undergoing reentry. The lowest STI rates were reported in Rowe et al’s randomised controlled trial (RCT) measuring the efficacy of family therapy compared with usual care (outpatient substance use treatment services) for reduction of HIV/STI risk behaviour.30 In this RCT, positive STI test results for the 154 participants total – all recently incarcerated adolescents with substance use histories – ranged from 0%–4% in a series of follow-ups conducted at 3 to 18 months after release.30 In contrast, other studies reported much higher ranges of STI prevalence. In the Robertson et al RCT, 46 adolescent females were randomised into either a health education programme or a HIV risk reduction intervention. Sexual risk behaviour was assessed after release.31 Both groups maintained rates of gonorrhea and chlamydia between 17%–20% while detained and at the 9-month follow-up after release. Though Robertson et al's study n was limited at 46, DiClemente et al provide additional evidence of high STI prevalence, with 14%–20% of adolescents testing positive for any bacterial STI at 3 and 6 months after release.32 These high rates were partially explained by the authors’ citing relatively higher engagement in sexual risk behaviours compared with a general population of youth, such as inconsistent condom use, engaging in sexual intercourse while under the influence of drugs and/or alcohol, having multiple partners, and exchanging sexual intercourse for money or drugs (table 2).
STI risk reduction interventions
Though most of the HIV/STI risk reduction interventions demonstrated effectiveness in increasing condom use, efforts to reduce sexual risk behaviours yielded mixed but promising results (table 2). Freudenberg et al described a RCT comparing the reduction of sexual risk behaviour among 397 adolescent males due to either an intensive jail and community-based intervention versus a single jail-based discharge planning session.33 Neither the intervention nor use of community-based services alone reduced sexual risk behaviours at the 1-year follow-up. However, participants who both received the intervention and utilised community-based services after release were one-third as likely to engage in sexual risk behaviour compared with individuals who received the intervention but did not utilise community services.33 In contrast, Lawrence et al studied 361 adolescent males and found that safer sexual behaviours occurred at the 6-month post-release follow-up regardless of assignment to either a sexual risk reduction intervention or an anger management programme.34 They attributed the decrease in sexual risk behaviour to care and education received while incarcerated rather than to interventions delivered during reentry.34 In summary, across these studies, high rates of sexual risk behaviours were observed and rates tended to decrease over time in some groups, although the precise contributor to the decreased rates could not necessarily be attributed to a particular intervention.
Youth perspectives
The five articles that reported qualitative data on reproductive health described ideas for improving aftercare programme or evaluated youth perspectives on healthcare utilisation (table 3). These studies illustrated youths’ receptiveness to sex education, including within correctional facilities, which can be delivered in a variety of formats, such as via group sessions, or one-on-one by peers or adults, and via telephone during reentry, if connections are established prior to release.35–37
The studies also demonstrated the value of gender-specific programming.35 38 39 Much of the focus was on pregnancy. The single mixed-methods evaluation included, by Jacobs et al, evaluated the Massachusetts Health Passport Project serving recently incarcerated adolescents re-entering their communities.38 Young women reported that they were most concerned with pregnancy, STIs, trauma from prior sexual abuse, involvement in sex trafficking, and hygiene. Young men also reported STIs as a top health concern, but diverged from females on their other health priorities, which included violence-related and sports-related injuries, mental health, and substance use.38 In another qualitative study (Davis et al, 2016), one of the lessons learnt from the implementation of a HIV/STI risk reduction intervention was that addressing girls’ more salient priorities can establish stronger and more effective bonds between youth and providers.35 The interviewed girls expressed their desire to achieve goals that they felt competed with their reproductive health, which included completing their education, improving their personal relationships, anger management, and reducing substance use.35 Thus, there was a pattern of competing priorities across both genders, with boys and girls each expressing gender-specific needs.
Discussion
This systematic review addressed the current state of research on the reproductive health needs of youth transitioning from incarceration back to the community. Overall, there are few published data on this topic. The limited existing literature indicates that youth undergoing reentry have high reproductive health needs and are greatly in need of reproductive health services. Data on the youths’ reproductive health needs predominantly emerge from HIV/STI prevention studies, with studied interventions showing promising results. Safer sexual practices after intervention receipt, such as increased condom use, were observed (eg, Magura et al, 1994),40 highlighting the potential value of interventions during the crucial time period of reentry. The qualitative studies provided a useful exploration of youths’ perspectives on reproductive health education and gender-specific concerns related to reproductive health needs. Taken together, the current literature indicates that more attention to this topic is needed but that potential to reduce youths’ sexual risks during reentry exists.
The widest gap was the lack of clear evidence supporting interventions. While more can be done to describe problems – for example, delineating STI and pregnancy incidences during reentry – the most pragmatic step forward seems to be focusing on developing and testing interventions. The few studies on intervention approaches showed a decreasing trend in the overall high rates of sexual risk behaviour during reentry. Mechanisms need to be clarified regarding these reductions so they can be leveraged to improve outcomes. Another gap in the literature was the lack of articles on hormonal methods of contraception. While several of the articles addressed unprotected sex and/or condom use, none of the articles focused on hormonal contraception. Additionally, sexual orientation was not addressed in the literature. Finally, an additional gap was the lack of studies from outside the US. Although the search was broad, all 14 of the studies were conducted in the US., suggesting an opportunity for research to highlight the reproductive health needs of youth undergoing reentry – and solutions – in other developed countries, as well as in the developing world, which was not a focus of this review.
The existing literature indicates that gender-specific approaches are needed to overcome barriers to meeting youths’ reproductive health needs during reentry. Youth face competing priorities during reentry, which can impede accessing care. Females expressed a high prioritisation of obtaining reproductive health services when they perceived a need for pregnancy prevention and pregnancy-related care. The studies overall showed that youth wanted to receive sex education, especially while incarcerated, which could later encourage reproductive care utilisation during reentry. Provider awareness of youths’ reproductive health education and reproductive healthcare needs – and competing priorities during reentry – can optimise the efficacy of clinical encounters. Additionally, studies to develop and test scalable, cost-effective interventions that provide gender-specific solutions for improving reproductive health outcomes during reentry are needed to extend and build on the current research.
Future directions
The small number of articles identified in our cross-disciplinary search is perhaps the clearest evidence that the reproductive health needs of youth undergoing reentry remain under the public health radar. Although the US National Institutes of Health have disproportionally limited research funding to studies dealing with incarcerated populations,41 and institutional review boards and correctional facilities create bureaucratic hurdles to studies on these populations,2 research in this field should be systematically encouraged to address the research gaps highlighted above.
Practitioners, policymakers and researchers can feel encouraged by the positive outcomes demonstrated in the reentry interventions, indicating that a focus on intervention – both pre- and post-release – is likely worthwhile. In particular, practitioners can use findings from this review to implement interventions and trainings focused on meeting youths’ reproductive health needs during reentry. Many juvenile justice facilities screen for pregnancy and STIs, with youth receiving needed care and treatments while in custody.9 Pre-release planning that anticipates reentry needs and continues to address youths’ reproductive health concerns during reentry can further prevent and treat STIs, decrease the rate of unintended pregnancy, and facilitate teen pregnancy being as transformative and healthy as possible.42
Additionally, increased awareness of the reproductive health and social challenges that youth face during reentry would allow reproductive health professionals to deliver more complete care.
A diverse range of healthcare professionals addresses reproductive health in the community – including primary care providers, emergency department physicians, school nurses, and obstetrics-gynaecology providers – creating varied points of access to reproductive healthcare. Reproductive health professionals attuned to the unique challenges and opportunities of reentry have the potential to be hugely impactful.
Limitations
Our systematic review has several potential limitations. Given the multidisciplinary nature of research on youth involved in the justice system, our approach was to conduct broad, systematic searches of select literature databases to ensure that we captured all relevant articles. However, the search concept (‘reproductive health’) was broad, which limits the specificity of the results. Also, incarceration type and duration varied. Some interventions studies included a pre-release component, while others did not. Additionally, all of the articles resulting from the search were conducted in the US, which limits the applicability to other countries and suggests a need for an international research focus on the reproductive health needs of youth exiting incarceration. Correctional systems and health systems in countries outside of the US may differ considerably, as does societal context. Culture differences in youths’ attitudes towards reproductive health, norms regarding youths’ sexual behaviour, and preferences for reproductive care and contraceptive care, as well as country-specific variation in prevalence of STIs, limit the generalisability of the findings. Another limitation is that we excluded articles that only pertained to non-reproductive health aspects of physical health (very few articles) or to mental health. We chose to focus specifically on reproductive health because of the well-documented and impactful high reproductive health needs observed among incarcerated youth undergoing reentry. Despite these limitations, the literature review points to clear gaps in the current literature that signify ripe opportunities for future research.
Conclusions
Lessons learnt from the review indicate a literature gap on youths’ reproductive health needs during reentry worth addressing, and also highlight the potential for impact of interventions aimed at reducing youths’ sexual risk behaviour during reentry. Needs according to gender and sexuality should be further explored. Juvenile incarceration and its aftermath should be recognised as a public health priority. Practitioners, researchers and policymakers have an opportunity to improve the reproductive health of youth returning to their communities after incarceration. Dedication to this marginalised youth population may make a lasting improvement on the health of adolescents as they transition into adulthood, thereby narrowing the growing racial/ethnic and socioeconomic health disparity in our society.
References
Footnotes
Contributors EB, AS, LA and PLC collaborated on all aspects of the review including, design, search strategy, extraction, interpretation, and preparation of the manuscript. EB and AS conducted the extraction process.
Funding The study was funded by UCLA CTSI KL2 Program/NIH-NCATS (#ULTR00124) and by the UCLA Children’s Discovery and Innovation Institute.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.