Article Text

Statistics from Altmetric.com
Improving the provision of postnatal contraception (PNC) has been a topic of great attention recently, especially since the publication of the FSRH guideline Contraception After Pregnancy.1 Many Trusts across the UK are currently working hard to implement changes to improve uptake of effective PNC, including our service in Leeds. We would like to inform Journal readers about our pilot study that we ran in 2019.
Leeds has two maternity hospitals: Leeds General Infirmary and Saint James’ University Hospital. Prior to this pilot study, no contraception was offered routinely before or at the time of postnatal discharge. A previous local study among postnatal women showed a theoretical demand for contraception provision prior to discharge.2 To address this, and to raise awareness among staff, Leeds Sexual Health (LSH) provided an outreach service to postnatal wards for a 3-month period.
During this pilot, a doctor or nurse visited one morning per week to discuss and provide contraception to women on postnatal and transitional care wards. The methods offered included the progestogen-only pill (POP), implant and injection. Additionally, outreach staff were able to counsel and book appointments for women to attend LSH for intrauterine contraception fitting.
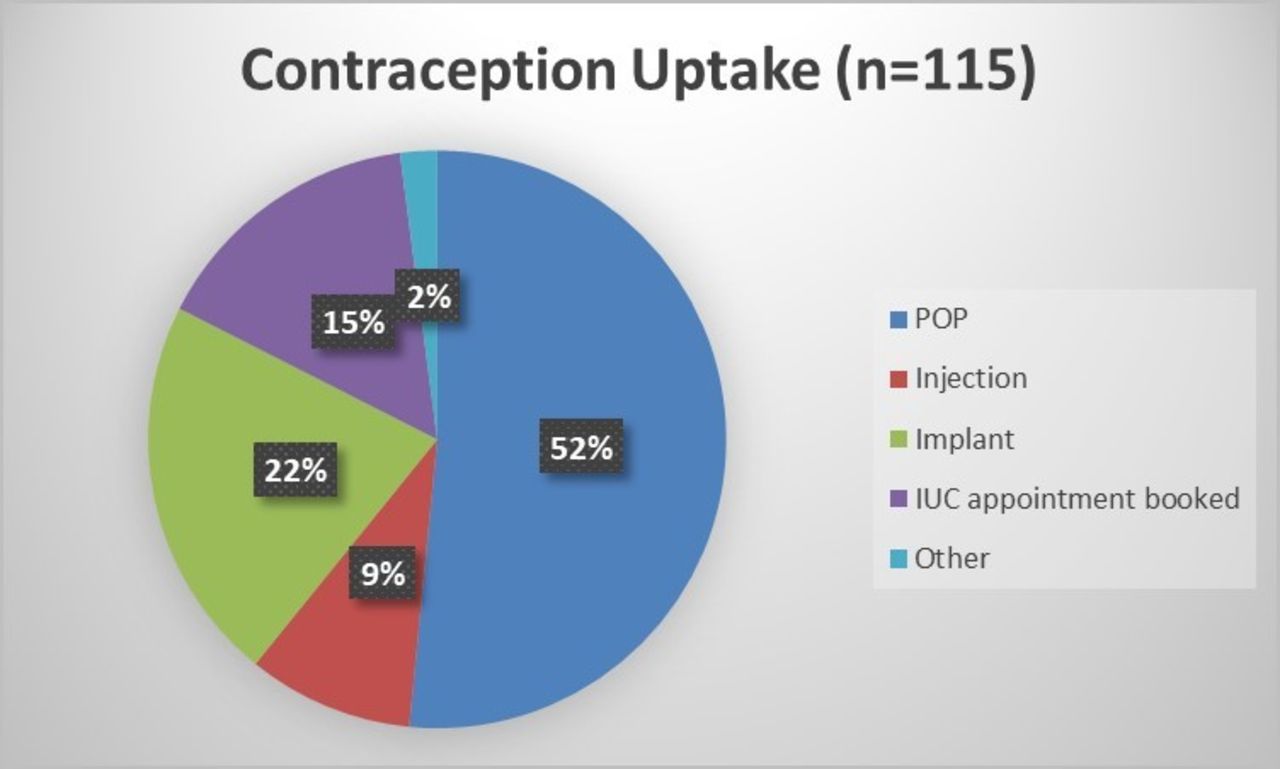
Over a 20-week period (5 February to 26 June 2019) there were 26 visits across both hospitals and 115 women accepted contraception discussion and supply, including a number with medical problems and comorbidities for whom effective contraception improved their future health safety profile (figure 1).

{kind=link}
Contraception uptake among women on the ward (n=115). IUC, intrauterine contraception; POP, progestogen-only pill.
A small number of women (15), who had received a variety of contraceptive methods, gave feedback on their experience 3 months after the pilot. At this time 13 women were still continuing with their chosen method. The two women who had discontinued (both POP) named dissatisfaction with bleeding patterns as their reason for stopping. Of the 15 women who responded, 11 were ‘very happy’ with the provision of contraception taking place on the postnatal ward with the remaining four reporting being ‘fairly happy’. The feedback cited the high quality of the service and its convenience.
In line with other studies,3 4 our data demonstrate the missed opportunity to provide women with ongoing contraception after pregnancy. Unfortunately, the response rate at 3 months was poor (13%) and consequently information regarding rates of method continuation and satisfaction is lacking. However, this pilot study does show that there is an unmet demand for PNC prior to discharge from hospital and that the feedback from women regarding this novel service was very positive. This was only a brief pilot study and is, at present, not sustainable in the long term as it was conducted by staff from another service (LSH) and LSH also provided the contraceptive supplies.
Despite its brevity, we believe this pilot study had a wider impact on raising the awareness of PNC in the maternity services. It encouraged both patients and staff on the postnatal wards to think and talk more about PNC and provided a welcome opportunity for us to raise awareness and provide education and training on this issue. Our key messages are that this service was well received by staff and women and that the contraceptive uptake demonstated that there is a demand for this service. We plan to use this pilot to support our cause for implementing long-term, sustainable and effective initiatives to improve in-hospital contraception provision, and we hope that those healthcare professionals reading this letter will feel inspired to take similar action within their own Trust.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.