Article Text

Statistics from Altmetric.com
Key messages
Women who were obese were more likely to use long-acting reversible contraception (LARCs) and less effective contraceptive methods or no contraception.
Women using LARCs and less effective contraceptive methods or no contraception were more likely to be current smokers.
High levels of psychological distress were most likely among women using LARCs, condoms or no contraception.
Introduction
Prevention of unintended pregnancy remains of public health significance, particularly among young women. A recent national Australian study reported that 26% of women had experienced an unintended pregnancy, and a quarter of these pregnancies were unwanted.1 Young women (aged 20–29 years) were most likely to report an unintended pregnancy. Although contraception is widely available in Australia, the women in this study who reported unintended pregnancies were less likely to be using contraception at the time of conception.1 The relatively high prevalence of unintended, unwanted pregnancies suggests that barriers to contraception remain for a substantial proportion of Australian women. Young women may have different needs regarding contraception than their older peers, however, there is limited population-based research.
Women’s reasons for contraceptive use (and non-use) appear to depend on intersecting individual, social and healthcare factors.2 Women’s decisions about contraception are also influenced by, and change in response to, their physical and emotional health.3 However, the few studies examining women’s physical and mental health and contraceptive use are largely based on small, cross-sectional studies and have reported inconsistent findings. For example, researchers suggest that women reporting symptoms of depression are more likely to use both highly effective (eg, long-acting reversible contraception (LARC))4 5 and less effective methods of contraception and no contraception.6–8 Although the association between depression and contraceptive use may depend on the recent reproductive history of the woman, studies examining women seeking contraception following abortion have also reported conflicting findings.8 9
Regarding women’s physical health, a somewhat similar conflicting pattern of findings is also evident for body mass index (BMI), with obesity most consistently associated with effective contraception methods10–12 and to a lesser extent less effective methods (eg, condoms) and no contraception.10 12 Physical health is also strongly related to health behaviours; however, studies examining the associations between health behaviours and women’s contraceptive use are scant. Although a large population-based study with young Australian women reported that smoking and alcohol use were associated with overall contraceptive use,13 the study did not examine whether differences emerged by levels of contraceptive effectiveness.
Women’s physical and mental health may have a strong influence on patterns of contraceptive use. However, evidence that examines physical and mental health, while taking into account sociodemographic and reproductive factors to understand women’s contraceptive use, appears absent from the literature. Further, the factors associated with contraceptive use in early adulthood may be important for understanding the trajectory of contraceptive use across the life course. This study therefore examines the association between young women’s physical and mental health and health behaviours and their contraceptive use over time.
Methods
The Australian Longitudinal Study on Women’s Health (ALSWH) is a national, population-based study focusing on the biological, psychological, social and economic factors relevant to women’s health.14 This paper uses four waves of ALSWH survey data from young women who were aged 18–23 years when first surveyed in 2012–2013. Women were eligible if they were born in the years 1989–1995, lived in Australia, had a valid Medicare number (the universal national health insurance scheme) and if they consented to linking survey data with administrative records on healthcare. Participants were recruited through conventional means (eg, magazine advertising) and online social media (eg, Facebook). Further details of the survey methodology are published elsewhere.15
Women completed annual online surveys about their physical health, mental and reproductive health and health service use. Surveys were only available in English. A total of 17 012 women responded to survey 1 in 2012–2013, with response rates of 70% and 55% at surveys 2 and 3, respectively.15 A total of 4952 women, who responded to surveys 1, 2, 3 and 5 and answered questions about contraception, were included in this study. Survey 4 conducted in 2016 was a shorter survey that did not include a question about women’s contraceptive use; therefore, data were excluded.
Patient and public involvement
Participants were not involved in the study design or the recruitment process. ALSWH findings are disseminated to participants via newsletters, the ALSWH website and social media.
Measures
Outcome variable
At each survey (except survey 4), women were asked whether they used any contraception the last time they had vaginal sex and chose from a list of six options: the pill, condoms, Implanon, Mirena, other contraceptive, none. Women could select all applicable methods; however, women were classified based on the most effective contraception reported. Four categories were created: (1) long-acting reversible contraception ((LARC) defined as the levonorgestrel-releasing intrauterine system (Mirena) or the progestogen-only implant (Implanon)); (2) pill (combined hormonal contraception (CHC) or progestogen-only pill); (3) condoms; (4) other (potentially includes other hormonal, barrier and natural family planning contraceptive methods); and (5) non-user.
Explanatory variables
Information about women’s sociodemographic background and physical, mental and reproductive health was collected and included in analyses (see online supplementary table 1).
Supplemental material
Statistical analysis
χ2 tests and independent samples t-tests were used to compare the characteristics of the young Australian women when first surveyed in 2013 according to method of contraceptive use and to compare women who did, and did not, respond to all four surveys. Results were considered statistically significant if p<0.01. Multinomial logistic regression models using generalised estimating equations, with independent working correlation matrices, were used to account for the repeated measures within individuals over the four survey waves. The longitudinal associations between the explanatory variables (women’s physical and mental health and health behaviours) and the outcome (contraceptive method) were presented as ORs and 95% CIs. The ORs (95% CIs) represent a ‘population-averaged effect’ for the association between the explanatory variables and the outcome over the four survey waves. Women who change contraception multiple times across the surveys contribute data to different contraceptive methods across the survey waves. For each multinomial logistic regression model, women using the pill were used as the reference category.
The association between each explanatory variable and contraceptive method was first examined through a series of univariable multinomial logistic regression models. Analyses were adjusted for key sociodemographic factors related to contraceptive use reported in the literature including age, marital status, education and area of residence.2 13 Other potential confounders including women’s ability to manage on their income and use of a healthcare card did not change estimates by more than 10% and thus were not included in the final models. To examine the effect modification by women’s pregnancy history, sensitivity analyses stratified by women who had ever, and never, been pregnant were conducted (variable described in online supplementary table 1). Sensitivity analyses further stratified by women who had ever been pregnant with a history of termination/unplanned pregnancy were also conducted. All statistical analyses were performed using SAS software V.9.4.
Results
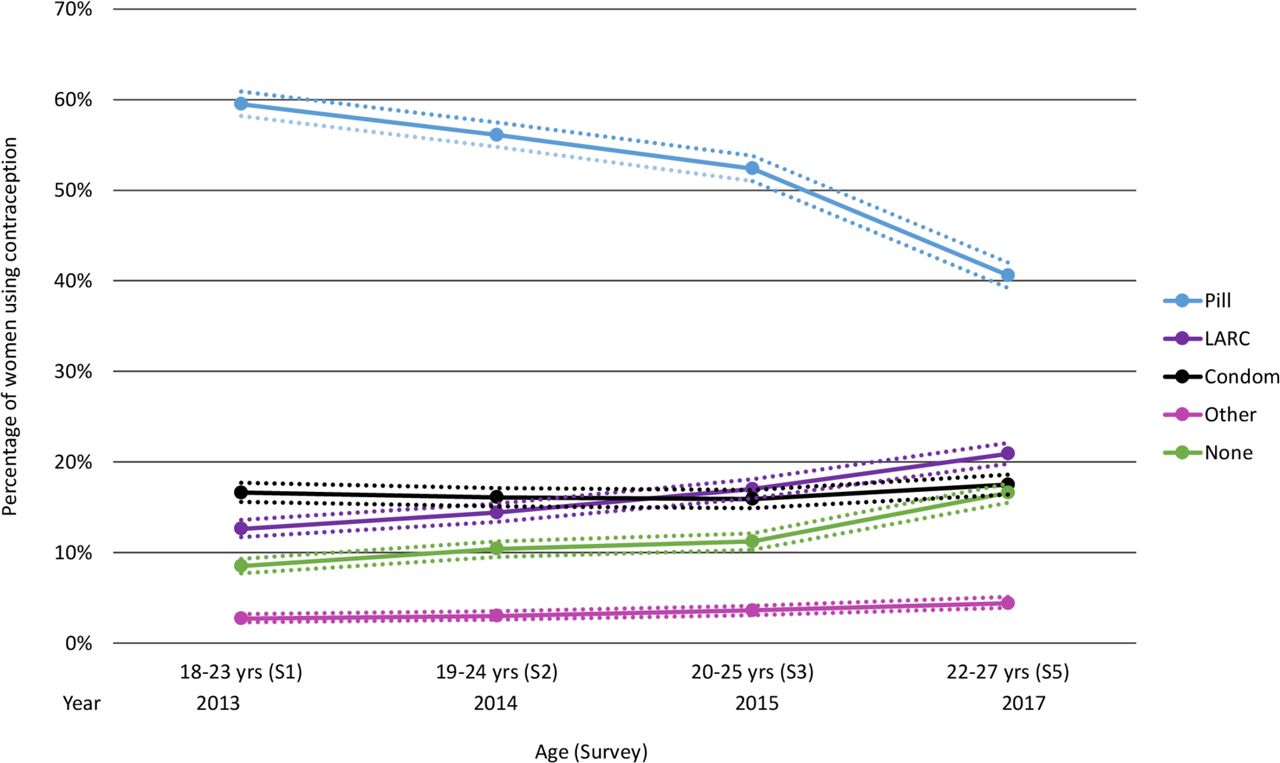
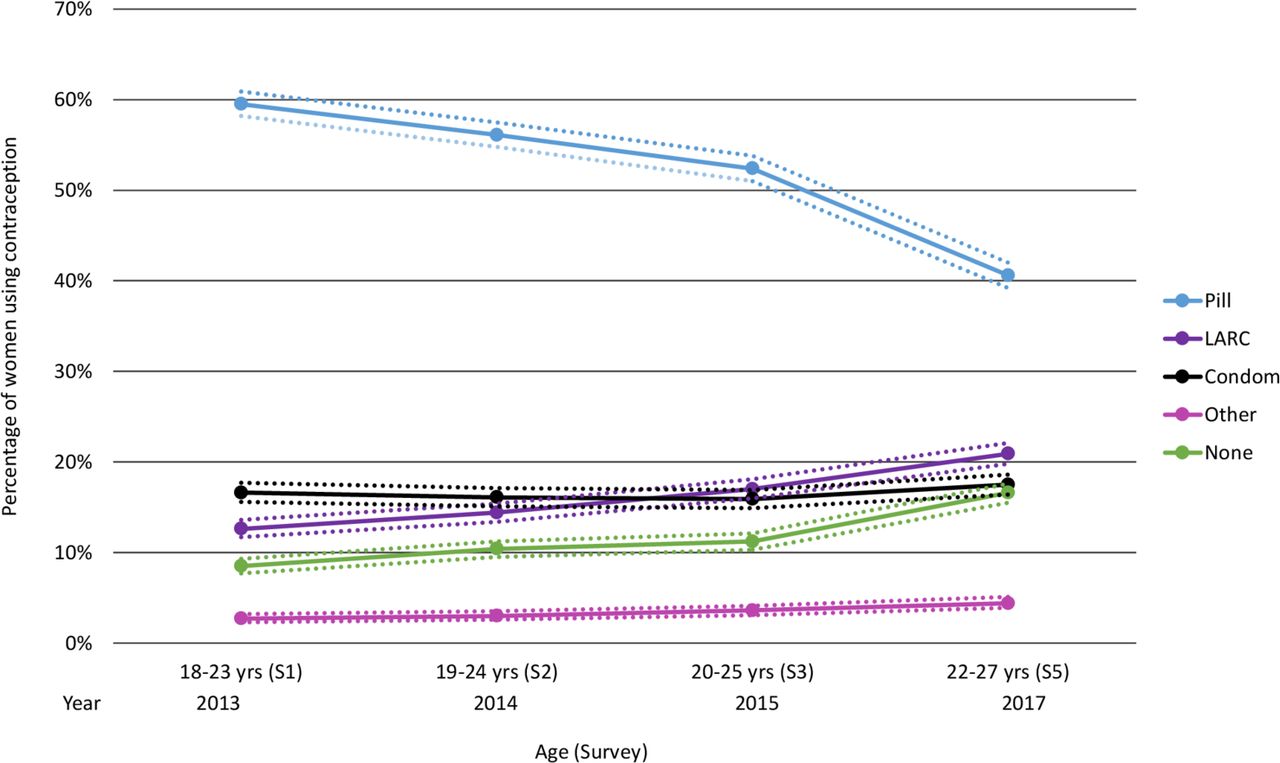
When the women were aged 18–23 years (survey 1), 60% (95% CI 58% to 61%) of women reported using the pill the last time they had sex but this decreased to 41% (95% CI 39% to 42%) by ages 22–27 (survey 5; see figure 1). Women using LARCs increased from 13% (95% CI 12% to 14%) to 21% (95% CI 20% to 22%) as did non-users from 9% (95% CI 8% to 9%) to 17% (95% CI 16% to 18%). At survey 1, women who did not use contraception were most likely to be older, married, have fewer than 12 years of education and report difficulty managing on their income. They were also most likely to have a history of live birth, miscarriage and unplanned pregnancy (table 1).
Characteristics of young Australian women when first surveyed in 2013 according to contraceptive method (n=4952)
{kind=link}
Percentage of women using each contraceptive method over the period 2013–2017 for the same Australian women. Dotted lines represent 95% CIs. LARC, long-acting reversible contraception.
Physical and mental health factors were also associated with contraceptive use (and non-use) over time (see online supplementary table 2). A multinomial logistic regression model adjusting for key sociodemographic variables examined associations between women’s physical and mental health over time and method of contraception (table 2). Compared with women using the pill, women using LARCs had higher odds of being overweight or obese relative to normal weight women and higher odds of being current smokers than never smokers. Women using LARCs also had higher odds of reporting fair or poor general health and very high levels of psychological distress. Women using condoms had higher odds of being overweight or obese, ex-smokers or current smokers, consumers of alcohol and reported fair or poor general health and very high levels of psychological distress compared with women using the pill. Women using other contraception had higher odds of being overweight or obese and ex-smokers or current smokers compared with women using the pill. Compared with women using the pill, women using other forms of contraception also had higher odds of moderate and very high levels of psychological distress relative to low levels of distress. Women not using contraception had higher odds of being overweight and obese, ex-smokers or current smokers, consumers of alcohol and reported fair or poor general health and very high levels of psychological distress compared with women using the pill.
Longitudinal associations between physical health, health behaviours and mental health and contraceptive use and non-use among young women (n=4952)
In analyses stratifying by women who had ever, and never, been pregnant, the results for women who had never been pregnant were similar to the results for women overall (see online supplementary table 3). By comparison, the results for women who had ever been pregnant differed (see table 3). Specifically, among women who had ever been pregnant, women using LARCs had higher odds of being obese compared with normal weight women using the pill. Women who had ever been pregnant and who were using condoms were less likely to report good levels of general health than women using the pill. Women who had ever been pregnant and who were using other forms of contraception were less likely to be consumers of alcohol compared with women using the pill. Women who had ever been pregnant who were not using contraception had higher odds of being obese than normal weight women using the pill. There were no associations between smoking and psychological distress and women’s contraceptive use among women who had ever been pregnant. These results did not appreciably differ in analyses further stratifying by a history of unplanned pregnancy or termination only (see online supplementary table 4).
Longitudinal associations between physical health, health behaviours and mental health and contraceptive use and non-use among women who have ever been pregnant
Discussion
Overall women who were obese, smokers, in poor general health and with high levels of psychological distress were more likely to use both highly effective (LARCs) and less effective methods or no contraception. A few previous studies have shown that depression and obesity are associated with highly effective and less effective contraceptive methods,6–8 10–12 but results overall have been conflicting. In this study, findings varied by pregnancy history. Among women who had ever been pregnant, obesity remained strongly associated with contraceptive use and non-use, but psychological distress and smoking did not. Other social and healthcare factors may better predict the contraceptive use of women who have been pregnant. Our findings further support the complexity of contraceptive decision-making.2 The results reinforce the need for health professionals to consider a woman’s reproductive history and desire for future pregnancies while also considering mental and physical health issues.
Women’s health and well-being concerns influence contraceptive decision-making. In a systematic review, fears about weight gain were identified as barriers to LARC use.16 Similarly, a recent Australian study found that women reporting body management (including weight) as a reason for contraceptive use were less likely to use LARC.17 Qualitative research has also described how women change or discontinue contraception due to weight gain or mood problems.3 18 These concerns might explain our findings of associations between obesity, poor general health and psychological distress and contraceptive non-use. At the same time, we found that obesity, poor general health and psychological distress were also associated with LARC use. The importance of preventing unintended pregnancy17 may facilitate uptake of LARCs among women with pre-existing physical and mental health concerns.
The relationship between obesity, smoking, depression and contraception is influenced by social and healthcare factors. Women are guided by the knowledge and preferences of their healthcare professional.19 Obesity, smoking and mental health issues may create additional complexity for prescribers. Mental health problems may influence women’s ability to consistently use contraception20 and there may be increased risks of psychological side effects,21 which may influence health professional recommendations. The UK Medical Eligibility Criteria does not typically recommend CHC for women with a BMI ≥35 kg/m2, particularly if they also smoke.22 Adherence to these recommendations in Australian clinical practice is endorsed,23 and may explain the decreased odds of CHC use among women who were obese and current smokers in our study. Because of the potential health risks of CHC among young women who are obese our findings are reassuring. On the other hand, it is possible that misconceptions about the safety of certain contraceptive methods for young women who are obese24 may adversely impact women’s contraception use.25
Women’s physical and mental health are embedded within the social context. The women in this study who used LARCs were more likely to reside in rural areas and to report a history of sexually transmitted infections (STI). Women who live in rural areas can have geographical barriers accessing contraception and may rely on LARCs for their long-term contraceptive effectiveness, but in doing so are not protected from STIs. Further, women who used no contraception in our study were less likely to have completed high school or university and more likely to be current smokers. Young women from disadvantaged backgrounds may have poor access to contraception and to contraceptive-related education and information than their peers from advantaged backgrounds, limiting their access to contraception. On the other hand, increased contact with health professionals among women who have been pregnant may increase opportunities for women to discuss their contraceptive needs.
We examined a range of physical and mental health factors associated with different contraceptive methods over 5 years. Contraception use was measured annually and so precluded assessment of changes over the course of the year. We relied on women to accurately self-report their contraceptive use and were also limited by the survey question on contraceptive use, which only included the more common methods used and may not reflect the full range of methods used over time.
It is difficult to establish whether women’s health outcomes influenced their contraceptive use or changed following use and therefore we cannot assume causality. Finally, the analyses only included women who responded to all four survey waves and who answered questions about contraceptive use. Women responding to all four surveys were more likely to be older, in a relationship, university educated, a non-smoker and reported better physical and mental health than the women who inconsistently responded or who withdrew. Thus, our study may underestimate the associations between obesity, depressive symptoms and contraceptive use.
Our findings suggest that physical and mental health are an important factor in young women’s contraceptive use (and non-use). Improving the support and education available to health professionals may better assist them to support women with physical and mental health issues. Targeting supportive services to women who are obese, smokers and who report mental health problems may optimise contraceptive care and decision-making.
Data availability statement
Data are available upon reasonable request. The data underlying this study are owned by the Australian Government Department of Health. The process for data access is documented on the Australian Longitudinal Study on Women’s Health (ALSWH) website (http://www.alswh.org.au) which includes all the survey questionnaires, data books of frequency tables for all surveys, metadata, conditions of data access and request form. Data may be made available to collaborating researchers where there is a formal request to make use of the material. Permission to use the data must be obtained from the Data Access Committee of ALSWH.
Ethics statements
Ethics approval
The study has ethics approval from The University of Queensland (UQ) and The University of Newcastle (UoN) Human Research Ethics Committees (HREC).
Acknowledgments
The research on which this paper is based was conducted as part of the Australian Longitudinal Study on Women’s Health, The University of Newcastle and The University of Queensland. We are grateful to the Australian Government Department of Health for funding and to the women who provided the survey data.
References
Footnotes
Twitter @IngridRowlands, @jacaluc
Contributors IJR made substantial contributions to the conception and design of the study and conducted the statistical analyses and drafted the manuscript. GDM made substantial contributions to the acquisition of the data, the interpretation of the results and critical revision of the manuscript for intellectual content. JCL made substantial contributions to the conception and design of the study, the interpretation of the results and critical revision of the manuscript for intellectual content. All authors read and approved the final manuscript.
Funding GDM is supported by an Australian National Health and Medical Research Council Principal Research Fellowship (GNT1121844). The ALSWH is funded by the Australian Government Department of Health.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.