Article Text

Abstract
Introduction Women on Web (WoW) is a global medical abortion telemedicine service operating outside the formal health sector. In April 2019 they opened their helpdesk to Germany. Our aim was to understand the motivations, and perceived barriers to access, for women who choose telemedicine abortion outside the formal health sector in Germany.
Methods We conducted a parallel convergent mixed-methods study among 1090 women consulting WoW from Germany between 1 January and 31 December 2019. We performed a cross-sectional study of data contained in online consultations and a content analysis of 108 email texts. Analysis was done until saturation; results were merged and triangulation used to validate results.
Results The quantitative analysis found that the need for secrecy (n=502, 48%) and the wish for privacy (n=500, 48%) were frequent reasons for choosing telemedicine abortion. Adolescents were more likely to report secrecy, cost, stigma and legal restrictions as reasons for using telemedicine abortion compared with older women. The content analysis developed two main themes and seven subsidiary categories, (1) internal motivations for seeking telemedicine abortion encompassing (i) autonomy, (ii) perception of external threat and (iii) shame and stigma, and (2) external barriers to formal abortion care encompassing (iv) financial stress, (v) logistic barriers to access, (vi) provider attitudes and (vii) vulnerability of foreigners.
Conclusions Women in Germany who choose telemedicine abortion outside the formal health sector do so both from a place of empowerment and a place of disempowerment. Numerous barriers to abortion access exist in the formal sector which are of special relevance to vulnerable groups such as adolescents and undocumented immigrants.
- abortion
- induced
- health policy
- health services accessibility
- qualitative research
- reproductive health
- reproductive rights
Data availability statement
All original data are available upon reasonable request to the researchers.
Statistics from Altmetric.com
- abortion
- induced
- health policy
- health services accessibility
- qualitative research
- reproductive health
- reproductive rights
Key messages
When Women on Web, an abortion telemedicine service operating outside the formal healthcare sector, opened in Germany in April 2019, 1208 women consulted the service in the first 9 months.
Women who choose telemedicine abortion do so both from a position of empowerment, for reasons of autonomy, and from a position of disempowerment and lack of autonomy.
Numerous barriers to abortion access, as permitted by German law, exist in the formal health sector, which may most impact vulnerable groups such as adolescents, women with low financial means and undocumented immigrants.
Introduction
In April 2019 Women on Web (WoW), an abortion telemedicine service usually serving settings where abortion is legally restricted, opened their helpdesk to Germany. Between April and December 2019, consultations increased from 44 to 193 per month, suggesting a demand for abortion services not being met in the formal health sector. The WoW consultation process has been described previously.1 2 Based on available data, abortion by telemedicine has similar clinical outcomes to in-person abortion, and women choose telemedicine abortion for a multitude of reasons.3 4
In Germany elective abortion is technically illegal but formally allowed through a legal clause that permits abortion up to 12 weeks’ gestation through a ‘consultation process’ entailing an appointment with a state-approved agency, 3 days' reflection, and a physician-administered abortion.5 The advertisement of abortion services, however, can technically be penalised with imprisonment, and conscientious objection, the possibility of by law refusing to provide abortion care for personal beliefs, is permitted.5 Abortion providers are asked to register with the General Medical Council but this information is not accessible to the public.6 7 In 2018, 100 986 abortions were performed in Germany, of which 96.2% occurred through the consultation process.8
To our knowledge, there are no studies on why women in Germany opt for abortion outside the formal health sector. Our aim was to understand the motivations, and perceived barriers to access, for women in Germany choosing telemedicine abortion over formal services.
Methods
We performed a convergent parallel mixed methods study consisting of a cross-sectional study and a content analysis. Both data components were collected simultaneously, analysed independently but accorded equal weight, and merged for interpretation. We triangulated the data to validate results.
Cross-sectional analysis
We retrieved and included anonymised data from all unique consultations sent to WoW from women living in Germany, excluding US military bases, in German or English, between 1 January and 31 December 2019.
We summarised participants' background characteristics and evaluated associations between age categories, population size of town of residence, immigration status, and reasons for choosing telemedicine abortion, selected from a list of 16 options.
Continuous data were summarised as medians and interquartile range (IQR) and categorical data as frequencies (tables 1 and 2). Associations between sociodemographic characteristics and reasons for choosing telemedicine abortion (online supplemental table 1) were assessed using logistic regression and expressed as odds ratios (OR) with 95% confidence intervals (CIs). Data analysis was performed using Stata version 16.0 (StataCorp, College Station, TX, USA, 2016).
Supplemental material
Background and pregnancy-related characteristics of 109 women in Germany requesting an abortion through Women on Web between 1 January and 31 December 2019
Categorical reasons for choosing online abortion over formal abortion services among women in Germany requesting abortion from Women on Web between 1 January to 31 December 2019
Content analysis
After submitting an online consultation to WoW, women in Germany receive an email telling them that abortion is available in the formal healthcare sector followed by this question:
If you feel you are unable to access abortion services in Germany, can you please tell us a bit more about why. […] We will let you know as soon as possible if we can help you in any way.2
We performed a content analysis of the responses to this question. Two researchers (KK and SG) identified the main themes and recurring categories in the text, continuously comparing results. One started from January working forwards and one from December working backwards until saturation was reached, after which a further 28 emails were analysed for confirmation from mid-year 2019.
The complete text was re-read and discussed with a third researcher (ME) for consistency and accuracy. We used systematic coding to categorise and derive subcategories. We analysed the text at the manifest level, using the text’s apparent meaning. We quantified recurring categories to contextualise the findings with the cross-sectional results.
Data validation
We used methodological and researcher triangulation to increase reliability. The cross-sectional and content analysis outcomes were compared and contrasted to nuance findings and identify contradictions.
The study did not include patient–public involvement, but its design was directly informed by contact with the study population, and the objectives formulated in response to this communication. Research arising from WoW data is referenced on their homepage.
The research was approved by the Ethics Committee at Karolinska Institutet, Sweden (Dnr 2009/2072-31/2 and Dnr 2020/05406).
Results
Cross-sectional study
Between 1 January and 31 December 2019 WoW received 1208 consultations from Germany, of which 1090 were included (figure 1).

Number of consultations for medical abortion received by Women on Web per month from Germany in 2019 (n=1090). A total of 1208 consultations received in 2019. Consultations that were duplicate, not in English/Germen, from US millitary bases, or from women not residing in Germany were excluded; final inclusion n=1090. The helpdesk opened in April 2019, and we included the few requests received between January and March as this was the dataset initially requested.
The median age of participants was 29 (±9) years. Median gestational age was 5 weeks+6 days, ranging from 3 weeks+0 days to 18 weeks+1 day. Background characteristics of participants, categorical reasons for requesting telemedicine abortion, and associations to background variables are shown in tables 1 and 2 and online supplemental table 1.
Content analysis
WoW received 255 emails following online consultations from Germany in 2019. Saturation was achieved after analysing 80 emails; a further 28 emails were included for validation. Emails varied in length from 10 to 400 words.
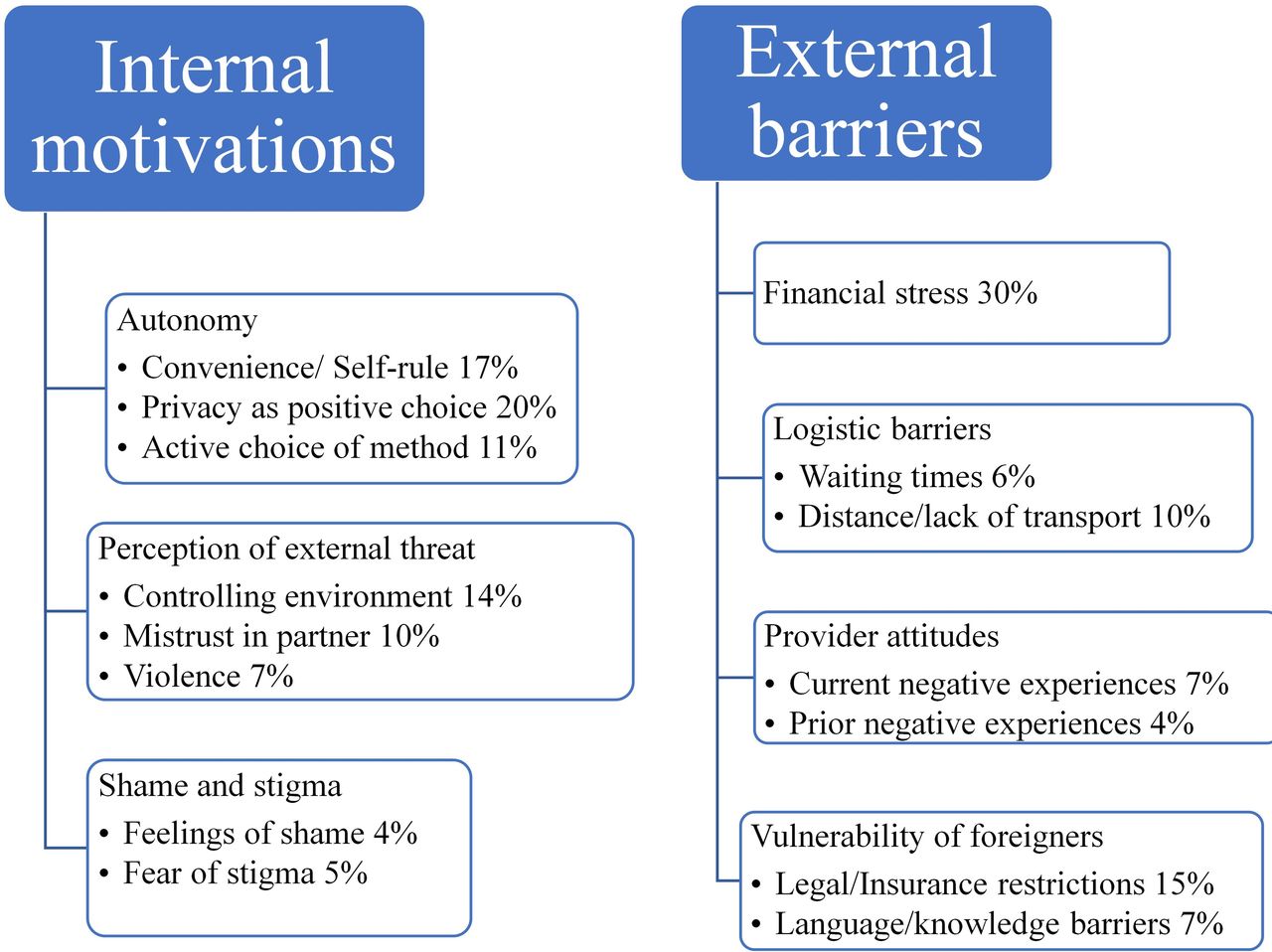
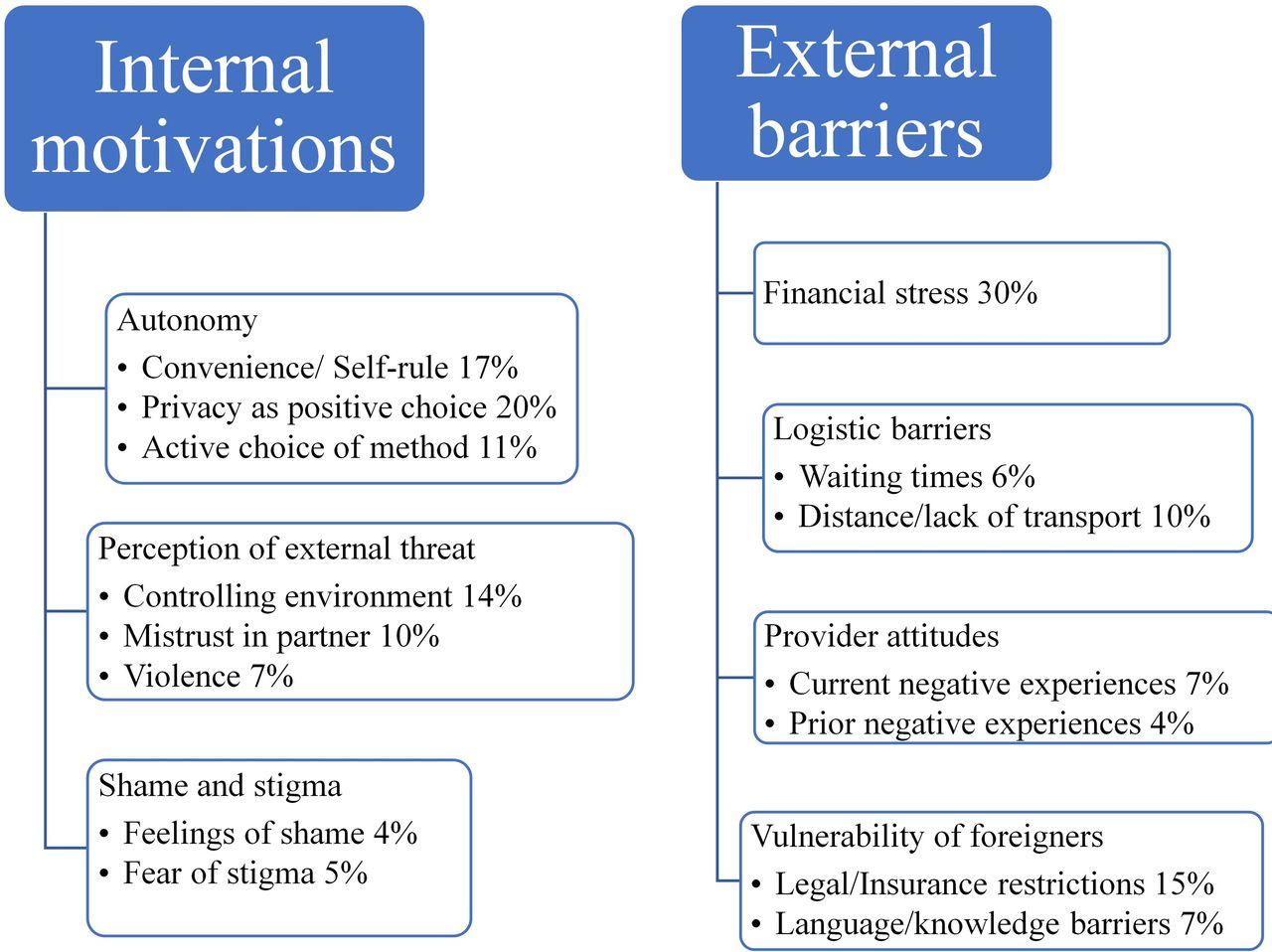
We developed two main themes and seven categories subsidiary to these themes: (1) internal motivations for seeking telemedicine abortion encompassing (i) autonomy, (ii) perception of external threat and (iii) shame/fear of stigma, and (2) external barriers to formal abortion care encompassing (iv) financial stress, (v) logistic barriers to access, (vi) provider attitudes and (vii) the vulnerability of foreigners. A scheme of themes, categories and subcategories is shown in figure 2.
{kind=link}
{kind=link}
Schematic presentation of derived themes, categories and subcategories with corresponding frequencies from 108 emails sent from Germany to Women on Web between 1 January and 31 December 2019 explaining the need for telemedicine abortion.
Integrated results
Autonomy
In the cross-sectional data, two frequent categorical reasons for requesting telemedicine abortion were the preference to keep the abortion private (48%) and being more comfortable at home (44%). In the content analysis, the wish for autonomy was a main internal motivation for choosing telemedicine abortion. As exemplified by the quote below, women described privacy as a positive choice, and the desire to choose where, when and with whom to perform the abortion.
I do not want to go the 'normally' way because my family will notice. I have extensively informed in the Internet about the pros and cons. I'm sure it’s the right decision for me. I do not want to have to discuss within the family about something that mainly concerns me.
Perception of external threat
The need to keep the abortion a secret from a family or partner was a frequent reason for requesting telemedicine abortion in the cross-sectional data (48%) and 5% of women reported living in an abusive relationship. Adolescents (≤18 years) were more likely to report the need to keep the abortion a secret (OR 2.78, 95% CI 1.59 to 4.87).
Secrecy because of a perceived threat from the family or community was also an internal motivation in the content analysis. Over a third of women described living in a controlling environment, as exemplified below:
The problem is my partner. We live and work together, which means that I do not have the opportunity to go to the consultation let alone to the doctor’s practice without being noticed. […] I am afraid he might hit me or push me against the furniture again. I would do it [the abortion] differently, but I am not able to do anything without him noticing. [translation]
In their consultation forms and email texts 6% of women reported having been raped. Rape was sometimes, as exemplified below, described as exacerbating the shame associated with the abortion:
I was raped. I live in Germany but cannot officially have an abortion. If somebody sees me in a different part of town it would be a catastrophe. […] If I disclose the rape and communicate with my family, then everything will be worse. They would not believe me. [translation]
Shame and fear of stigma
Some 37% of women in the cross-sectional study reported fear of stigma. Fear of stigma was further associated with living in a small town (OR 1.47, 95% CI 1.12 to 1.94) and being an adolescent (OR 1.81, 95% CI 1.08 to 3.01). In the content analysis, we found that self-recrimination and shame for the unwanted pregnancy were internal motivations for requesting telemedicine abortion. In the words of one woman:
[…] I feel very ashamed at the thought of discussing or rather sharing my decision to abort with so many people, that I do not know. I have the feeling that one will indirectly judge me and this, in combination with the thought of having the abortion carried out by the same people, feels unbelievably difficult and wrong to me.
Financial stress
Financial hardship was a barrier to abortion access of similar frequency in the cross-sectional study (40%) and the content analysis (30%). Adolescents were more likely to name cost as barrier (OR 2.61, 95% CI 1.51 to 4.5).
In their emails women described not being able to afford the out-of-pocket expenditure, not being able to afford to take days off work, and/or not meeting the criteria for the reimbursement of the abortion through the social welfare system.
Logistic barriers
In their consultation forms and emails women often described multiple logistic barriers such as waiting times, distance, work/childcare commitments and complicated bureaucracy. One woman described the complexity of the barriers facing her as follows:
I cannot get a doctor’s appointment. I cannot drive hundreds of kilometres, wait for weeks. I need to take care of my children, go to work. The next hospital, which does abortions, is 2 hours away. How am I supposed to do that? How will I get there? Where shall I leave my children during that time? [translation]
Provider attitudes
Some women described prior experiences of abortion care as their reason for choosing telemedicine abortion such as negative persuasion efforts, judgemental comments, delayed approval for abortion, or a pointed lack of assistance with the formal requirements.
One woman recounted:
Since I already had an abortion 3 years ago I know what kind of gauntlet I would have to expect. I cannot cope with this one more time.
Vulnerability of foreigners
In the emails 9% self-identified as undocumented immigrants and 21% reported difficulties related to being a foreigner. These women described being denied access to services, language barriers, lack of knowledge about a complex and highly regulated system, and fear of having their immigration status revealed, often in the context of financial hardship and controlling or threatening environments. Adolescents, without specified immigration status, were more likely to report legal restrictions to access (OR 2.82, 95% CI 1.63 to 4.9).
Discussion
This study suggests that there is a demand for alternatives to formal abortion services in Germany. Women who choose telemedicine abortion do so both from a place of empowerment, expressed as a desire for autonomy, and from a place of disempowerment, expressed as perceived barriers and fear of repercussions if the abortion were known about.
Attitudes, knowledge and confidence
The concept of access with respect to abortion is multifaceted and depends not only on legal prerequisites but on women’s attitudes, knowledge and confidence in obtaining services as well as the service delivery itself.9
The agency to make an informed choice is fundamental to empowerment in sexual and reproductive health and rights.10 11 Women in the study who described a personal preference for telemedicine abortion had often researched their options and knew why it was a good choice for them. A previous study has shown that women who opt for an abortion in the informal sector, also in countries where abortion is available through formal channels, often do so for reasons of privacy and self-management.3
In contrast, over a third of women in this study lived in environments that limited their ability to make choices about their sexual and reproductive health, forcing them to keep the abortion a secret. Many of these women were in abusive relationships. Concealing a pregnancy or abortion from a partner is known to be associated with inter-partner violence.12
Many women in the study directed feelings of shame and blame about the abortion towards themselves. The systematic blaming of women in cases of sexual- or gender-based violence, or negative outcomes of pregnancy, is termed “gendered blame” and is applicable also to unwanted pregnancy and abortion.13
Service delivery
Cost of services was a significant barrier to access in the study, consistent with a previous study from the US.14 Compared with the US, Germany has a strong public insurance system and extensive social welfare programmes but abortions without medical indication are not routinely covered.15 The exemption of abortion from publicly financed health reflects a low prioritisation of abortion rights.
In our results it was often the compounded effect of multiple logistic barriers that made abortion inaccessible. In a study from Great Britain, barriers to abortion were suggested to result from underfunding of health services in general, also impacting abortion services.16 In Germany, however, waiting times for clinical appointments other than abortion are shorter than in other high-income countries.17 This raises the question of specific underfunding of sexual and reproductive health and rights in Germany.
A proportion of women in the study also described negative experiences that reflect on abortion service delivery. A study in Hungary found that negative experiences with providers and fear of stigma were the main reasons women sought alternative abortion care options.18 Research supports that legalised access to abortion is difficult to enact successfully in the context of stigmatised services.19
Undocumented immigrants in the study described formal and informal difficulties accessing abortion. Undocumented immigrants within their first 15 months of stay receive only care for acute, pregnancy- or child-related health issues, excluding abortion, which makes elective interventions like abortion and family planning routinely impossible.20 This policy resembles that of Switzerland, where undocumented immigrants show significantly higher rates of unintended pregnancies than women with documented status.21
Policy implications
Abortion-related stigma persists in German laws and policies, and abortion care provision suffers from complicated bureaucracy and lack of transparency.4 5 The allowance of conscientious objection is known to increase the risk of judgemental treatment.15 22
Our results indicate that groups at particular risk of missing out on access are women with low financial means, undocumented immigrant women, and adolescents, where a particularly vulnerable group may be undocumented adolescent immigrants. Being young per se was not identified as a barrier to access but adolescents were more likely to report lack of finances, need for secrecy, and legal restrictions compared with older women. German law requires parental consent for girls below the age of 16 years, which is in practice often applied to girls under 18 years, something which must be recognised as a barrier to access.4
Abortion care reform in Germany requires a simplified care process, targeted interventions for vulnerable groups, and sensitisation of healthcare providers towards non-judgemental care. Even countries that formally provide elective abortion must recognise that barriers to access in the form of scarce service delivery, stigma, prohibitive cost, or requirements of multiple appointments are enough to seriously affect women’s health and rights.23 24
Study strengths and limitations
The motivations of women who seek abortion care outside the formal sector in Germany is a topic that has not been researched. The data represented a large sample, used mixed methods which enabled triangulation, and reached information saturation.
The content analysis, based on the response to a single question, would have been nuanced by in-depth interviews. Our findings cannot make an overall assessment of abortion service delivery in Germany. A broader survey among women and providers in Germany is required to describe the gaps in the current service delivery.
Conclusions
Our study indicates that women in Germany who choose telemedicine abortion outside of the formal health sector do so both from a place of empowerment and a place of disempowerment. Numerous barriers exist to abortion access in the formal health sector and these may most impact vulnerable groups such as adolescents, women with low financial means, and undocumented immigrants.
Data availability statement
All original data are available upon reasonable request to the researchers.
Ethics statements
Patient consent for publication
Ethics approval
Ethics Committee Karolinska Institutet Dnr 2009/2072-31/2 and Dnr 2020/05406
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors participated in the design of the study. KK performed the quantitative analysis and KK and SG performed the qualitative analysis. ME supervised the study analysis. ME and KK wrote the article manuscript. All authors participated in the discussion of the results and approved the final version of the manuscript.
Funding This study was funded by the Swedish Society of Medicine.
Competing interests Coauthors RG, SG and HA work for or are affiliated with Women on Web.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.